Chronic contained rupture of the abdominal aortic aneurysm presents a high risk of progression to free rupture which carries a high mortality rate, therefore urgent management is essential. We present a case of an 80-year-old woman with lower abdominal pain 6 months earlier that spontaneously remitted. A contrast-enhanced computed tomography indicated a contained ruptured abdominal aortic aneurysm. Patient reported worsen abdominal pain leading to hospitalization 30 days after first evaluation. Due to patient comorbidities and exclusion of other pain causes, urgent endovascular treatment with chimney technique was indicated. After several attempts to cannulate the left renal artery through the trans-axillary access without success, we applied the previously described "lift" technique for transfemoral creation of an up-facing snorkel branch to the left renal artery as a bailout strategy to preserve the left kidney. The aneurism was successfully treated, and all visceral branches preserved. The patient was discharged 3 days after surgery.
Chronic contained rupture, Endovascular repair, Abdominal aorta, Pararenal aneurysm, Stent-graft, Chimney graft, Chimney technique, Lift technique
Abdominal aortic aneurysms are defined as an aortic diameter of more than 3 cm. Its rupture is associated with high mortality rates. The single most important predictor of rupture is the diameter of the aneurysm, with the risk increasing with larger aneurysms [1]. Rarely, ruptured abdominal aortic aneurysm (rAAA) may be effectively "sealed off" by the surrounding peritoneum, which leads to a "chronically" contained retro-peritoneal hematoma resulting in a chronic contained rupture of the abdominal aortic aneurysm (CCR-AAA) [2]. Proper treatment depends on distinction between CCR-AAA and free rAAA [3]. CCR-AAAs have a high risk to progress to free rupture which carry a high mortality rate, therefore urgent management is essential, however, if diagnosed and managed properly, they have comparable morbidity and mortality rates compared to elective interventions [3]. Treatment options include either open aortic repair (OAR) or endovascular aortic repair(EVAR) [4]. Endovascular techniques are less invasive methods of treating infrarenal abdominal aortic aneurysms (AAAs) especially for patients with severe comorbidities [5]. Endovascular aortic repair with parallel stents in the visceral arteries [6], the chimney technique (ChEVAR), is an important treatment option in high-risk patients with o juxtarenal (JRAAA), pararenal (PRAAA), and Crawford type IV thoraco-abdominal (TAAA) aneurysms [7,8]. However, this method requires selective catheterization of the target vessels through the subclavian or axillary artery, which may be hazardous or challenging in several situations [7]. We report a case of a pararenal chronic contained ruptured abdominal aortic aneurysm using the "lift" technique as a bailout strategy to preserve the left renal artery due to challenging antegrade catheterization.
An 80-year-old woman referred to our hospital for evaluation due to pulsatile abdominal mass and chronic abdominal pain. She reported having perceived intense lower abdominal pain 6 months prior the initial examination, but it spontaneously remitted. Her medical history was remarkable for known cardiovascular disease, chronic obstructive pulmonary disease (COPD) with a 36 pack-year history of tobacco use, hypertension, stage 3 chronic renal insufficiency (Cr 1,39 Ur 42 BUN 19,6) and hyperlipidemia. She had no known history of aortic aneurysm. On initial assessment the patient's vital signs were stable. A pulsatile abdominal mass was palpable, but no pain related on physical examination. A blood test revealed no anemia, thrombocytopenia, or coagulation abnormalities. Computed tomographic angiography (CTA) revealed a pararenal abdominal aortic aneurysm, with a maximum diameter of 5.1 cm, with a large, poorly enhancing soft tissue mass (6.7 × 5.1 cm) arising from and continuous with the left anterior-lateral aspect of the aneurysm. The features were suggestive of a CCR-AAA (Figure 1, Figure 2, Figure 3 and Figure 4). Patient reported severe abdominal pain leading to hospitalization 30 days after first evaluation. Due to patient's comorbidities, an endovascular approach was considered. A ChEVAR was then planned.
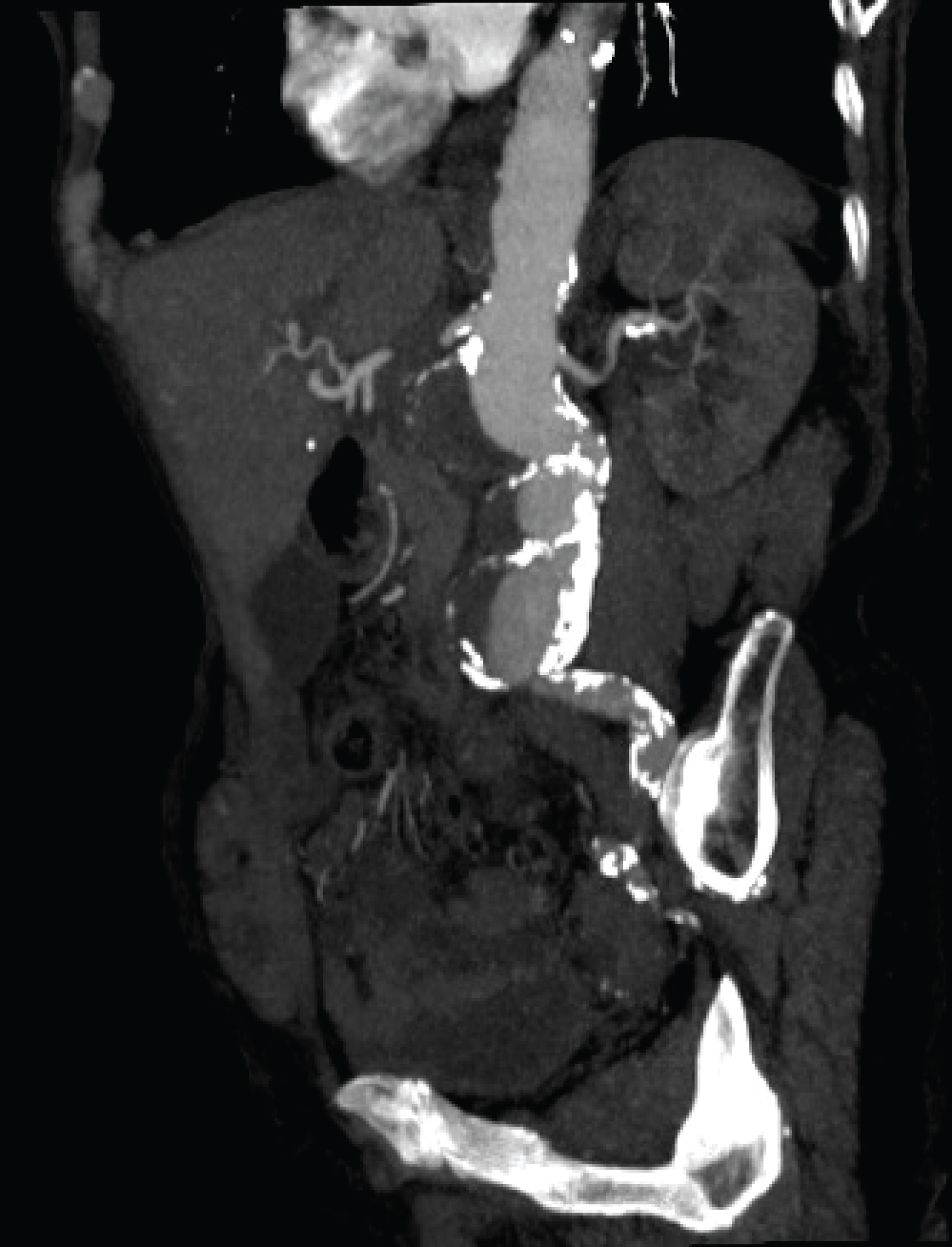 Figure 1: CTA show the Pararenal abdominal aortic aneurysm.
