Background: Hemodynamic instability of patients during induction of anesthesia and intubation, are very important clinical concern. Hemodynamic change after induction of general anesthesia is a common event and associated with negative result in clinical practice.
Methodology: An institutional based observational prospective cohort study was conducted from February 26 up to April 30. The source of population, all adult patients age between 18- 60 years old, underwent abdominal surgery under general anesthesia in Wolaita Sodo Teaching and Referral Hospital during the study period. We checked data manually for completeness and then coded and entered into the epi data version and export to SPSS statistical package program (Version 25) for further analysis. Normality of variables was measure using the Shapiro-Wilk test. Differences of numerical data between groups were evaluated using student's t-test and Mann-Whitney U-test. A p value of < 0.05 consider as statically significant.
Result: Mean arterial pressure was significantly increased immediately after induction of anesthesia, in the ketamine group compared with ketamine+ thiopental (P < 0.003). Heart rate was significantly rise in ketamine group during induction of anesthesia (maximum 96.42 ± 13.08) (P < 0.05). The maximum Systolic blood pressure change is observed after intubation in ketamine group 133.42 ± 12.04 while all Diastolic blood pressure was significantly different from baseline at post induction and intubation, 5 min and 10min in both group, (P value 0.001,0.005, 0.000, and 0.008 respectively) higher DBP (79.82 ± 10.36) was measured immediately after induction of anesthesia in ketamine group l measurement time drop in ketamine-thiopental group.
Conclusions: In conclusion, the use of a combination of the drug with ketamine has a better hemodynamic stability effect than using a single (ketamine or thiopental) induction agent.
Hemodynamic instability, Ketamine, Ketamine with thiopental
ASA: American Society of Anesthesiologists; BP: Blood Pressure; CAD: Coronary Artery Disease; CSA: Central Statistical Agency of Ethiopia; CBF: Cerebral Blood Flow; DBP: Diastolic Blood Pressure; ECG: Electrocardiogram; ETT: Endotracheal Intubation; GA: General Anesthesia; HR: Heart Rate; ICU: Intensive Care Unit; MAP: Mean Arterial Pressure; MC: Mallampati Class; NMD: N-methyl D-aspartate; SPO2: Oxygen Saturation; PONV: Post Operative Nausea and Vomiting; PRCT: Prospective Randomized Control Study; RCT: Randomized Control Study; SBP: Systolic Blood Pressure; SNNPRS: Southern Nations Nationalities and Peoples' Regional State; WSUTRH: Wolaita Sodo University Teaching and Referral Hospital.
Hemodynamic instability of patients during induction of general anesthesia is a very important clinical concern and it is a common event associated with negative results in clinical practice [1]. During induction of anesthesia patients are exposed to pain full procedure such as laryngoscopy and endotracheal intubation. This procedure is often associated with tachycardia, hypertension, arrhythmia and other undesirable hemodynamic changes [2]. Hypotension and hypertension all through general anesthesia are independently associated with adverse results in patients having both abdominal and non-abdominal surgery [3]. In particular, general anaesthesia is highly associated with morbidity and mortality [4,5]. This is often accompanied by a period of hemodynamic instability, especially hypotension, which could be a significant problem in patients with compromised cardiac output [6]. Hemodynamic disturbance is highly prevalent in abdominal surgery and associated with unfavorable patient outcome. An arterial blood pressure (ABP) decline below the lower limit of the vascular auto regulation curve might lead to ischemia of vital organs [7].
Major adverse cardiovascular events (MACE) constitute 15% of lawsuits against surgeons and anesthesiologists with 64% of those associated with death and 21% with brain damage [8].
About 9% of patients experienced clinically significant hypotension in the period 0-10 minutes after anesthetic induction in common clinical practice that leads to postoperative complications and end organ damage [3]. Another study shows the incidence of intraoperative hemodynamic change varies between 5% and 99% [9].
