Bentall's procedure is a type of cardiac surgery to replace part of the aorta and the aortic valve of the heart because of pathological aortic conditions. Button aneurysm of coronary artery is a rare and uncommon condition following Bentall's procedure. Here, we present a case of a 29-year-old female who developed left coronary artery button aneurysm four years after Bentall's procedure for ascending aortic aneurysm. Hence, in patients with Bentall's procedure, a regular follow-up is encouraged for the timely identification of all the complications associated with Bentall's procedure.
Bentall's procedure also known as aortic valve replacement is a surgical treatment done for repairing an aortic root pathology associated with a diseased aortic valve. The procedure implies the replacement of the aortic root, valve, and the ascending aorta with a composite valve graft [1]. Bentall's procedure is recognized as a safe and long-term efficient approach in patients with aortic root and valve disease. However, as with any other surgical procedure, it also has associated complications, such as hemorrhage, thromboembolism, endocarditis, major adverse valve-related events, progressive aortic dilatation, and coronary artery root dilation resulting in button aneurysm [2]. Coronary button aneurysm is a rare but well-recognized complication whose possibility of occurrence should always be taken into account while undertaking aortic root surgery [3]. Since the presenting clinical signs and symptoms are non-specific, the preferred imaging method to diagnose the condition is CT angiography [4]. We herein present a case of a young female patient who developed a focal left main coronary artery button aneurysm following Bentall's procedure performed for ascending aortic aneurysm.
A 29-years-old female patient presented to our outpatient department with a history of dull chest pain and shortness of breath. She had no specific comorbidities except a history of undergoing surgical procedure namely Bentall's procedure four years back for a fusiform aneurysm of the ascending aorta. Provided the history of aortic valve replacement with a prosthetic valve graft, a CT aortogram was performed for the evaluation of the graft.
A 640-slice CT scanner was used to perform CT Aortogram following standard imaging protocols. Her CT Aortogram showed focal aneurysmal dilatation of the left main coronary artery at its origin, from which the Left Anterior Descending (LAD) and Left Circumflex (LCX) arteries were branching out (Figure 1). The dilated segment of the left main coronary artery was approximately 12.0 × 10.0 mm in size. The prosthetic aortic valve was noted in situ and was intact (Figure 2). No evidence of perigraft or perivalvular leakage was seen.
 Figure 1: Volume Rendering (VR) image (a) and CT soft tissue window axial view (b) showing a button aneurysm in the form of focal aneurysmal dilatation of the left main coronary artery at its origin, and its branches LAD and LCX arteries (arrows).
View Figure 1
Figure 1: Volume Rendering (VR) image (a) and CT soft tissue window axial view (b) showing a button aneurysm in the form of focal aneurysmal dilatation of the left main coronary artery at its origin, and its branches LAD and LCX arteries (arrows).
View Figure 1
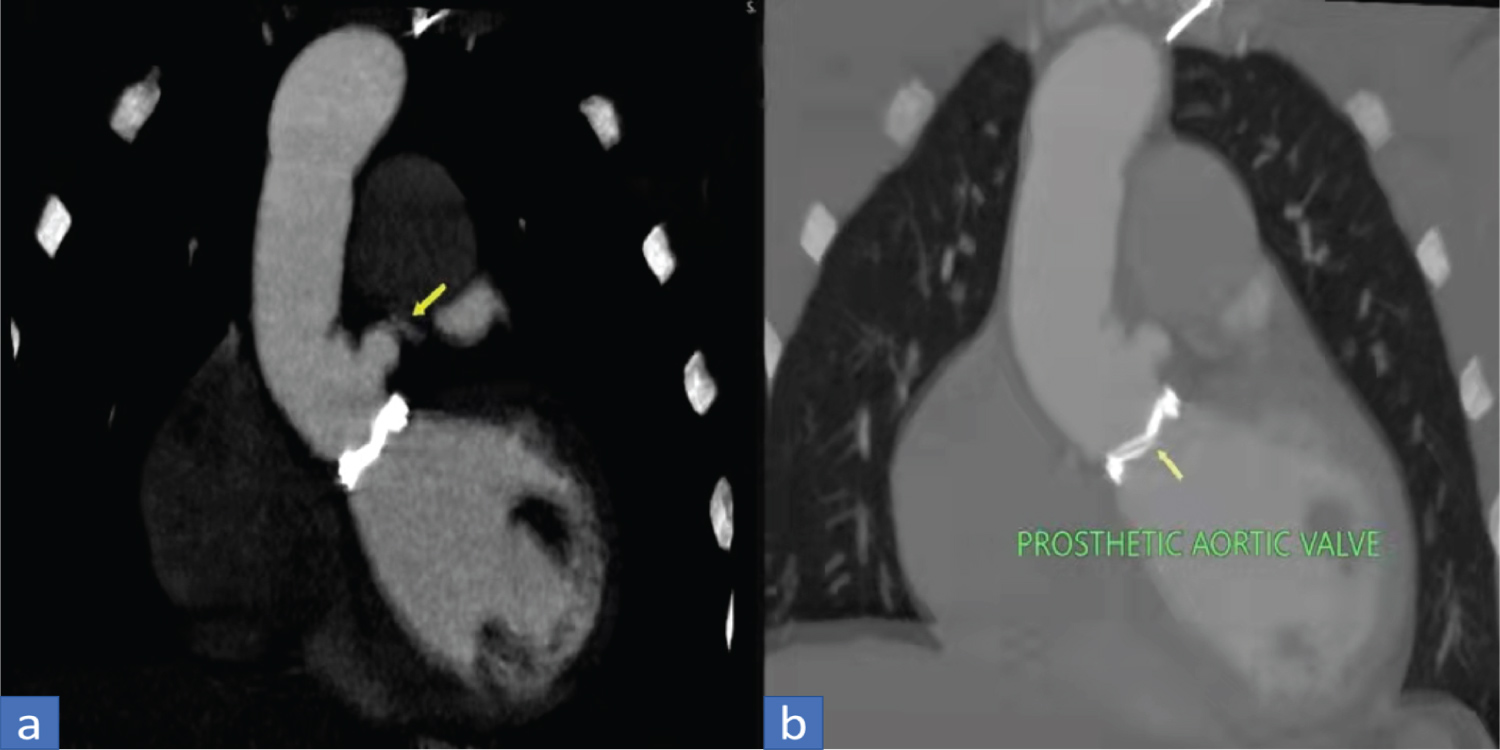 Figure 2: CT angiography image soft tissue window coronal view (a) showing a button aneurysm (arrow), lung window coronal view (b) showing an intact prosthetic aortic valve in situ (arrow).