View Figure 1
Figure 1: CTA show the Pararenal abdominal aortic aneurysm.
View Figure 1
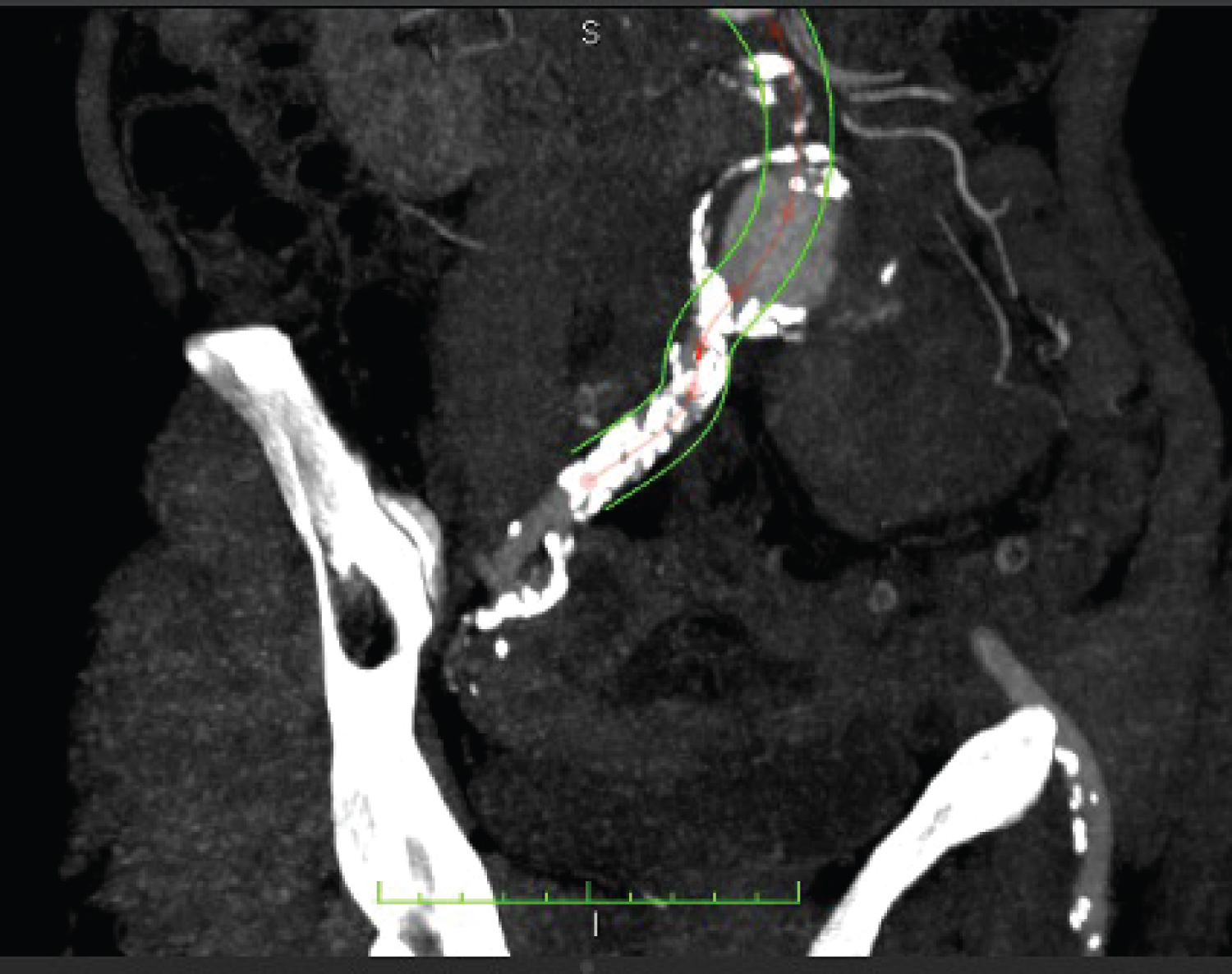 Figure 2: CTA - coronal reconstruction showing anterior CCR-AAA with hematoma outside the rim of calcification.
View Figure 2
Figure 2: CTA - coronal reconstruction showing anterior CCR-AAA with hematoma outside the rim of calcification.
