Propofol is used as an induction agent to facilitate laryngeal mask airway (LMA) insertion but unwanted responses such as drop in blood pressure, cough, laryngospasm, movement and apnoea may occur. Use of adjuvant with propofol or a combination of different synergistic pharmacologic agents that can maintain airway patency and hemodynamic parameters can be exploited to avoidance these undesirable responses and effects during LMA insertion. We compared the effects of ketamine-fentanyl and propofol-fentanyl combinations on LMA insertion conditions and post-operative outcome in children undergoing herniotomy.
The study was randomized double-blinded conducted on eighty ASA physical statuses I and II paediatric patients age ranged 1 to 15 years scheduled for herniotomy. The patients were grouped into two (A and B) of forty patients each and LMA was inserted following administrations of two different drug combinations. Group A received pre-mixed ketamine 2 mg/kg and fentanyl 2 μg/kg while group B received pre-mixed propofol 2.5 mg/kg and fentanyl 2 μg/kg. The quality of response to LMA placement (LMA insertion conditions) and post-operative outcome (patient recovery) was assessed.
The number of patients with acceptable LMA insertion conditions were comparable in both groups, p = 1.000, while incidence of apnoea was significantly greater in propofol-fentanyl group, p = 0.045 with no difference in the post-anaesthesia discharge scores between the groups, p = 0.241.
Intravenous ketamine-fentanyl combination is a better induction agent for LMA insertion in children with acceptable LMA insertion conditions, good post-operative recovery scores and lower incidence of peri-insertion apnoea when compared with propofol-fentanyl combination.
Ketamine, Fentanyl, Propofol, Laryngeal mask airway, Laryngeal mask airway insertion conditions, Apnoea
Laryngeal mask airway (LMA) is a non-invasive supraglottic airway device that revolutionized the management of modern general anaesthesia [1,2]. It is now being increasingly used in place of face mask or endotracheal tube (ETT) during administration of anaesthesia either to facilitate ventilation or to pass ETT in a patient with a difficult airway [3,4].
Obtundation of airway reflexes is essential for LMA insertion and hence requires either intravenous or inhalational induction agent that suppresses the airway reflexes. Its insertion requires sufficient depth of anaesthesia for jaw muscles to relax and for the inserted LMA to be tolerated without undue coughing, gagging, breath holding and movement by patients [5,6]. Till date, different combinations of induction agents and adjuncts have been used for LMA insertion; yet, the ideal combination that provides the best insertion conditions with minimal side effects has not been identified, particularly in children.
Propofol has quick recovery profile after intravenous administration; and has been successfully used as a sole induction agent to facilitate LMA insertion in adults and children due to its predominant upper airway reflexes depressant action, unwanted responses such as drop in blood pressure, coughing, laryngospasm, and movement may occur [7,8]. Reduced sympathetic tone after propofol overdose or lighter plane of anaesthesia with inadequate induction dose has been implicated as the cause of the unwanted response [9,10]. Search for an induction agent(s) or adjunct that produce excellent LMA insertion conditions and good post-operative outcome is worthy of clinical endeavour.
Ketamine produces dissociative anaesthetic state by blocking the connection between the thalamic and limbic regions of the brain from processing external stimuli [11] but causes emergence phenomenon, elevated blood pressure, increased heart rate and raised intracranial pressure can occur [12]. Fentanyl is a potent synthetic opioid with faster onset of action and 50 to 100 times more potent than morphine. When used as pre-treatment agent for LMA insertion, it reduces induction dose of anaesthetic required for LMA insertion and prevent depression of airway reflexes caused by higher propofol doses. Studies [13,14] have also shown that propofol-fentanyl combination provides a better LMA insertion conditions. Evidences abound on the possible synergistic interactions between ketamine and opioids [15-17]. Combinations of opioids (such as fentanyl) and NMDA receptor antagonists (such as ketamine) may result in an enhanced effect which permit combination of low doses of both drugs.
There is paucity of randomized controlled trials on the use of induction agent(s) for LMA insertion despite its routine use for paediatric day-case surgeries in our environment. We compared the LMA insertion conditions and post-operative recovery scores following day-case herniotomy in African children when ketamine-fentanyl or propofol-fentanyl combination was used as induction agents prior to LMA insertions.