Perioperative hypertension affects 26.4% of the global population. It is an independent predictive factor of cardiac adverse events in abdominal and other non-cardiac surgery. Hypotension is frequent between the induction of anesthesia and the beginning of surgery. A decrease of 40% in MAP and an episode of a MAP < 50 mmHg during surgery are associated with cardiac events in high-risk patients. Even short episodes of intraoperative MAP of < 55 mmHg are associated with acute kidney injury and myocardial injury after abdominal and other non-cardiac surgery [10]. Maintaining hemodynamic stability during induction and maintenance of anaesthesia is an important task for the anesthesia providers [11].
Thus, a general anaesthetic agent with minimal effect on heart rate (HR), blood pressure (BP) cardiovascular instability, and better control of airway would be the agent of choice for general anaesthesia, commonly for gastrointestinal tract surgery [5].
There is no ideal induction agent that has yet been discovered in terms of providing a stable hemodynamic with fewer adverse effects since the introduction of general anaesthesia [12,13]. Many studies have been conducted to determine the effects of different types of medications such, as etomidate, thiopental, propofol, ketamine, and other narcotics for attenuating hemodynamic response to laryngoscopy and induction of anesthesia [1,2,8].
Ketamine is one of the most commonly used induction agents in anesthesia practice, particularly in developing countries like African countries. It is an N-methyl-D-aspartate (NMDA) receptor antagonist with strong analgesic effects, even at low concentrations [14]. It elevates arterial blood pressure, pulmonary artery pressure, and heart rate due to sympathetic stimulation. Ketamine is more lipid soluble and less protein bound than thiopental [15]. An important consideration in the use of ketamine anesthesia relates to the high incidence of hallucinations, nightmares, altered short-term memory, and cognition during the early recovery period. These effects are dose dependent; the reduction of induction dose with lower incidence, without pain and awareness. Prior administration of thiopental or benzodiazepines can blunt ketamine-induced cardiovascular and hemodynamic events [16].
Barbiturates have been used for over 30 years. Intravenous (IV) pentobarbital, rectal methohexital, and thiopental are the barbiturates that have been studied for procedural sedation and induction of anesthesia. Thiopental can produce effective sedation within one minute, and has a rapid clinical recovery (about 15 min). Thiopental administered intravenously has adequate sedation, faster recovery, and a lower rate of bradycardia and desaturation [17]. However, it has several disadvantages, including decreased arterial pressure, dose-dependent reduction in cardiac output, stroke volume and systemic vascular resistance which associated with a compensatory tachycardia [18]. In theory, the opposing hemodynamic effects of these two drugs (ketamine and thiopental), might be complementary and minimize overall adverse effects. In balanced anesthesia, a mixture of small amounts of several anesthetic drugs is concurrently administrated, which summates the advantages, but not the disadvantages, of the individual components of the mixture. Considering the concept of balanced anesthesia and also, little information available on the hemodynamic effects of a combination of ketamine-thiopental in patients undergoing surgery, with non-Comorbidity, this study will be conducted to compare the hemodynamic responses to ketamine versus ketamine-thiopental sodium combination for induction of anesthetic in patients undergoing abdominal surgery [5].
The homodynamic effects of combination of ketamine and thiopental is not study in Ethiopia so the aim of this study is to compere the hemodynamic effects of ketamine versus ketamine with thiopental combination for patient undergoing to abdominal surgery under general anesthesia.
An institutional based observational prospective cohort study was conducted from February 26 up to April 30. The source of population, all adult patients age between 18-60 years old, underwent abdominal surgery under general anesthesia in Wolaita Sodo Teaching and Referral Hospital during the study period.
Patients of ASA class I and II, age ranging from 18-60 years and who were undergoing abdominal surgery under GA were included in the study. Patient's difficult airway, pre-operative hypertension, and patients on beta-blocker were excluded from the study. Patients' selection and drug choice were based on duty anesthetist preference.