View Figure 2
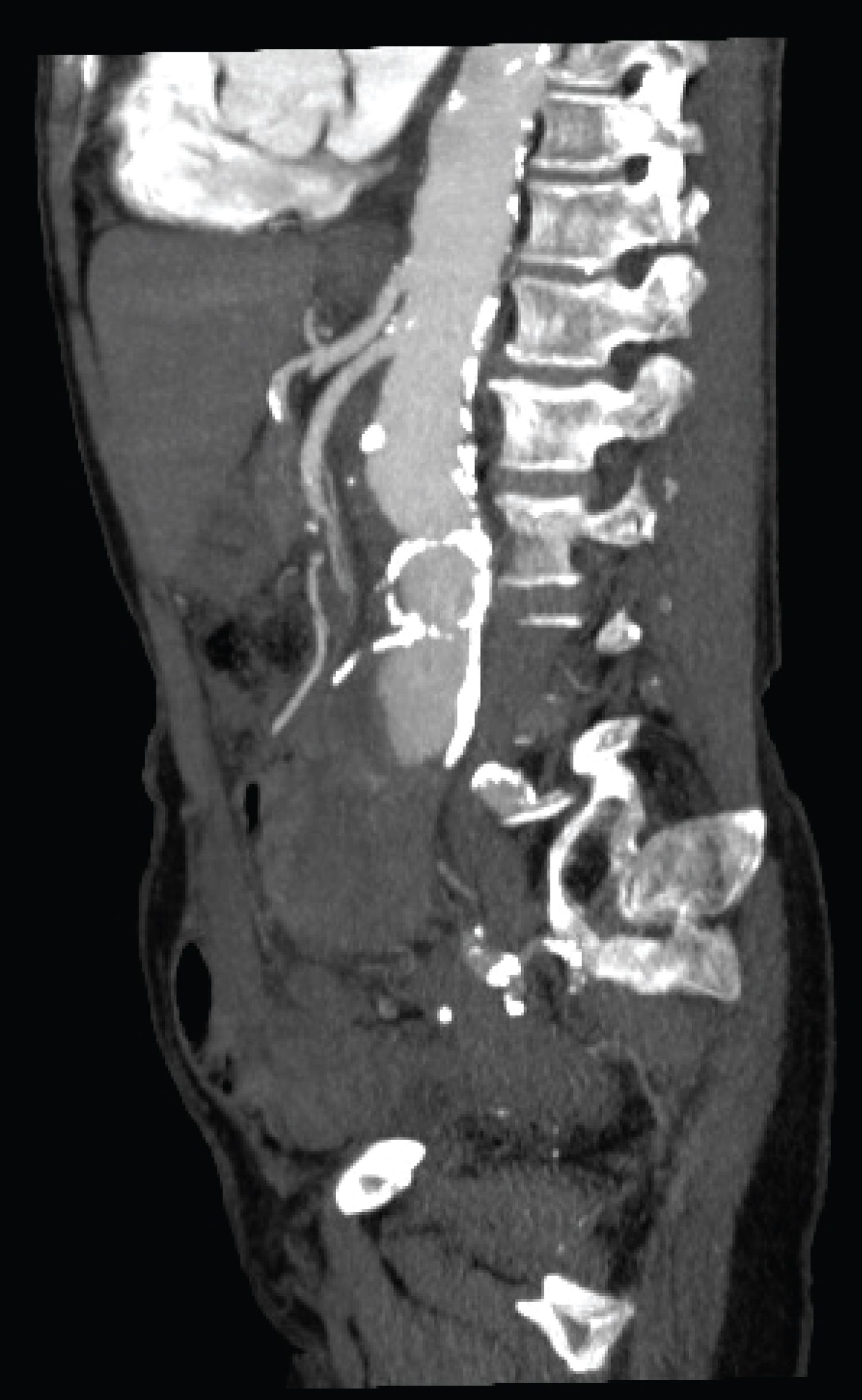 Figure 3: CTA - sagital reconstruction showing anterior CCR-AAA with hematoma outside the rim of calcification.
View Figure 3
Figure 3: CTA - sagital reconstruction showing anterior CCR-AAA with hematoma outside the rim of calcification.
View Figure 3
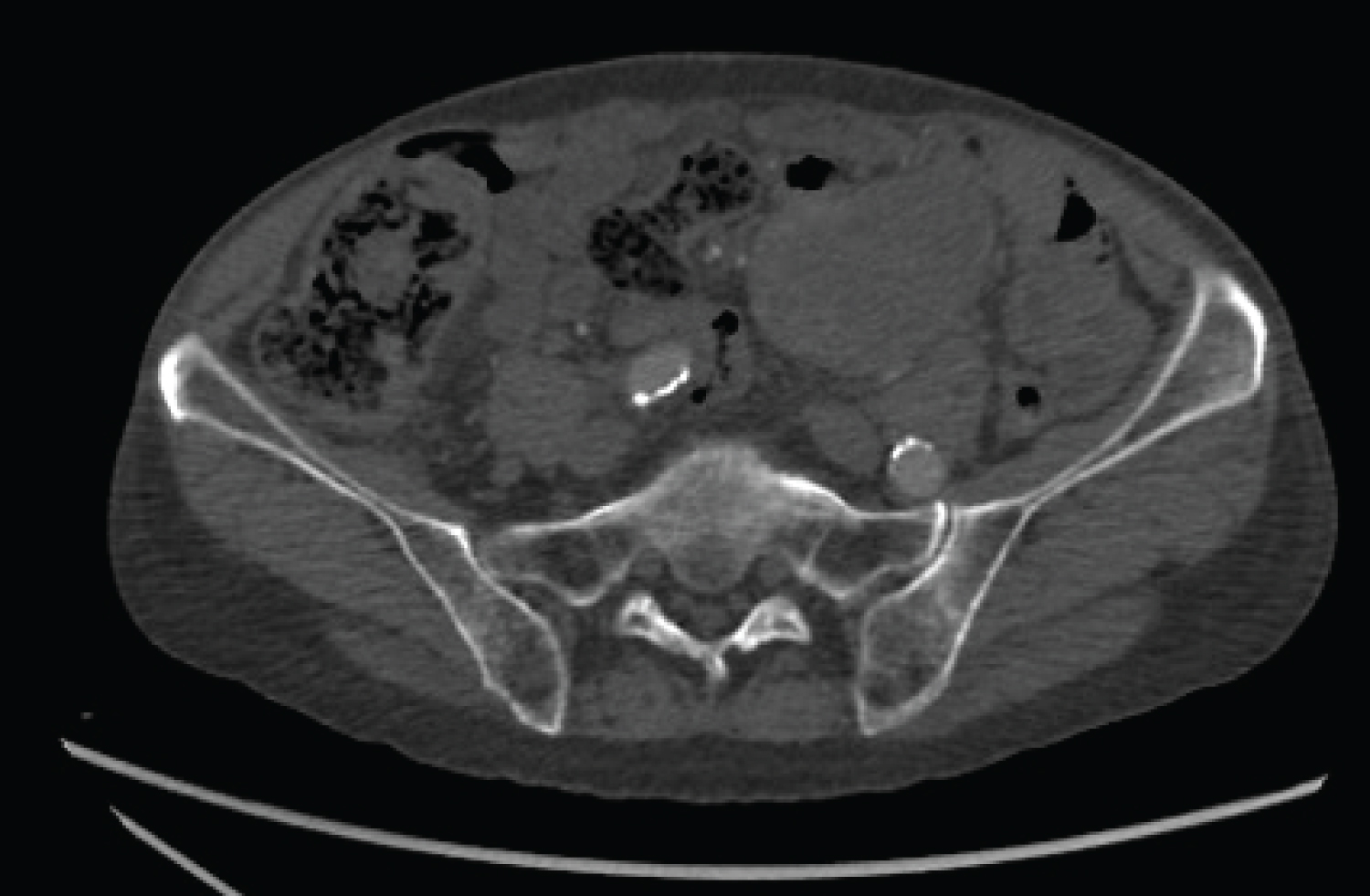 Figure 4: CT showing abdominal aortic aneurysm with large extra-mural mass extending into anterior-left flank.
View Figure 4
Figure 4: CT showing abdominal aortic aneurysm with large extra-mural mass extending into anterior-left flank.