After approval from institutional ethical review committee (ERC PAN/2017/05/1679) of a large tertiary hospital in West Africa and written informed consent from the parents, 80 paediatric patients of ASA grade I and II, aged 1-15 years, scheduled for elective herniotomy under general anaesthesia with spontaneous breathing using an LMA was recruited. Sample size was calculated by using comparison of proportions (equal size group) [18]. A previous study 14 revealed 36% of the patients experienced excellent LMA insertion conditions, and clinical significance is said to occur if 25% experience good LMA insertion conditions.
Children with history of allergic reactions to propofol, ketamine and fentanyl, clinically significant cardiovascular, respiratory, hepatic and renal diseases, oropharyngeal pathology, hiatus hernia, respiratory tract infection/hyperactive airway, seizure disorder, raised intracranial or intraocular pressure, anatomical abnormality of the airway, risk of aspiration and those currently taking sedative or analgesic drugs were excluded from the study.
Patients were fasted according to the fasting guidelines for surgery (6 hours for solid meals, 4 hours for breast milk and 2 hours for clear carbohydrate drinks). Patients were allocated to either of the group A (pre-mixed ketamine 2 mg/kg and fentanyl 2 μg/kg) or B (pre-mixed propofol 2.5 mg/kg and fentanyl 2 μg/kg); both patients and the investigators were blinded to the randomization schedule and the study drugs. Each patient or parent randomly picked from the ballot box containing the two groups of ballot papers.
Venous access was secured with appropriate-sized cannula on the ward with the aid of EMLA cream an hour before being transferred to the operating suite. On arrival at the operating suite, multi-parameter patient monitor was attached to patients and baseline physiologic parameters such as heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), respiratory rate (RR), temperature, and peripheral oxygen saturation (SpO2) were measured and recorded and baseline ECG noted. All patients received intravenous (IV) atropine 0.01 μg/kg and IV paracetamol 12.5 mg/kg prior to induction of anaesthesia. The patients were pre-oxygenated for 5 minutes and, based on the group of the patients, the study drugs were given intravenously over 10 seconds. Blinding was achieved by wrapping of the syringes containing the study drugs with aluminium foil to conceal their contents. To ensure accurate delivery of the study drugs, the syringes were unwrapped under drapes before administered to patients. After 120 seconds post-administration of study drugs, appropriate-sized classic paediatric LMA was inserted using the standard midline approach and the cuff was then inflated with air until effective ventilation was established. Following successful insertion, correct LMA position was assessed by observing chest movement, square wave capnographic tracing and reservoir bag movement with both spontaneous and assisted ventilation.
Incorrectly placement, LMA was removed and re-inserted after the second dose of the assigned drugs. When a second dose was given, the procedure was repeated as previously detailed. To prevent dislodgement, LMA was properly secured with adhesive tapings. When LMA insertion was unsuccessful after 3 attempts, patient's trachea was intubated with endotracheal tube following administration of suxamethonium 1 mg/kg intravenously, and the patient was excluded from the study.
After successful insertion of LMA, patient was allowed to breathe spontaneously. In case of apnoea (absence of respiration for more than 30 seconds), manual assisted ventilation via LMA was done to keep the SpO2 above 95% till spontaneous breathing resumed. Thereafter, patient was positioned for caudal block in the left lateral position and 0.5 ml/kg of 0.25% plain bupivacaine was injected under aseptic condition into the epidural space via sacral hiatus for both intra-operative and post-operative analgesia.
Anaesthesia was maintained with 1% halothane in 50% oxygen with medical air. The intraoperative monitored parameters were peripheral oxygen saturation (SpO2), heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MAP) and respiratory rate (RR) at 1 minute, at 3 minutes, and subsequently at 5 minutes interval till the end of the surgery. Intra-operative fluid management was achieved with 4.3% dextrose in 0.18% saline and 0.9% saline in younger and older patients respectively.
At the end of surgery, all patients were extubated after suctioning the hypopharynx with the LMA cuff still inflated until fully awake. The patients were then transported in recovery position to the post-anaesthetic care unit (PACU) where monitoring of vital signs, fluid administration, and oxygen supplementation were continued. Post-anaesthetic discharge score 19 was at 30 minutes, 45 minutes and 1 hour post-extubation.
Data were analyzed with SPSS Version 20.0 (SPSS Ltd, Chicago, IL, USA). Values were presented as means (SD) or frequencies, medians and proportions and level of significance analyzed with Student's t-test. Categorical data such as gender and number of attempts were analyzed with the Chi Square test or Fisher's exact test as appropriate. Post-anaesthesia discharge score was analyzed with Mann Whitney U test. A p value < 0.05 was considered to be statistically significant.