The primary endpoint of this study was to assess the effects of ketamine versus ketamine with thiopental on hemodynamic stability among patients undergoing abdominal surgery at Wolaita Sodo University. The sample size was calculated using two independent sample size formulas based on hemodynamic stability among the group. There is no previous study conducted in this area, and we do not adopt results from literature to calculate sample size because geographic and population differences affect our study. This is sample is calculated by using G* power software 3.1.9.4 version we calculated the proportion of two different independent mean by the following.
Tile-two tail, Effect size d = 0.8, α err probability = 0.025, Power (1- β err probability = 0.9, Allocation ratio N1/N2 = 1. This gives N1 = number of subjects to take ketamine 41, N2 = number of subjects to taken ketamine with thiopental 41, Added 10% contingency, Total sample size = 90. Participants are selected using convent sampling method. All patents full fill our inclusion criteria during the study period used as a sample. The questionnaire, which prepared in English, used to collect data. After providing training for data collectors, data collected by one MSc and two BSc Anesthetists. Appropriate data were collected using observations of patient hemodynamic parameters such as HR, SBP, DBP, and MAP, as usual app all standard monitoring device including noninvasive blood pressure (NIBP) cuff, pulse-oximetry, and electrocardiograph (ECG) record vital sign at pre induction (baseline), immediately after induction, immediately after intubation, fifth minute, tenth minute, fifteenth minute, and thirteenth minute. Whereas reviewing patients' chart where employed for demographic, anesthesia, medical and surgical related factors. Anesthesia provider opens intra venous (IV) line, and administers fluid as routinely. Pre-oxygenate the patient with 5 L/min 100% of Oxygen via face mask, for 5 minutes and give an injection of atropine 0.02 mg/kg I.V. prior to induction. The anesthetist provides an induction dose of ketamine 1.5 mg/kg for (Group K) and provides ketamine 0.5 mg/kg and thiopental 2.5 mg/kg, followed by ketamine for (Group KT).
➣ ASA-I patient no systemic disease come with surgical treatment only.
➣ ASA- ӀӀ mild systemic disease but get appropriate treatment.
➣ Baseline vital sign- vital patient's condition parameter is before induction of anesthesia.
➣ Hemodynamic instability- 20% changes on vital sign from baseline.
➣ Tachycardia-increase heart rate above 100 b/mint.
➣ Hypotension-decries blood pressure over 20% mm Hg from baseline.
We checked the data manually for completeness and then coded and entered into epi data version 3.1 computer programs for cleaning. Descriptive statistics are used to summarize data, tables and figures. The principal investigators perform entry and cleaning data. Ten percent of the questionnaires were crosschecked with the entered data to keep up its validity. The SPSS statistical package program (Version 25) is used to analyze all the data. Data expressed as means ± standard deviation. Normality of variables was measured using the Shapiro-Wilk test. Differences of numerical data between groups evaluated using the student's t-test and Mann-Whitney U-test. A p value of < 0.05 is considered as statically significant.
A total of 90 patients were included and none excluded from the study. In the, distribution age significant, different not observed in patients enrolled under study. The largest age distribution observed at ages between 18-28, was 38 (42.2%). The mean and standard deviation of age was 35.76 ± 13.289 (Table 1).
Table 1: Age distribution of patients in the two groups. View Table 1
Socio- demographic characteristic weight, sex, ASA, mouth opening, mallampati class, anesthetist experian's and drugs (premedication and additional dose) were no significant differences between the groups (Table 2).
Table 2: Socio-demographic characteristic of patients in two groups. View Table 2
Patients in both groups were comparable with respect to preoperative baseline hemodynamic variables. The mean arterial pressure difference between the groups is not significantly different before induction (P-value = 0.216; it is insignificant). Immediately after induction of anesthesia, a 96.42 ± 8.88 significant increase in mean arterial blood pressure was observed in the ketamine group from the baseline, while in the ketamine-thiopental group; there was a rise in mean arterial pressure at three consecutive measurements again after 15 mints and 30 mints in the ketamine group (P < 0.003).