View Figure 4
Surgical exposures of both common femoral arteries (CFA) were obtained, after which, surgical exposures of the right axillary arteries (RAA) and left axillary arteries (LAA) were performed. Digital subtraction angiogram (DSA) showed, a pararenal aneurysm with no leak of contrast (Figure 5). After systemic heparinization, one 8.5 Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) was inserted into the LAA and an 8.5Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) sheath into the RAA. Both sheaths were advanced into the distal descending thoracic aorta. The right renal artery (RRA) was cannulated from the LAA, employing a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.). Sequentially, the 0.035 Road Runner wire (Cook Medical, Inc.) were exchanged to a 0.035 Rosen wire (Figure 6). After several attempts to cannulate the left renal artery (LRA) through the trans-axillary access without success, we planned to apply the previously described "lift" procedure for transfemoral creation of an up-facing snorkel branch to the LRA as a bailout strategy to preserve the left kidney. The superior mesenteric artery (SMA) was temporarily cannulated with a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.) from the left axillary access site (Figure 7). One 8.5Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) was inserted into the right common femoral artery (RCFA). The sheath was advanced into the distal descending thoracic aorta and LRA cannulation was attained employing a 5-F Vert catheter, and a 0.035 Road Runner wire (Cook Medical, Inc.). Sequentially, the 0.035 Road Runner wire (Cook Medical, Inc.) were exchanged to a 0.035 Rosen wire (Figure 7). The 6 × 100 mm Viabahn® stent graft (W.L. Gore & Associates, Inc.) was advanced from the RCFA within the LRA then positioned and deployed with the distal end ~ 2 cm into the vessel (Figure 8). A 0.035 Rosen wire was advanced and positioned in the initial ~ 3 cm of the 6 × 100 mm Viabahn® stent graft (W.L. Gore & Associates, Inc.). The 8.5 Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) was advanced along with the 0.035 Rosen wire up into the thoracic aorta "lifting" the proximal end of the stent into an up-facing snorkel position (Figure 9a, Figure 9b, Figure 9c and Figure 9d). Another 6 × 100 mm Viabahn® stent graft (W.L. Gore & Associates, Inc.) was advanced from the RAA, within the RRA then positioned and deployed with the distal end ~ 2 cm into the vessel on an up-facing snorkel position. Sequentially, the 8.5 Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) from the RCFA was exchanged to a delivery system 18 Fr × 33 cm Dryseal Flex (W.L. Gore & Associates, Inc.) for the main body, and a delivery system 12 Fr × 33 cm Dryseal Flex (W.L. Gore & Associates, Inc.) for the contralateral iliac extension was placed in the left common femoral artery (LCFA). A 28.5 mm × 14.5 mm × 14 cm C3 Excluder® main body (W.L. Gore & Associates, Inc.) was advanced to the level of the renal arteries. The Endograft was semi deployed to enable maneuverability. After position confirmation the C3 Excluder's main body was fully deployed. A DSA showed the presence of a delayed low flow type Ia endoleak. New balloon dilatation of aortic graft was performed as prompt corrective treatment with no significant diminution of the endoleak (Figure 10). A 32 × 45 mm aortic cuff (W.L. Gore & Associates, Inc.) was then deployed at the level of the SMA, through the RCFA. Two iliac limb extensions were deployed from the femoral access (right side: Gore Excluder® iliac-limb 14 × 100 mm graft; left side: Gore Excluder® iliac-limb 12 × 100 mm graft (W.L. Gore & Associates, Inc.)) to complete the ChEVAR. The procedure was then finalized ballooning of the docking zone to achieve complete expansion of the aortic graft especially in the overlapping areas. Final DSA showed patency of all grafts and visceral branches, the aneurysm was satisfactorily excluded with significant diminution of the Ia endoleak (Figure 11). Catheters were withdrawn, and artery access sites, both femoral and axillar, were treated with Prolene 6-0 suture.
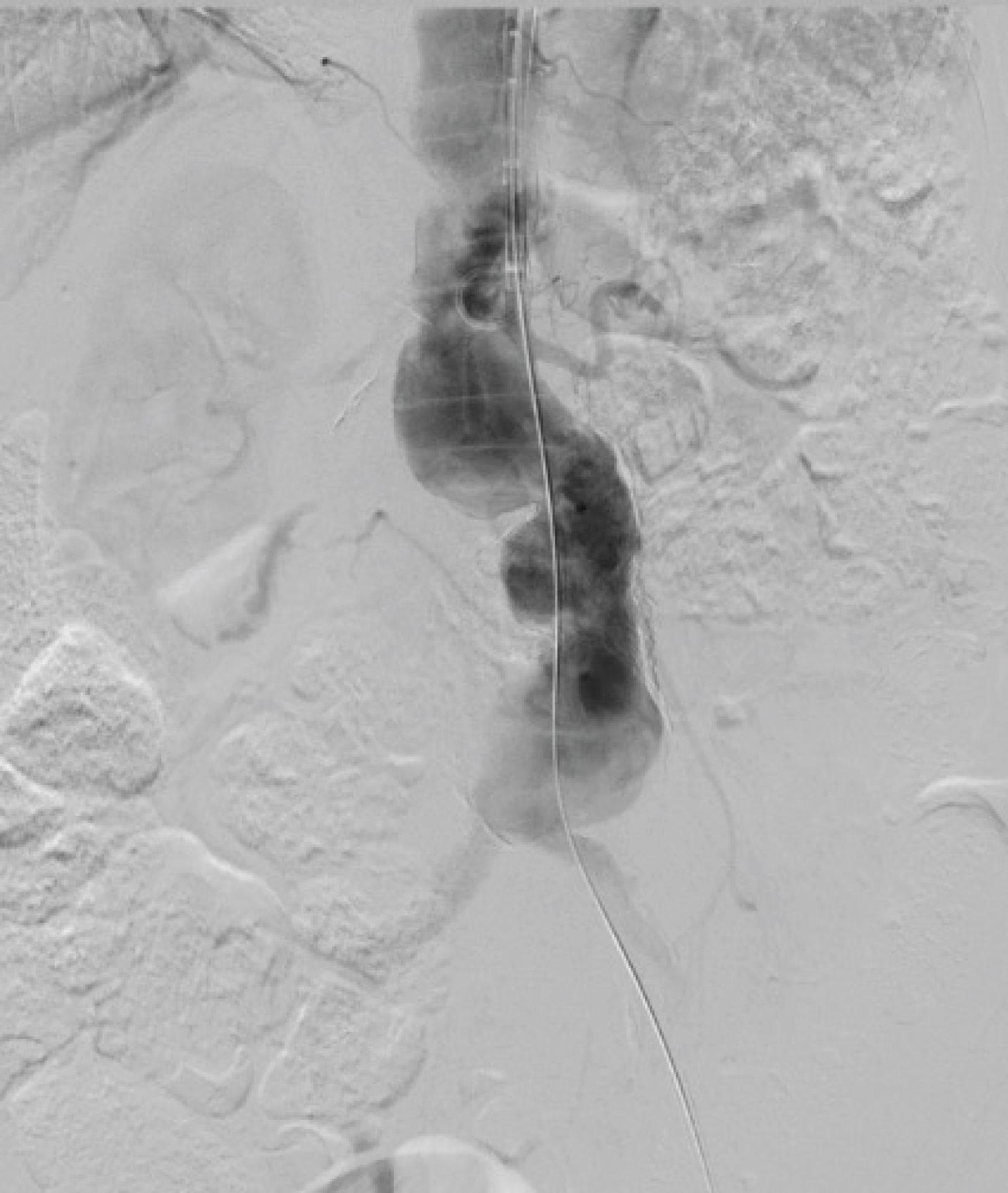 Figure 5: DSA show preoperatively, a pararenal aneurysm.
