The retro-psoas iliac artery is a rare vascular anomaly that has been reported few times in the literature; and while it may be clinically silent with no specific symptoms; reporting it can prevent many complications that may arise during surgical and interventional procedures. We report a case of a 40-year-old male who presented with progressive neurological symptoms, and was found to have a right retro-psoas iliac artery as an incidental finding on a lumbar spine MRI.
Retro-psoas, Iliac artery, MRI, Vascular anomaly
Iliac artery anomalies are rather rare, the most common iliac artery anomaly is persistent sciatic artery with iliofemoral aplasia, which presents as a pulsatile mass in the gluteal region with absence of the femoral artery pulse [1,2]. The retro-psoas iliac artery is an extremely rare anatomical variant, with only eight reported cases in the literature in total [2-9]. Most of the patients are asymptomatic and the anomalous artery is detected incidentally during imaging. Serious vascular compromise may occur during orthopedic, vascular, or pelvic procedures if left unrecognized during imaging. We report a right retro-psoas iliac artery diagnosed incidentally on lumbar spine MRI in a 40-year-old male with progressive neurological symptoms.
A 40-year-old male patient presented to the emergency department at our institution with progressive upper and lower limb weakness and numbness for a duration of seven weeks, which evolved into oculobulbar symptoms, urinary incontinence and saddle anaesthesia. He was admitted to the neurology department for further assessment.
An enhanced whole spine MRI demonstrated enhancement and thickening of the nerve roots of the cauda equina; a radiological feature suggestive of Guillain-Barre syndrome (GBS). Incidentally, the right common iliac artery was seen arising from the abdominal aorta at the level of L4 and taking an anomalous course posterior and medial to the right psoas muscle, coursing between the psoas muscle and the vertebral bodies down to the level of the of S1 anterior to the right sacro-iliac joint where it gave rise to the right internal iliac artery. The left common iliac artery maintained a normal course (Figure 1).
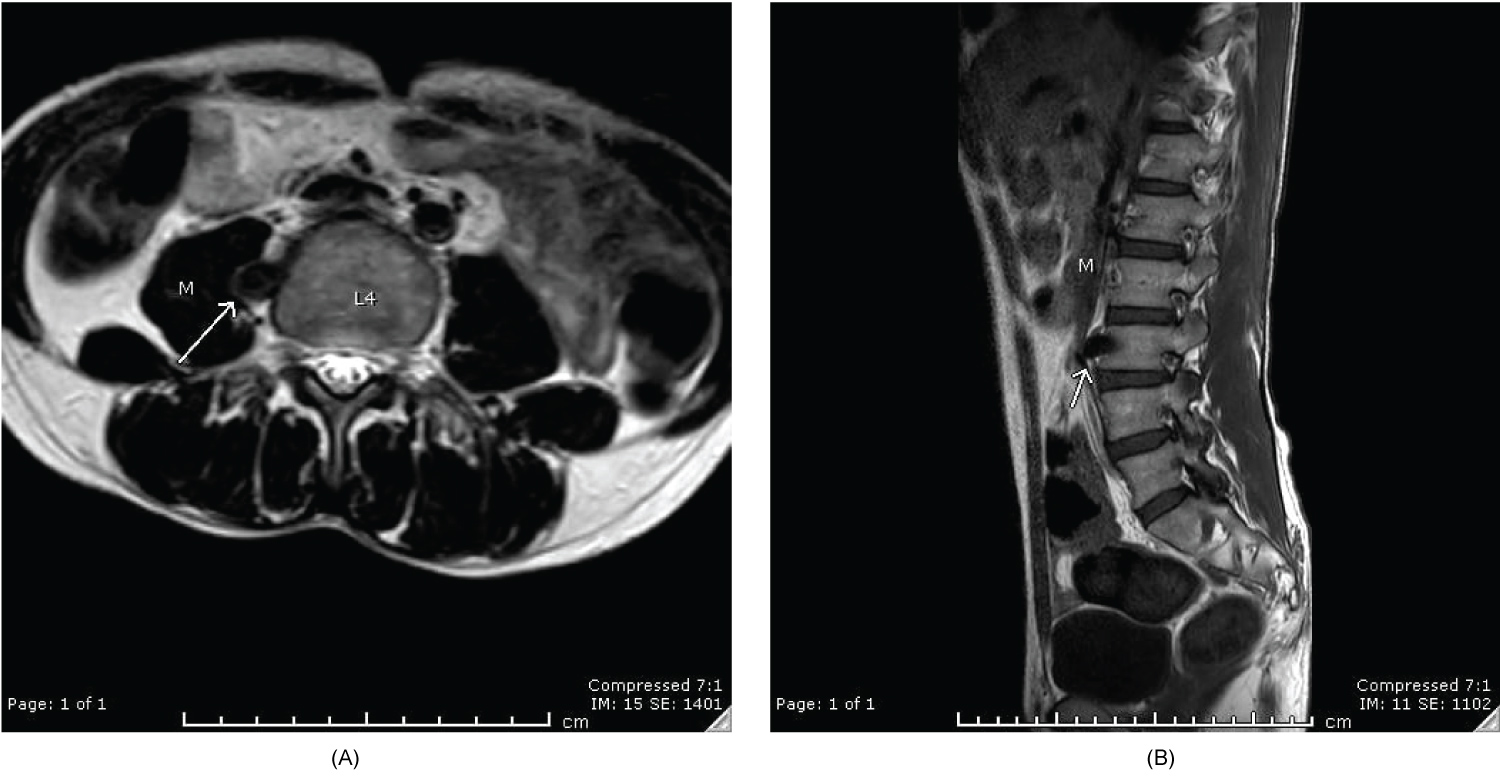 Figure 1: (a) Axial T2; (b) Sagittal T1 MRI images of the lumbar spine show the right common iliac artery (arrow) arising from the abdominal aorta at the level of L4 and taking an anomalous course posterior to the right psoas muscle (M).
View Figure 1
Figure 1: (a) Axial T2; (b) Sagittal T1 MRI images of the lumbar spine show the right common iliac artery (arrow) arising from the abdominal aorta at the level of L4 and taking an anomalous course posterior to the right psoas muscle (M).