The maximum mean arterial pressure was 96.42 ± 8.88 mmHg with a ketamine group seen immediately after induction anesthesia (Figure 1).
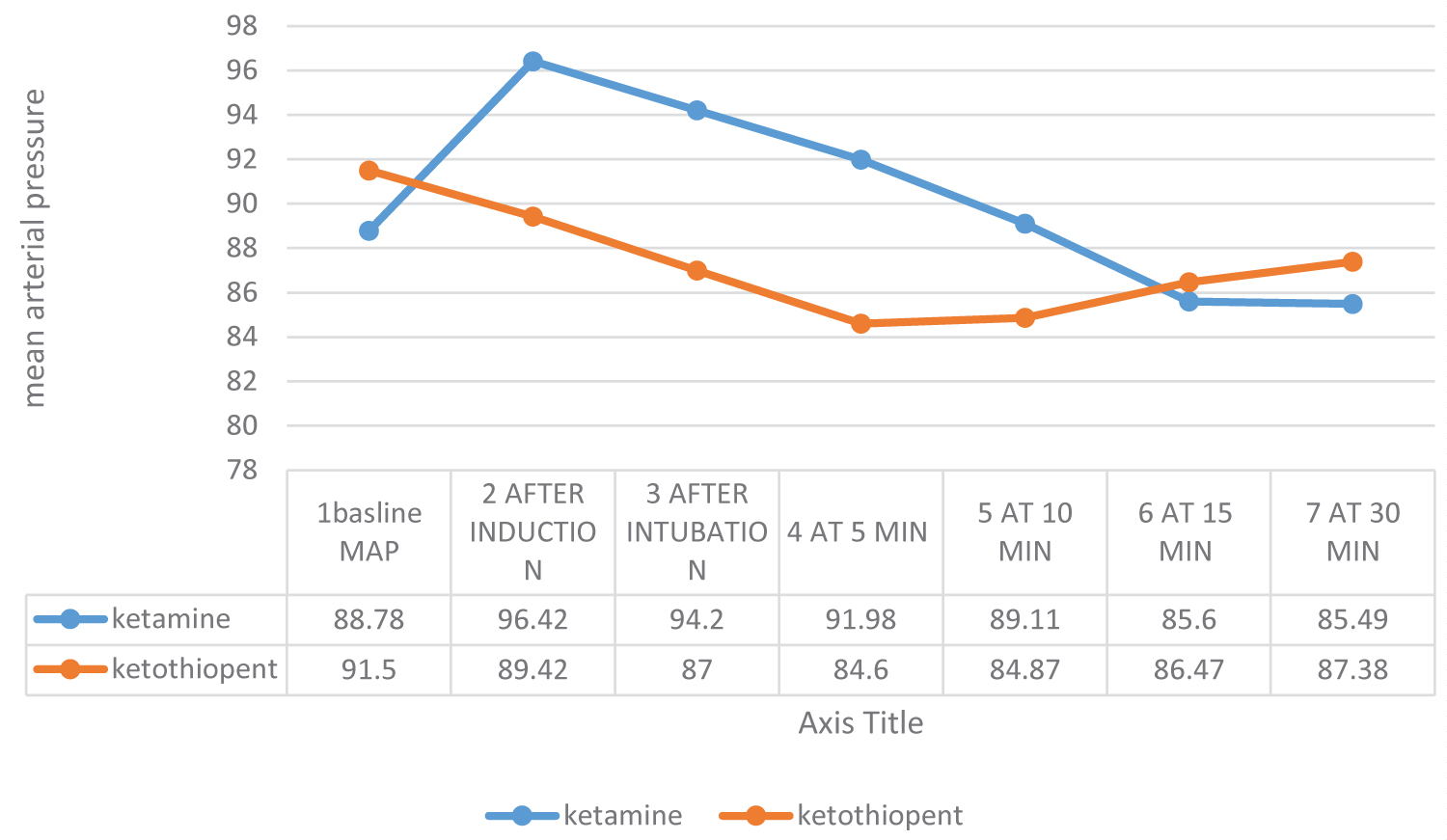 Figure 1: Change on mean arterial pressure between ketamine and ketamine with thiopental.