View Figure 5
Figure 5: DSA show preoperatively, a pararenal aneurysm.
View Figure 5
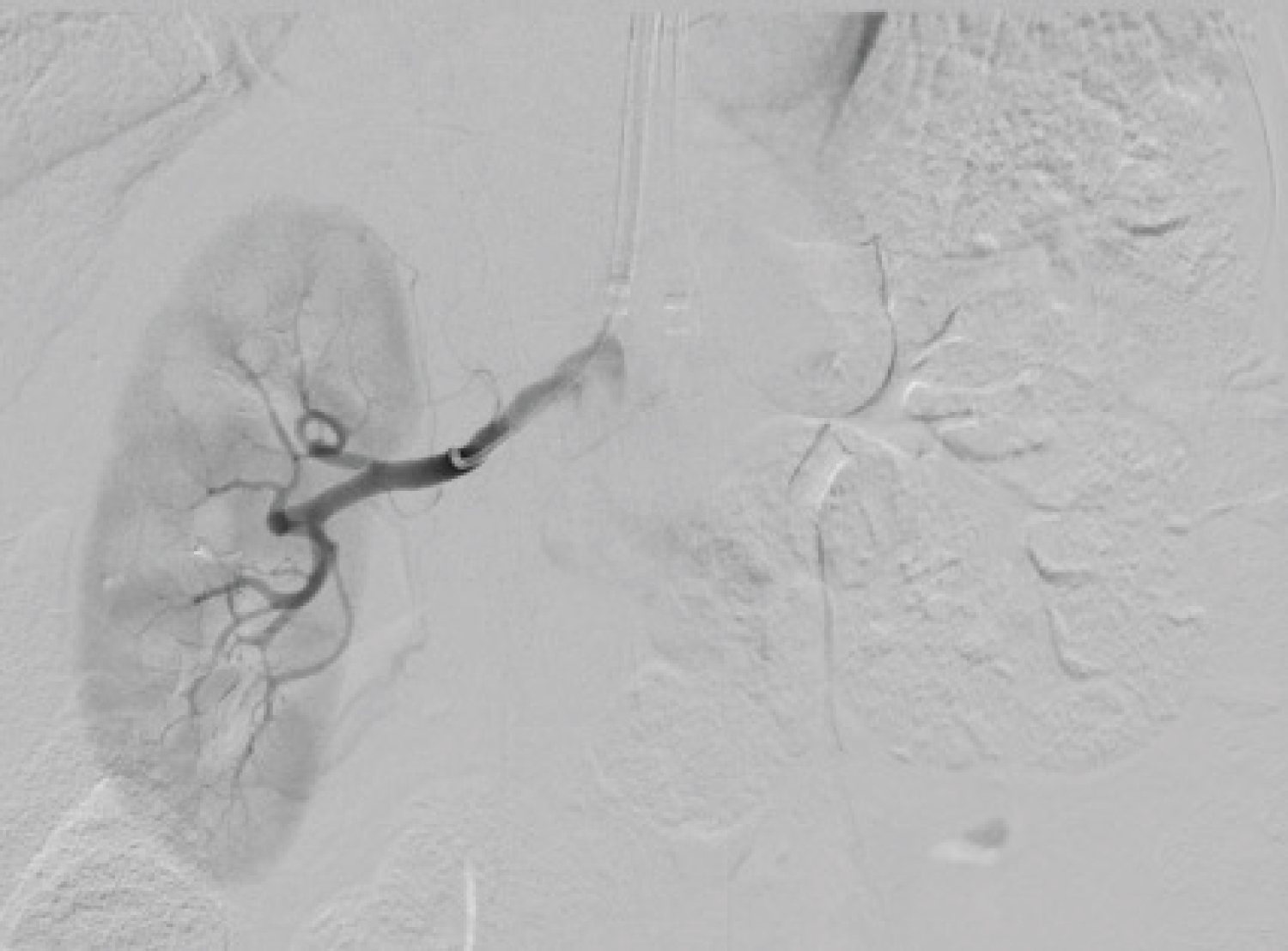 Figure 6: The right renal artery was cannulated from the right axillary artery, employing a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.).
View Figure 6
Figure 6: The right renal artery was cannulated from the right axillary artery, employing a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.).
View Figure 6
 Figure 7: The superior mesenteric artery was temporarily cannulated with a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.) from the left axillary access site. The left renal artery was cannulated from the right femoral artery, employing a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.).
View Figure 7
Figure 7: The superior mesenteric artery was temporarily cannulated with a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.) from the left axillary access site. The left renal artery was cannulated from the right femoral artery, employing a 5-F Vert catheter and a 0.035 Road Runner wire (Cook Medical, Inc.).
View Figure 7
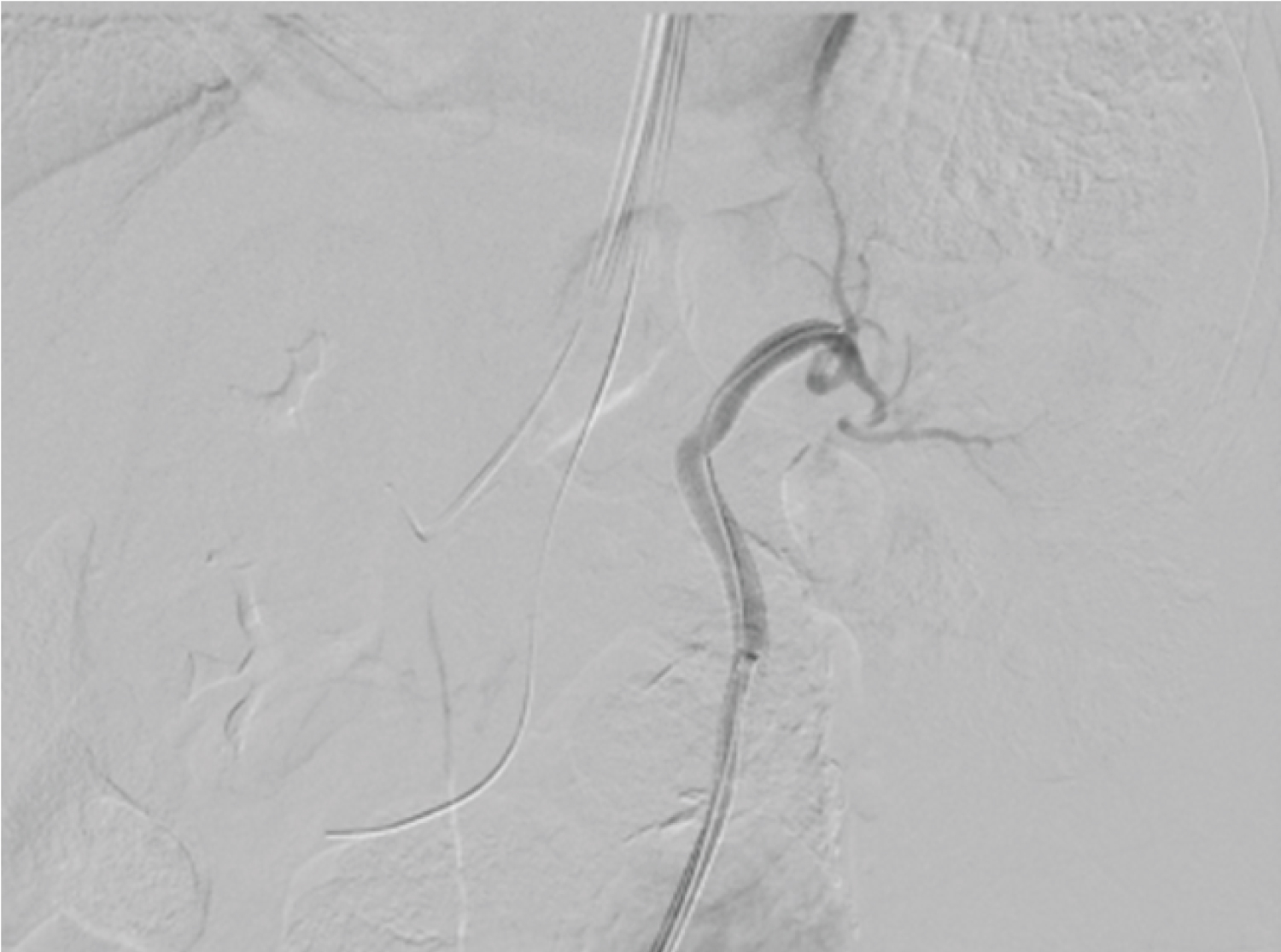 Figure 8: The 6 × 100 mm Viabahn® stent graft (W.L. Gore & Associates, Inc.) was advanced from the right femoral artery, within the left renal artery then positioned and deployed with the distal end ~2 cm into the vessel.