View Figure 2
Figure 2: CT angiography image soft tissue window coronal view (a) showing a button aneurysm (arrow), lung window coronal view (b) showing an intact prosthetic aortic valve in situ (arrow).
View Figure 2
Coronary button aneurysm is one of the several complications post-Bentall's procedure that is performed in the pathologies such as large aneurysms and type A dissections, associated with aortic stenosis or insufficiency [4]. The procedure basically includes the replacement of the diseased aortic root and valve whereby anastomosis of the coronary arteries is done. Hence, complications such as coronary ostial aneurysms may be evident in some patients undergoing Bentall's procedure. The coronary ostial aneurysms may present in the form of either pseudoaneurysm, aneurysm at the anastomosis site to the composite graft, and aneurysm of the left main trunk [5]. Some common complications following Bentall's procedure are listed in Table 1.
Table 1: Common complications post Bentall's procedure. View Table 1
Coronary ostial aneurysm: It is an exceptionally rare complication to occur post-Bentall's procedure, however, if it does, may even have catastrophic consequences depending on the size of the aneurysm. Thus, a surgical repair may be required in order to avoid an aneurysmal rupture [5].
True aneurysm: The term "true aneurysm" refers to the aortic root aneurysm that generally necessitates a second surgical intervention which frequently occurs in people with connective tissue disorders such as in Marfan syndrome [6,7].
Pseudoaneurysm: Aortic root pseudoaneurysm is a rare complication and the most frequent sites to occur one is the graft anastomosis site, second being the coronary artery anastomosis site, followed by the aortotomy site, the aortic cannulation site, and the needle vent site [6,8].
Endoleak: Endoleaks are frequently experienced by patients undergoing endovascular repairs including both open surgical aortic root repair and endovascular repair of aortic arch aneurysms [6,9].
Dissection: The prevalence of dissection after aortic root repair is somewhat similar to that of an aortic root aneurysm which warrants a second surgical procedure. Thus, aortic root graft requires regular monitoring [6,7].
Perigraft seroma/Perivalvular leakage: Perigraft seroma in form of fluid between the open aortic graft and the sac wall may be a common finding right after surgery but should resolve over time. Although it may be aspirated, the routine drainage and evacuation of seroma fluid could nevertheless lead to its recurrence [6].
Pulmonary embolism: Pulmonary embolism should always be considered in patients with a history of aortic root repair presenting with vague complaints of chest pain and dyspnea that may mimic pseudoaneurysm or dissection [6].
Hemothorax: Aortic root repair carries the risk of hemothorax post-operatively that may necessitate thoracotomy and surgical drainage. Locating the source of the bleeding and ruling out an aortic root pseudoaneurysm may be possible with contrast-enhanced CT (CECT) [6].
Sternal dehiscence: Sternal dehiscence and sternal wound infections are significant consequences that can develop separately or simultaneously with mediastinitis. Displacement of sternal wires, sternal erosion, or cleft within the sternotomy site is the usually evident findings on CT [6,10].
Mediastinitis: Mediastinitis has the highest death rate of all the sequelae, ranging between 27-50%. Along with the clinical signs of fever, chest discomfort, and sepsis, the CT findings of abnormally high volumes of low-attenuation material surrounding the aortic graft or increased fluid and soft-tissue infiltration and the presence of gas suggest mediastinitis [6,11].
Among all the complications, our present case presents the coronary ostial aneurysm occurring in the left main coronary artery itself. The aneurysm, however, was modest and had low-risk implications. Therefore, the patient was managed conservatively with an uneventful hospital stay.
In conclusion, despite being an uncommon post-Bentall complication, a Button aneurysm of the coronary artery can indeed be identified sooner using a radiological modality like CT angiography. Hence, a regular follow-up is encouraged for the timely identification of all the complications associated with Bentall's procedure, so that the possibility of an inaccurate diagnosis leading to needless investigations and interventions may be avoided.
We wish to thank all involved in this study for their contribution.
Nirmal Prasad Neupane: Analyzed and interpreted the patient data; Kritisha Rajlawot: Major contributor in writing the manuscript; Sujan Thapa and Asim Sitaula: Literature review and report preparation.
All authors have read and approved the manuscript.
No funding was obtained for this study.
All data generated or analyzed during this study are included in this published article.
This case report did not require review by the Ethical committee for publication.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
All of the authors declare that they have no competing interests.