A total of 80 children, aged 1-15 years were recruited and randomized into two groups of 40 patients each. Patients in group A received ketamine-fentanyl combination and propofol-fentanyl combination was administered to patients in group B. All patients in both groups, except one in group B that regurgitated after LMA insertion, completed the study. LMA insertion was successful at first attempt in all the patients in both groups. The demographic characteristics and anthropometric parameters were not different in both groups, Table 1.
Table 1: Demographic and anthropometric parameters of the patients. View Table 1
The respiratory rate at baseline, 1, 3 and 5 minutes after LMA insertion were similar in both groups with no significant difference, p = 0.089, p = 0.190, p = 0.187 and p = 0.14 respectively. However, the respiratory rate was significantly higher in group A than group B patients at 10, 15, 20, 25, 30 and 35 minutes after induction of anaesthesia, p < 0.05. There was no significant difference at 40 minutes after LMA insertion till the surgery was concluded (p > 0.05), Table 2.
Table 2: Respiratory rate (RR) of the patients in both groups. View Table 2
The incidence of apnoea after LMA insertion was significantly higher in the propofol-fentanyl group compared with the ketamine-fentanyl group, 33 (84.6%) patients versus 26 (65%) patients, p = 0.045. However, the mean duration of apnoea was similar in both groups, 62.31 ± 23.88s versus 68.18 ± 32.06s respectively for groups A and B, p = 0.439. Apnoea was observed only after the administration of the study drugs for induction of anaesthesia and before LMA insertion. Moreover, prolonged apnoea (> 120 seconds) was not observed in both groups throughout the surgery, Table 3.
Table 3: Incidence of apnoea in both study groups. View Table 3
Statistically significant proportion of patients in group B achieved full mouth opening during LMA insertion, 34 (87.20% versus 14 (35%) patients, p = 0.006; but proportion of patients with partial mouth opening was higher in group A than B, 26 (65%) versus 5 (12.80%) patients, p < 0.001, Table 4. LMA insertion conditions were scored and categorized as excellent (score of 18), satisfactory (scores of 16-17) and poor (score < 16), Table 5.
Table 4: Comparison of laryngeal mask airway (LMA) insertion parameters. View Table 4
Table 5: Categorization of LMA insertion conditions of the patients. View Table 5
None of the patients in the two groups coughed after the LMA insertion. Swallowing was absent in 34 (85.0%) patients in group A compared with 38 (97.4%) patients in group B, p = 0.724; proportion of patients with slight swallowing was comparable between the two groups, with 6 (15%) patients (group A) versus 1 (2.6%) patient (group B), p = 0.131 (Table 4).
Patient movement was absent in 28 (70%) patients versus 34 (87.2%) patients in groups A and B (p = 0.525); moderate patient movement was not also significantly different in groups A and B, 12 (30%) patients versus 5 (12.8%) patients (p = 0.146); but vigorous patient movement was not observed throughout the study period (none of the 40 patients in group A and 39 patients in group B experienced vigorous movement) p = 1.000. Proportions of patients with easy, difficult, and impossible LMA insertions were comparable in groups A and B: 36 (90%) patients versus 38 (97.4%), p = 0.908; 4 (10%) patients and 1 (2.6%) patient. P = 0.37; and 0 (0%) versus 0 (0%) patients respectively (Table 5).
While patients were in the post-anaesthetic care unit and 30 minutes after removal of the LMA, all the 40 (100%) patients in group A and 37 (94.9%) patients in group B met the discharge criteria (modified post-anaesthesia discharge scoring system), p = 0241. At 45 and 60 minutes post LMA removal, all the patients in both groups scored at least 9 on the modified post-anaesthesia discharge scoring system and were discharged, Table 6.
Table 6: Post-anaesthesia discharge scores in the study groups. View Table 6
This study showed that ketamine-fentanyl and propofol-fentanyl combinations provide acceptable LMA insertion conditions, good post-operative recovery score and lesser incidence of peri-insertion apnoea in children. The use of combination of drugs for induction of anaesthesia was heavily criticized in the past but the concept of co-induction has been accepted as a common practice due to its faster onset of action, fewer side effects, and cost-effectiveness.