View Figure 8
Figure 8: The 6 × 100 mm Viabahn® stent graft (W.L. Gore & Associates, Inc.) was advanced from the right femoral artery, within the left renal artery then positioned and deployed with the distal end ~2 cm into the vessel.
View Figure 8
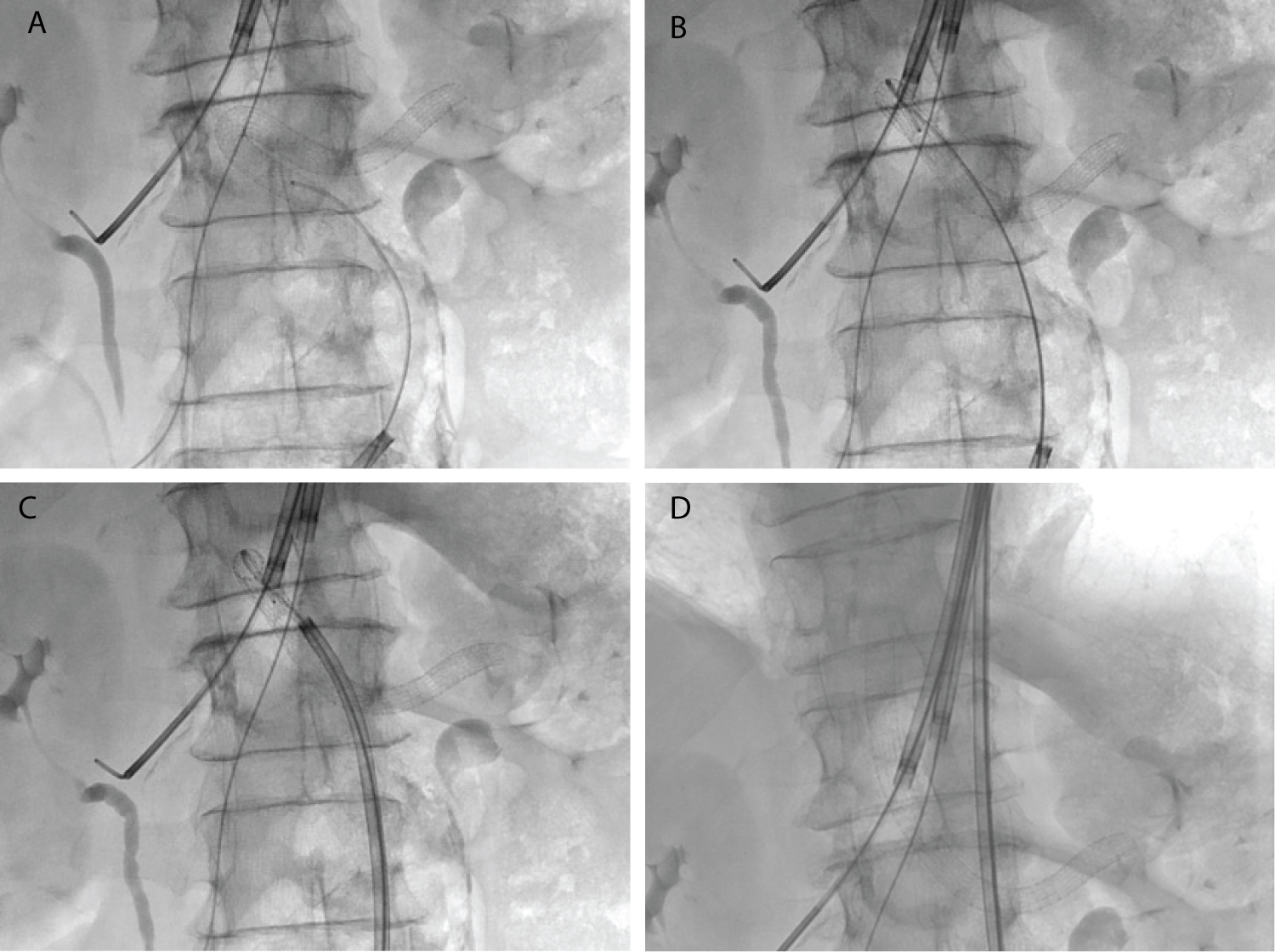 Figure 9: (a) A 0.035 Rosen wire was advanced and positioned in the initial ~3 cm of the 6 × 100 mm. Viabahn® stent graft (W.L. Gore & Associates, Inc.); (b) The 0.035 Rosen wire was advanced up into the thoracic aorta; (c) The 8.5 Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) was advanced along with the 0.035 Rosen wire up into the thoracic aorta "lifting" the proximal end of the stent into an up-facing snorkel position; (d) Stent into an up-facing snorkel position.
View Figure 9
Figure 9: (a) A 0.035 Rosen wire was advanced and positioned in the initial ~3 cm of the 6 × 100 mm. Viabahn® stent graft (W.L. Gore & Associates, Inc.); (b) The 0.035 Rosen wire was advanced up into the thoracic aorta; (c) The 8.5 Fr × 71-cm Speed Cross MSB Twist (Medical System do Brasil, ltda.) was advanced along with the 0.035 Rosen wire up into the thoracic aorta "lifting" the proximal end of the stent into an up-facing snorkel position; (d) Stent into an up-facing snorkel position.