View Figure 1
Figure 1: Change on mean arterial pressure between ketamine and ketamine with thiopental.
View Figure 1
Before induction of anesthesia, there was no statistically significant difference (p-value 0.929) in HR between both groups. P values after induction up to five minutes were < 0.05 and that's statistically significant. With the induction of anesthesia, a significant rise in heart rate was observed in ketamine group (maximum 96.42 ± 13.08) from the baseline while in the ketamine-thiopental group, there was a maximum increment 88.71 ± 19.68 was observed at immediately after induction in heart rate (P < 0.05) (Figure 2).
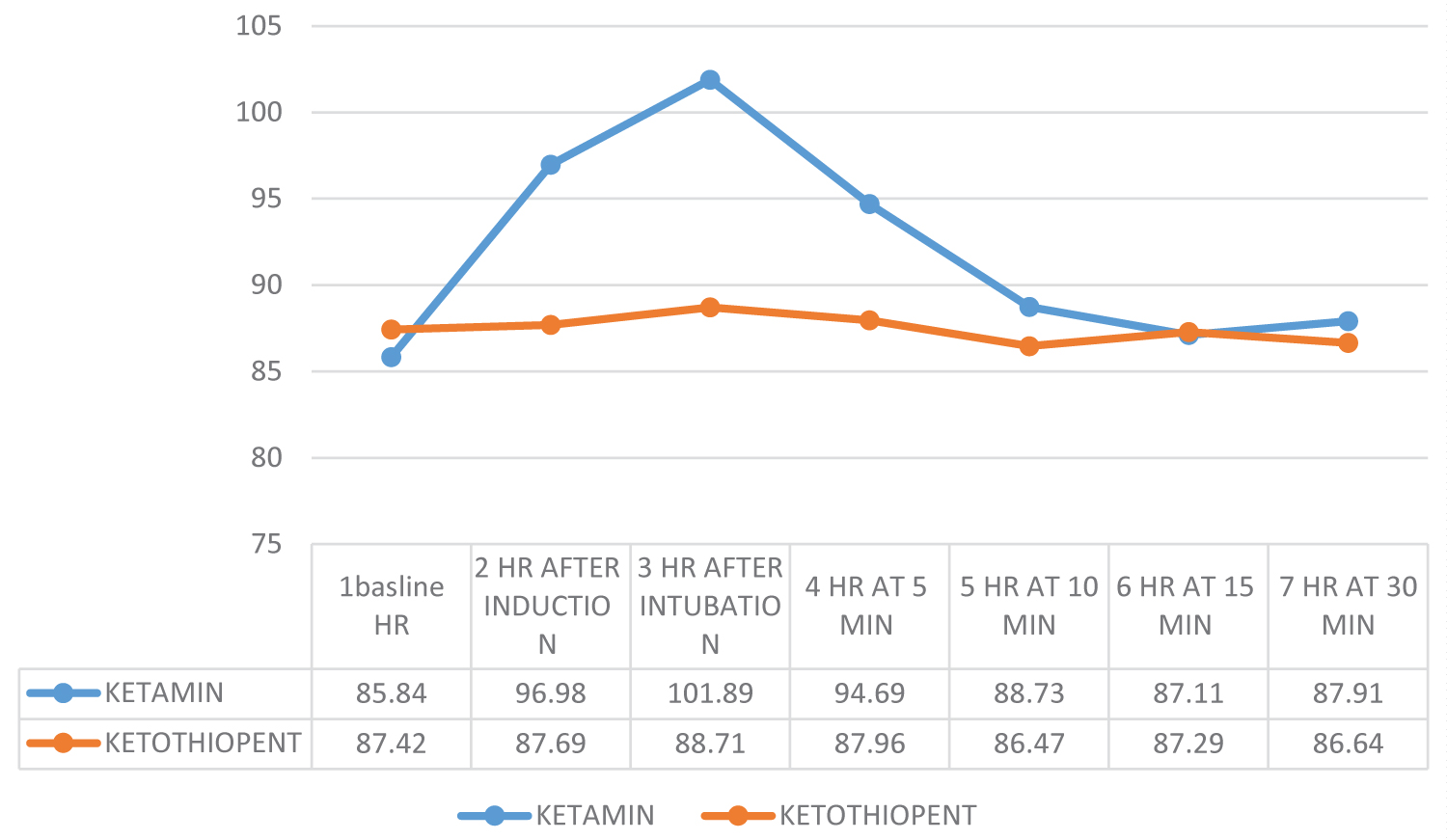 Figure 2: Heart rate change during the study in the two treatment groups.
View Figure 2
Figure 2: Heart rate change during the study in the two treatment groups.
View Figure 2
Systolic blood pressure was significantly different from baseline after induction, after intubation, 5 min, and 10 min, whereas after 10 min there was no significant difference between the group p-values of > 0.05. The greatest change observed after intubation was in ketamine group 133.42 ± 12.04, while all measurement time dropped in the ketamine-thiopental group.
Diastolic blood pressure was much different from baseline at post-induction and intubation, 5 min and 10 min in both groups, (P-value 0.001, 0.005, 0.000, and 0.008 respectively) higher DBP (79.82 ± 10.36) was measured immediately after induction of anesthesia in ketamine group and immediately after intubation were recorded in ketamine + thiopental group (73.2 ± 8.99) (Table 3).
Table 3: Hemodynamic variables in two treatment groups, mean and Standard deviation. View Table 3
In this study, we compared the effects of ketamine and ketamine with thiopental on hemodynamic stability in patients undergoing abdominal surgery with general anesthesia. In this study, ketamine with thiopental had better hemodynamic effects compared with ketamine alone.