Our findings are in agreement with results of other studies [19-22] that showed no different in the LMA insertion conditions between propofol-fentanyl and propofol-ketamine. The similarity between the present study and the findings of the other researchers could be due to combinations and use of the same induction agents on similar subjects. Unlike in our study, Singh, et al. [23] reported a better LMA insertion conditions in the propofol-fentanyl-treated patients in comparison with propofol-ketamine treated group. The difference that was observed by Singh, et al. [23] might be explained by the combination of low-dose ketamine (0.5 mg/kg) with propofol in their propofol-ketamine group.
Similar to our finding higher proportion of patients in the propofol-fentanyl group than in the ketamine-fentanyl group achieved full mouth opening prior to LMA insertion, Guptal, et al. [20] reported better level of jaw relaxation when propofol-fentanyl was used for LMA insertion than propofol-ketamine. The full mouth opening achieved by higher number of patients in the propofol-fentanyl group compared with the ketamine-fentanyl group could be ascribed to the ability of ketamine to increase the skeletal muscle tone. Whereas propofol has some degree of muscle relaxant effect on skeletal muscle, thereby providing better jaw muscle relaxation and mouth opening than ketamine.
In contrast to the result of this study, Singh, et al. [23] revealed that equal number of patients from the propofol-fentanyl and propofol-ketamine groups experienced full jaw relaxation. This finding might be due to the low-dose ketamine that was added to propofol; which was pharmacologically insufficient to increase the jaw muscle tone. Similarly, Yousef and Elsayed, [24] also reported that 45 patients in the propofol-ketamine group and 38 patients in the propofol-only group achieved full mouth opening during LMA insertion. The fact that the LMA insertions in all the patients enrolled into their study were guided by bispectral index (BIS) and attempted at BIS value of 40 could explain absence of insignificant difference in the insertion conditions between the two groups. At this level, some degree of muscle relaxation may be observed in the patients and might have increased the degree of mouth opening in propofol-ketamine group.
Our study reported no incidence of cough following LMA insertion in our patients; and this agrees with the finding of Ghatak, et al. [21]. They reported that 7 out of 60 patients vs. 3 out of 60 patients respectively in the propofol-ketamine and propofol-fentanyl groups coughed after LMA insertion, respectively. Gupta, et al. [20] however, reported incidence of mild cough which was similar and statistically insignificant between the patients in the propofol-ketamine and propofol-fentanyl groups, 11 (36.66%) patients vs. 13 (43.33%) patients respectively. The only plausible explanation for the absence of coughing among patients in the present study could be the predominant anti-tussive effect of fentanyl over the obtundation of airway reflexes by propofol.