View Figure 9
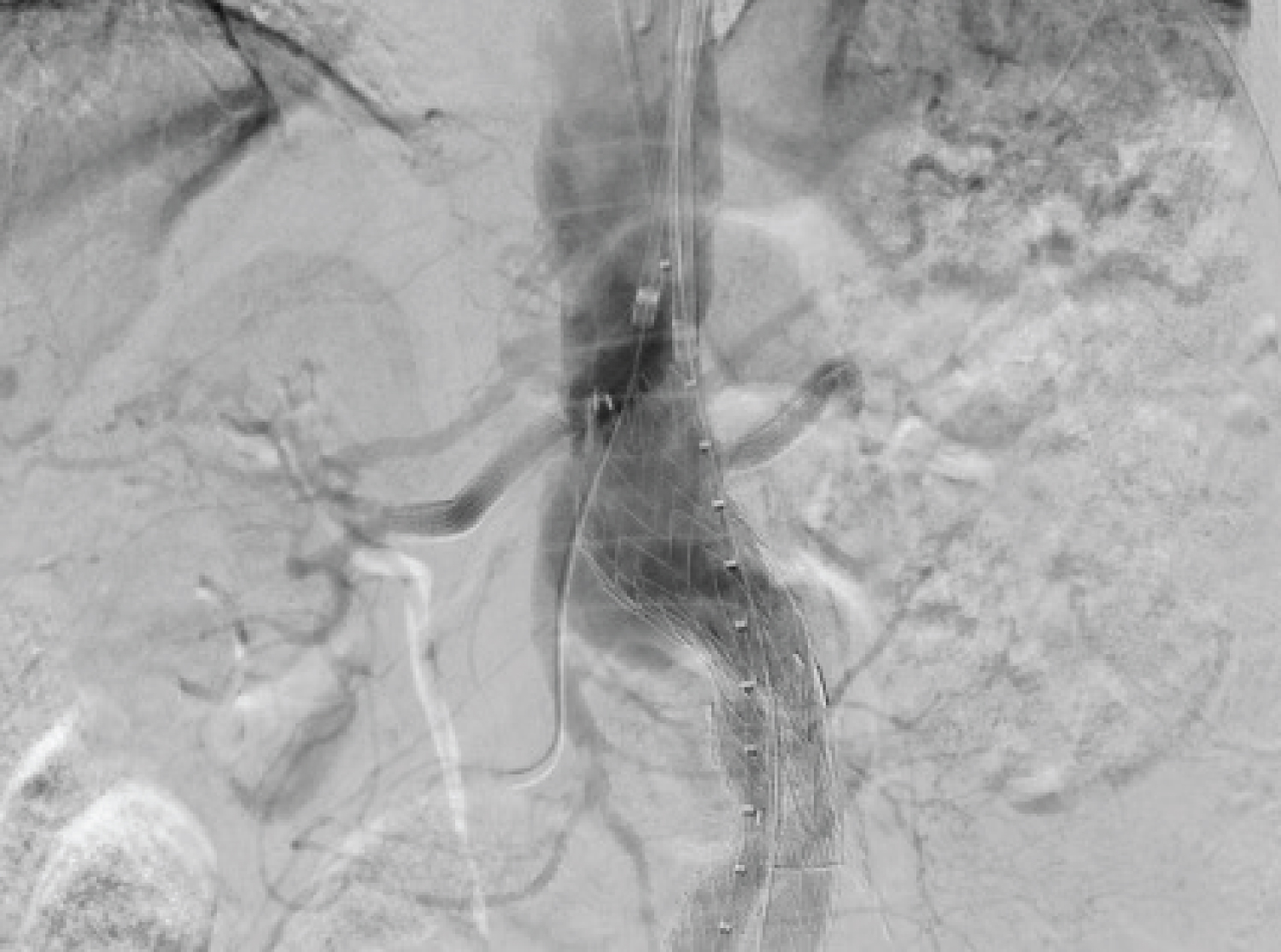 Figure 10: A 28.5 mm × 14.5 mm × 14 cm C3 Excluder® (W.L. Gore & Associates, Inc.; Flagstaff, Az) main body was advanced to the level of the renal arteries. After position confirmation the C3 Excluder's main body was fully deployed. Intraoperative fluoroscopic images show the presence of a delayed low flow type Ia endoleak.
View Figure 10
Figure 10: A 28.5 mm × 14.5 mm × 14 cm C3 Excluder® (W.L. Gore & Associates, Inc.; Flagstaff, Az) main body was advanced to the level of the renal arteries. After position confirmation the C3 Excluder's main body was fully deployed. Intraoperative fluoroscopic images show the presence of a delayed low flow type Ia endoleak.
View Figure 10
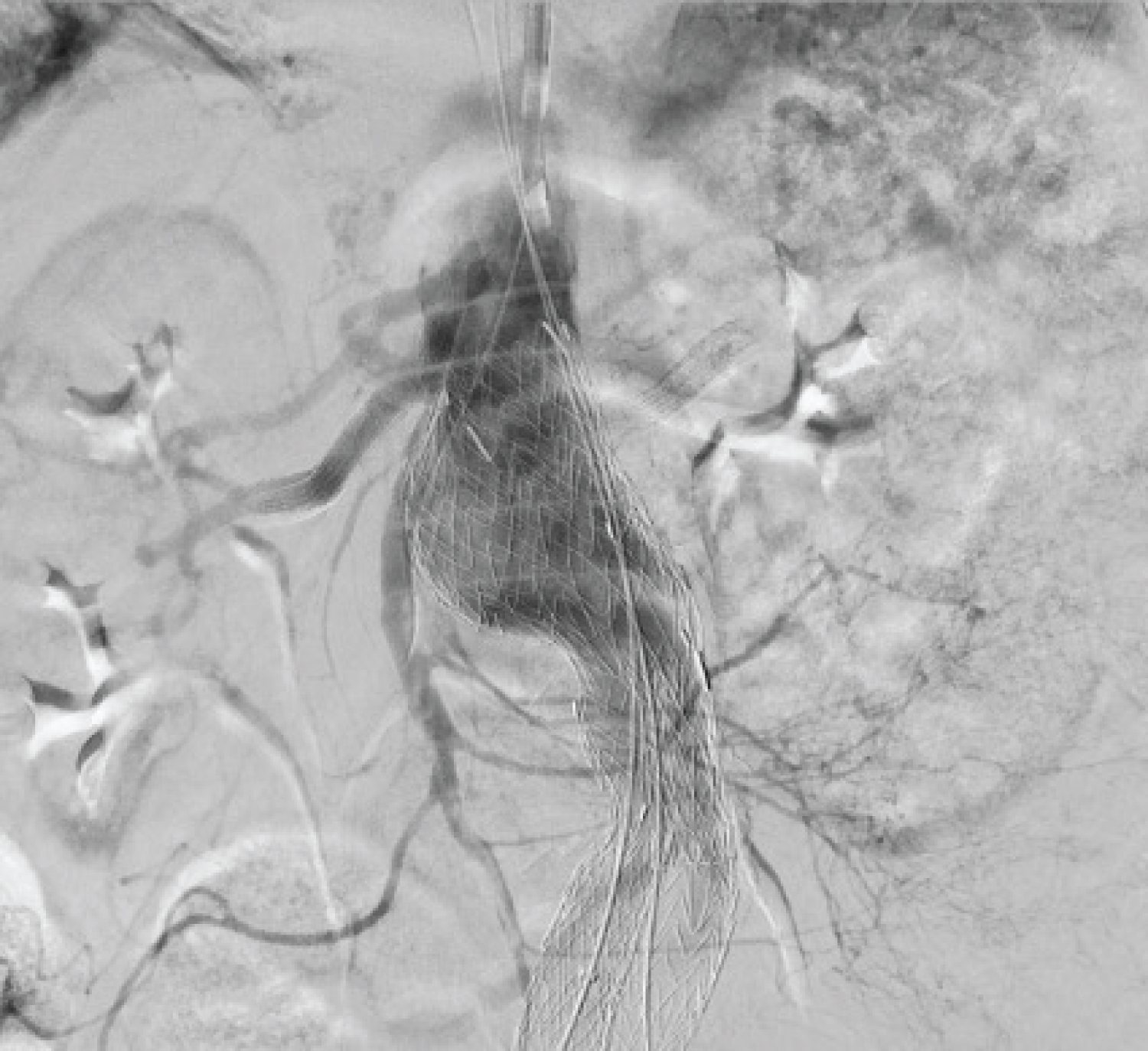 Figure 11: Final fluoroscopic images show all grafts and visceral branches were patent, the aneurysm was satisfactorily excluded with significant diminution of the endoleak after the deployment of the 32 × 45 mm aortic cuff (W.L. Gore) at the level of the superior mesenteric artery.