According to Mehdi Dehghani Firoozabadi, et al. study, the pulse rate of patients in both groups before intubation, 1 minute, 3 minutes and 5 minutes after intubation showed that there is no significant difference between both groups (p > 0.05). The finding of this study is different from our result. PR was significantly increased in all measurement time in the ketamine group and the ketamine-thiopental group is stable. The p-value between the groups is statically significant at post-induction, intubation and after five minutes. Mehghania's study shows the result was the same with HR in diastolic blood pressure, i.e. without a significant difference, but it was significant in systolic blood pressure except in 1 minute after intubation with p = 0.04. But the result in our study is a significant difference in SBP and DBP post-induction up to ten minutes after induction (p-value > 0.05). The effect was attenuated by phantanile and midazolam was administered followed by induction agents [19].
Honarmand A and Safavi M compare the cardiovascular response of three different combinations of induction drugs, such as ketamine with thiopental (KT), thiopental with fentanyl (TF), and ketamine- fentanyl and thiopental (KFT) combination. After laryngoscopy, systolic, diastolic, and mean arterial pressures were significantly higher in the TF and TK groups compared with the TFK group (P < 0.05), the rank sequence is TK > TF > TFK. Heart rate was significantly higher in the TK group compared with TF and TFK groups after laryngoscopy (P < 0.05), the rank sequence is TK > TF > TFK [20].
HR is significantly increased after induction, post-intubation and after five minutes, 96.98 ± 13.08, 101.89 ± 12.64 and 94.69 ± 12.81 respectively in the ketamine group, but after ten minutes drop down to baseline (Table 3). In Ketamine-thiopental the HR was unchanged compared with pre-induction level but the statically significant difference is seen between two groups post-induction up to five minutes.