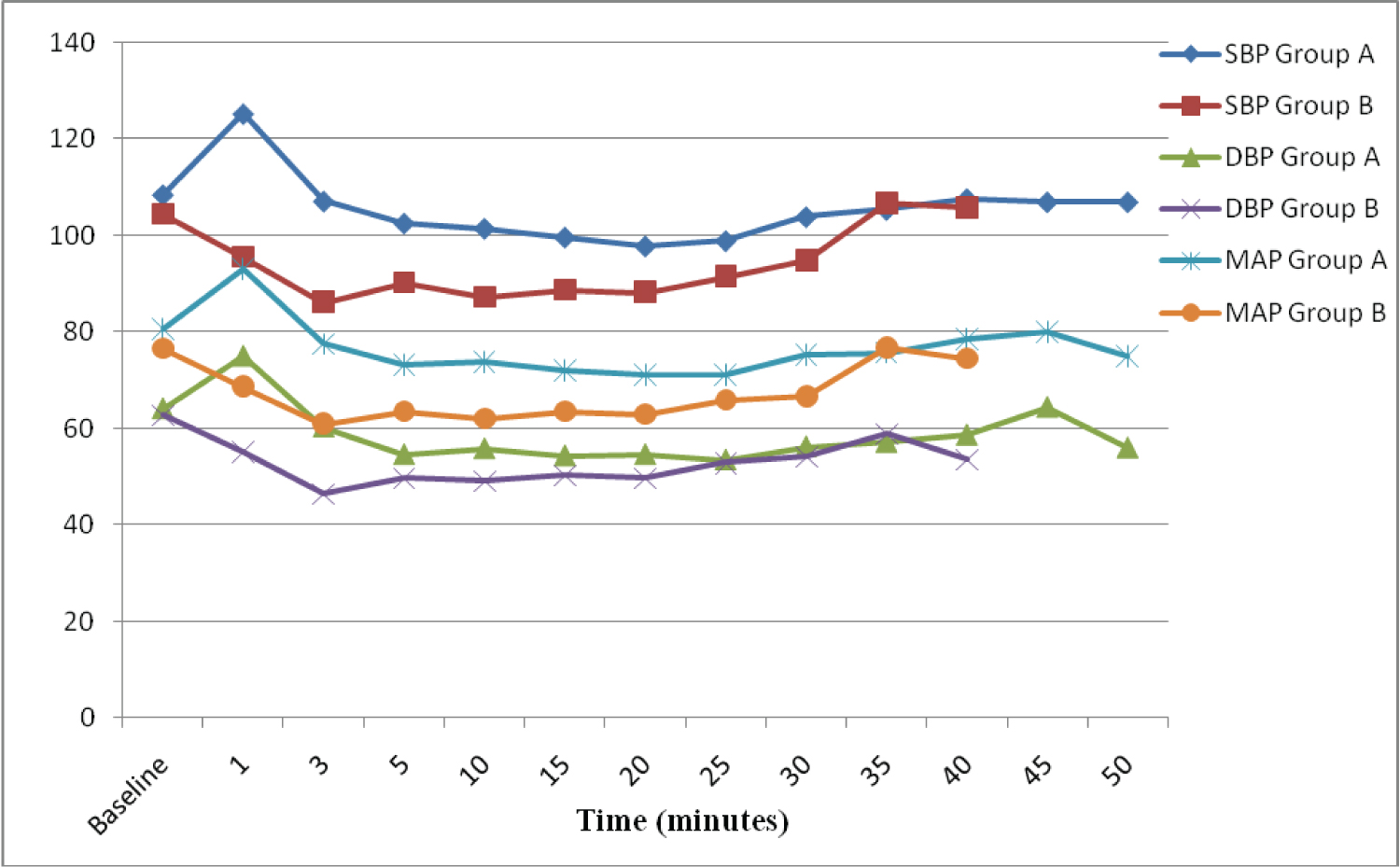 Figure 1: Trend of mean systolic blood pressure, diastolic blood pressure and mean arterial pressure of the patients over 50 minutes post LMA insertion.
View Figure 1
Figure 1: Trend of mean systolic blood pressure, diastolic blood pressure and mean arterial pressure of the patients over 50 minutes post LMA insertion.
View Figure 1
At variance with our result study, Singh, et al. 23 reported higher incidence of coughing after LMA insertion in the propofol-ketamine than in the propofol-fentanyl groups; 14 out of 50 patients versus 4 out of 50 patients. This might be due to the anti-tussive effect of fentanyl or earlier LMA insertion before the peak effect of the administered fentanyl was attained.
We also reported higher incidence of slight swallowing in the ketamine-fentanyl group compared with the propofol-fentanyl group, and this is corroborated by the findings of Ghatak, et al. [21] in their patients groups (propofol-ketamine and propofol-fentanyl) as well, though differences observed in the two studies were insignificant. In their study, slight swallowing was observed in 6 out of the 60 patients in the propofol-ketamine group and 4 out of the 60 patients in the propofol-fentanyl group. Similarly, our result agrees with the outcome published by Hussein [22] who studied LMA insertion in patients randomized into propofol-fentanyl and propofol-ketamine groups. The insignificantly higher incidence of slight swallowing seen in the ketamine-fentanyl group was probably due to the fact that both pharyngeal and laryngeal reflexes are usually preserved after administration of ketamine. The similarity in the results of the two studies might be due to the blunting of the swallowing reflex by fentanyl that was combined with ketamine.
The degree of swallowing observed after LMA insertions by Singh, et al. [23] between their study groups was significant and differs from our finding. Singh and colleagues [23] reported observed slight swallowing in 6 out of the 50 patients in the propofol-fentanyl group compared with 15 out of the 50 patients in propofol-ketamine group. The increase might be ascribed either to the use of ketamine, failure to administer fentanyl in the two groups or early insertion of LMA before the onset of action of the drugs.
As observed in our study, Gupta, et al. [20], Ghatak, et al. [21] and Hussein [22] reported moderate patient movement was observed in many patients in the ketamine-fentanyl group than in the propofol-fentanyl group but vigorous patient movement after LMA insertions was not observed by the authors in the four studies. The lack of significance in the extent of movement in our study and others might be due to the synergistic effect of fentanyl on the depth of anaesthesia when combined with ketamine and propofol with reduced movement of patients in both groups.