View Figure 11
Figure 11: Final fluoroscopic images show all grafts and visceral branches were patent, the aneurysm was satisfactorily excluded with significant diminution of the endoleak after the deployment of the 32 × 45 mm aortic cuff (W.L. Gore) at the level of the superior mesenteric artery.
View Figure 11
The patient was discharged on postoperative day 3 with renal function during discharge (Cr 1.82; Ur 67 and BUN 31.27) and on dual antiplatelet therapy. On subsequent surveillance USG, the stented aortic segment showed signs of favorable aortic remodeling with false lumen thrombosis and decreased maximum transaortic diameter associated with patency of the grafts and visceral branches.
CCR-AAA is a rare condition which represents 2.7% to 4% of all operated infra-renal AAAs [9,10]. It was first reported by Szilagyi, et al. in 1961 and [10] it's characterized by low blood loss and stable hemodynamics, which are due to hemostasis by the retroperitoneum tissue when the aortic aneurysm ruptures [11].
CCR-AAAs may present with different symptoms which are usually indefinite and resulted from compression to the nearby structures rather than changes in the patient's hemodynamics. Clinical stability of patients for long periods usually resulted in a delayed diagnosis [12].
CTA is a useful modality for diagnosing CCR-AAA; it shows a well- defined soft-tissue density mass, adjacent to the aortic wall usually with no contrast effect inside [13]. There may be a breach in calcification in the aortic wall at the site of the rupture. Recurrent leaks will lead to a "onion skin" appearance [14]. Another typical CTA sign is the "draped aorta" sign. The posterior wall of the aorta drapes along the contour of the adjacent vertebral body and becomes indistinct from the surrounding structures [15,16].
The diagnostic criteria for CCR-AAA consist of the following: known AAA; previous pain symptoms; stable condition and normal hematocrit; CTA showing a retroperitoneal hematoma; and pathological confirmation of an organized hematoma [13]. Diseases from which CCR-AAA must be distinguished include retroperitoneal tumors and abscess [11]. The present case met the four criteria, and we could obtain conclusive evidence indicating that the lesion observed via the CTA was a hematoma excluding other diseases or infection patterns.
PRAAA is defined as aneurysms involving the renal arteries, with or without reaching the origin of the SMA accounts for 8% to 20% and need careful planning to preserve abdominal aorta main branches [17,18].
To preserve the branches' patency, parallel graft techniques have emerged such as the Inner tubing technique [6] and the ChEVAR [8]. The use of chimney endografts increases the applicability of EVAR for challenging neck anatomies without the need for custom-made devices. It can be used as a bailout technique for accidental coverage of visceral arteries during EVAR [8,19].
The ChEVAR is based on the placement of a stent parallel to the aortic endograft and its main goal is to achieve an adequate proximal sealing zone and keep aortic branches patent through covered stent grafts [8]. Challenging anatomy, cardiovascular disease and chronic obstructive pulmonary disease are indications to consider ChEVAR [8,19,20].
As described our patient had the two mentioned comorbidities and needed urgent intervention therefore the ChEVAR seemed a valid option. Other option for non-fit patients is the Fenestrated EVAR (FEVAR) but it takes time, for precise planning and endoprosthesis customization [20]. In contrast, ChEVAR offers the advantages of immediate availability, lower cost, and lower profile for associated aortic devices. Furthermore, ChEVAR can overcome some anatomical contraindications related to FEVAR such as aortic angulation, renal or visceral ostia proximity, and target vessel orientation. ChEVAR is less complex to perform, widely available and feasible in the acute setting. On the other hand, ChEVAR requires upper limb access with a risk of embolic stroke in atheromatous aortic arches, and risks exposure to gutter related endoleaks (Type Ia) with a risk of proximal sealing failure [5,20].
Selective catheterization of the target vessels through the subclavian or axillary artery, which may be hazardous or challenging in several situations such as those involving occlusion of the subclavian or axillary artery, the type III aortic arch, post-arch replacement, and obtuse renal artery angle [9].
Placement of up-facing snorkels, delivered from a transfemoral approach, has first described by Lachat, et al. as "lift" technique and was used for renal artery stenting during endovascular repair of a PRAAA. Branch access and stent delivery from a transfemoral approach is subsequently manipulated in situ from a down-facing periscope into an up-facing snorkel that receives antegrade blood flow [9].
We successfully used the "lift" technique during ChEVAR as a bailout strategy to preserve the left renal artery. An aortic cuff was needed to treat Ia endoleak identified during the procedure.
Different from de original description of the "lift" technique. We did not used any angioplasty balloon affixing the stent-graft in the renal segment to replace the proximal end from down to up. We used just a Rosen wire to perform the "lift" technique without any migrations of the renal stent (Figure 9).
Endovascular treatment of pararenal aneurysm can be technically challenging. As such, extensive experience of the vascular surgeon in complex endovascular procedures is required. Incorporation of the "lift" technique into parallel grafting creates a platform for additional treatment of the remaining SMA and renal arteries, in challenging situations.
Funded by the authors.
No conflict of interest.