Studies compare the hemodynamic response to etomidate versus ketamine with thiopental sodium combination in coronary artery bypass graft surgery. Due to the conclusion of these studies, ketamine-thiopental reduces stress response for laryngoscopy and intubation, these findings support our result [6].
Research conducted by a Nigerian researcher called ZA Suleiman, et al, evaluated cardiovascular stimulation effects of ketamine. The main finding of these studies was the average peak increases of 34% in the pulse rate (PR), 22% in the systolic blood pressure (SBP), 24% in the diastolic blood pressure (DBP) and 23% in the mean arterial pressure (MAP) [21]. The result of this study was comparable with what our research finding shows in the group of ketamine.
Studies compare three induction agents, such as ketamine, thiopental and the combination of these two drugs. Systolic and diastolic blood pressures increased significantly in all groups (P < 0.05), except the combined group, where the average diastolic blood pressure did not increase significantly. During tracheal intubation or incision, heart rate increased in all groups, although to a lesser extent in the ketamine group. This study has similar results to our study. Change in hemodynamic parameters at the time of intubation was due to response to laryngoscopy and incision [22].
One study conducted in India that compared ketamine alone, thiopental alone and the combination of both ketamine and thiopental, do to the result of this studies there was no statically significant difference on socio-demographic parameters and pre induction variables across the group. However, post-induction values of systolic blood pressure were significantly higher for (Ketamine alone) P > 0.001, the difference between the groups was statistically significant (F = 7.13; df = 2.57; P = 0.002). These post-induction values are normalized at 30min. The results of these studies support our results except for time returns to the base line. The variability is due to physiological changes that occur during pregnancy, increased cardiac output and other responses to any change. After induction, diastolic BP increased significantly in all three groups. For 30 min, from the time of induction, diastolic BP (at 5 min intervals) was maximum in Groups ketamine and ketamine with thiopental, which was statistically significant (F = 3.6; df = 2.57, P = 0.034). The result is comparable to this result.
Heart rate at intubation, a rise in the thiopental group, and in the ketamine group, a decrease in heart rate was observed, while in the combination group there was no change. These intergroup variations were statistically significant. But our study showed, in the ketamine group, heart rate increased significantly immediately after induction, post intubation and at 5 minutes after induction of anesthesia [23]. The variability of heart rate observed in the ketamine group was due to analgesic effects of ketamine avoiding labor pine.
In conclusion, the use of a combination of the drug with ketamine has a better hemodynamic stability effect than using a single (ketamine or thiopental) induction agent.
We would like to thank Wolaita Sodo University for financial and other related support. We extend our gratitude to staffs, supervisor, data collectors, and respondents who participated on this study.
All authors contributed to the study conception and design. Material preparation, data collection, analysis and interpretation were performed by AAA, ZZK and BWD, first draft manuscript was written by AAA, ZZK, BWD, TDG, ADG and KEH. All the authors commented on the final version of the manuscript. All authors read and approved the final manuscript. AAA, ZZK and BWD contributed equally to this manuscript (shared first authorship).
Wolaita Sodo University had covered all financial costs for data collection instruments, data collection, data entry and Payments for supervisors and Advisors.
Data will be available with reasonable request from the corresponding author.
After taking approval from the Wolaita Sodo University and hospital Ethics review Committee and the study was registered as CHSM/ERC/103. The purpose of the study explain to the patient under the study and after obtained written informed consents, adult patients (ages from 18-60 years) included in these study. All information gathered was kept confidential. We are not including any identifiers, such as patient name or exact address. For participation, there is no specific benefit and if he or she find it not good, the patient have right quite the participation in between. For any condition that worsens patient health the appropriate treatment was given.
Not applicable.
The authors declare that they have no competing interests.