View Figure 1
Cerebrospinal fluid analysis results showed elevated protein levels, and nerve conduction study demonstrated changes suggestive of chronic inflammatory demyelinating polyneuropathy/chronic GBS.
The abdominal aorta bifurcates at the level of L4 into the common iliac arteries, which runs medial to the psoas muscles before bifurcating into the internal and external iliac arteries at the pelvic brim. The external iliac artery crosses under the inguinal ligament to continue as the common femoral artery to supply the lower limbs. The internal iliac artery gives multiple branches at the upper sacral region to supply the pelvic viscera and muscles [2].
Embryologically the fifth pair of lumbar intersegmental arteries remain as the common iliac arteries while most of the intersegmental lumbar arteries become lumbar arteries [2]. The embryological basis for the retro-psoas artery variation is not yet fully understood, partially due to the scarcity of published cases in that regard. However, Sonneveld, et al. mentioned that this variant could be attributed to the umbilical artery connecting to the fourth, rather than the fifth pair of lumbar intersegmental arteries [7]. The first case of retro-psoas iliac artery was recognized in 1991 by Vohra, et al. [8]. Tamisier, et al. classified congenital anomalies of the iliac artery into three groups. Group I: Anomalies in the origin or course. Group II: Iliac artery hypoplasia or atresia with persistent sciatic artery. Group III: Isolated hypoplasia or atresia [10].
The anomalous iliac artery was right sided in all but one of the reported cases, in which it was left sided, as reported by Mizuki Ozawa, et al. [6]. Clinically, five of the cases were asymptomatic, while the remaining three presented with lower extremity claudication and pain [2,3,8]. In our patient, the anomalous iliac artery was on the right side, the patient’s symptoms were attributed to the clinical and radiological diagnosis of Guillain- Barre syndrome, rather than the presence of the anomalous artery.
Discovering and reporting anatomical variants -especially vascular variants- is of utmost importance. It is a necessary measure that should be taken to ensure the safety of patients who undergo any kind of intervention in the area of interest, whether it is vascular, neurosurgical or orthopaedic intervention. Hemorrhagic complications could be avoided by communicating these findings clearly to the surgical teams.
The retro-psoas iliac artery is an extremely rare vascular variant. Although it is mostly clinically asymptomatic; conveying the existence of this variant to the surgical teams is crucial and can be detrimental to the patient’s safety.
No source of funding to disclose.