In contrast to our finding, Singh, et al. [23] observed a significant movement among patients during LMA insertions in the propofol-fentanyl group compared with propofol-ketamine group. Vigorous body movement was noticed in 1 out of the 50 patients in the propofol-fentanyl group and 11 out of the 50 patients in propofol-ketamine group. This observed vigorous movement in the propofol-ketamine group might be LMA insertions before onset of action of the induction agents was attained.
As observed in our study, Singh, et al. [23], Goyal, et al. [25] and Hussein [22] reported no case of laryngospasm after LMA insertion. Absence of laryngospasm reported in our patients and other authors cited above might be as a result of the airway-depressant effect of fentanyl and its synergistic effects on ketamine and propofol. Though some authors [20,21] reported high proportion of patents with laryngospasm after LMA insertion in the propofol-ketamine than in propofol-fentanyl groups, the difference was insignificant.
In our study, the scores for ease of LMA insertion were similar in ketamine-fentanyl and propofol-fentanyl groups. This observation agrees with the findings of Ghatak, et al. [21] and Singh, et al. [23] who reported difficult insertions in 4 out of 60 patients vs. 3 out of 60 patients and 3 out of 50 patients vs. 4 out of 50 patients respectively in the propofol-ketamine and propofol-fentanyl combinations.
We also observed no difference in post-anaesthesia discharge scores between the two groups. This is consistent with the results of Yousef and Elsayed, 24 who reported similar mean recovery time after LMA removal in patients treated with propofol-placebo and propofol-ketamine combinations, 11.5 ± 9.4 min vs. 14.7 ± 11.3 min, p = 0.32. However, Goyal, et al. [25] reported prolonged mean recovery time in the propofol-ketamine than propofol-fentanyl groups, 14.20 ± 3.35 min vs. 11.60 ± 3.45 min, p < 0.05. This finding might be due to printing error as lack of difference was indicated in the text but p < 0.05 was probably reflected in one of their Tables.
As observed in our study, Singh, et al. [23] and Hussein [22] reported increased mean respiratory rate in the ketamine-fentanyl group after LMA insertions. The increased respiratory rate in these two studies was limited to the first 5 minutes, which constituted their study period, after LMA insertion. This is in contrast to ours, where increased respiratory rate in ketamine-fentanyl group was recorded throughout the study period, 50 minutes post LMA insertion; but significant increase was noted between 10-35 minutes. The reason for the reduced respiratory rate in the propofol-fentanyl group might due to the ability of propofol to cause respiratory depression and/or apnoea even at induction doses. On the other hand, ketamine causes little or no respiratory depression at induction doses.
Higher incidence of apnoea in the propofol-fentanyl group than ketamine-fentanyl group reported in our study was comparable with the findings by Hussein, [22] and Gupta, et al. [20] 15 patients vs. 6 patients and 60% vs. 27% respectively in the propofol-fentanyl group and propofol-ketamine groups. Singh, et al. [23] also reported prolonged apnoea in 40 (80%) out of 50 patients in the propofol-fentanyl group and 25 (50%) 50 patients in the propofol-ketamine group.
The incidence of apnoea in the propofol-fentanyl groups was expected to be higher than in the propofol-ketamine group because either fentanyl or propofol is a potent cause of apnoea when used during anaesthesia without the appropriate precaution. Moreover, these drugs potentiate each other when combined, which may exaggerate the apnoeic effect.
From this study, it can be concluded that a combination of intravenous ketamine 2 mg/kg and fentanyl 2 μg/kg, is a better induction agent for insertion of laryngeal mask airway. It provides acceptable LMA insertion condition score and a good post-operative recovery score that were comparable with intravenous propofol 2.5 mg/kg and fentanyl 2 μg/kg combination. Though, both LMA insertion condition and post-recovery scores were comparable in the two groups, but low incidence of apnoea achieved by ketamine-fentanyl combination makes it a better and safer combination than propofol-fentanyl combination.
We acknowledge the support from the anaesthetists, paediatric team, peri-operative nurses and surgical ward nurses towards the management of the patients.
The study was commenced after obtaining certificate for ethical approval from ethical review committee, University of Ilorin Teaching Hospital (ERC PAN/2017/05/1679), located in Ilorin East Local Government area of Kwara State, Nigeria in West Africa.
This study was self-sponsored by the authors.
We declare no conflicts of interest.