Introduction: PTSD is a mental health condition that can develop in some individuals who have experienced or witnessed a traumatic or life-threatening event. Previously, we identified a combination of blood biomarkers to differentiate controls from a PTSD cohort. This biomarker model could be used to diagnose and monitor treatment of PTSD, both behavioural and pharmacological. A recent publication questioned the health impact of selective serotonin reuptake inhibitors (SSRIs) which are used to improve mood, emotion and cognition and treat PTSD, and that long-term use of antidepressants may decrease serotonin levels. The action of SSRIs may potentially impact astrocytes and damaged astrocytes release GFAP into the bloodstream. In our previous study, GFAP did not contribute to the model. The aim of the current study was to revisit the previous data and to determine whether there were differences in GFAP levels between control and PTSD individuals and to determine levels of serum GFAP in individuals prescribed SSRIs.
Materials and methods: Study participants were recruited in the US between January 2019 and June 2019. In total, N = 40, age and sex matched individuals were included; n = 20 controls and n = 20 clinically diagnosed with PTSD. Informed consent was obtained from all individuals. Venous blood samples and a detailed clinical history including current medications, were obtained from all individuals. Levels of serum GFAP were measured in duplicate in samples at Randox Clinical Laboratory Services (RCLS) (Antrim, UK) using the Cerebral Array I on a Randox Investigator according to manufacturer's instructions (Randox Laboratories Ltd, Crumlin, UK). Statistical analyses were performed using R Version 3.5.1, and IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp, Armonk, New York).
Results: Control and PTSD individuals were matched for age (39.0 ± 2.64 vs. 41.5 ± 11.0 years, p = 0.386), gender (10/20 (50%) vs. 9/20 (45%), male/female, p = 0.752) and BMI (29.7 ± 7.9 vs. 27.9 ± 6.3, p = 0.496), respectively. Serum GFAP levels were not significantly different between the control (627.0 ± 355.4 pg/ml, n = 20) and the PTSD group (963.7 ± 732.5 pg/ml, n = 20) (p = 0.196); albeit there was a trend for GFAP levels to be higher in the PTSD group. However, across the full cohort (i.e., controls and PTSD) individuals prescribed SSRIs has significantly higher GFAP levels than individuals not prescribed SSRIs (1042.8 ± 715.4 pg/ml, n = 15 vs. 646.9 ± 460.6 pg/ml, n = 25, respectively) (p = 0.041).
Conclusion: This study demonstrated that serum GFAP levels were not significantly different between the control and PTSD group; albeit there was a trend for GFAP levels to be higher in the PTSD group. However, across the whole cohort, individuals prescribed SSRI medications had significantly higher levels of serum GFAP compared to individuals not taking SSRIs. Since elevated serum GFAP levels can be used for diagnosis of Alzheimer's Disease, and antidepressant use is significantly associated with an increased risk of developing dementia, monitoring of GFAP levels in individuals prescribed an SSRI is warranted.
GFAP, selective serotonin reuptake inhibitor, SSRI, post-traumatic stress disorder
Previously, we measured several biomarkers in serum, including GFAP (an intermediate filament protein that has a key role in astrocytic processes that aid in regulation of neuron synapses) to identify differential expression of protein biomarkers between a control and post-traumatic stress disorder (PTSD) cohort [1]. PTSD is a mental health condition that can develop in some individuals who have experienced or witnessed a traumatic or life-threatening event. These events may include natural disasters, serious accidents, combat situations, sexual assault, or any form of violence. PTSD can affect anyone, regardless of age, gender, or background.
Three biomarkers were identified in our previous study, namely, EGF, tPA and IL-8, which when combined into a single model, differentiated control individuals from patients clinically diagnosed with PTSD. This novel biomarker combination has the potential to be used to assist in patient diagnosis and monitor treatment efficacy, both behavioural and pharmacological e.g., cognitive behaviour therapy, talking therapies, selective serotonin reuptake inhibitors (SSRIs) and selective noradrenaline reuptake inhibitors (SNRIs).
SSRIs block reabsorption (reuptake) of serotonin, the chemical responsible for carrying signals between neurons. The increased serotonin is reported to affect mood, emotion, and cognition [1]. However, recently it has been suggested that serotonin levels may not play a role in depression and that long-term use of antidepressants may decrease serotonin levels [3]; studies suggest that SSRIs may have neurotrophic effects, influencing the growth and survival of neurons [4,5]. These effects potentially impact astrocytes [6], which when damaged could release GFAP into the bloodstream [7,8] or alter astrocyte activity [9].
GFAP has been observed in blood following brain injury/stroke and other neurodegenerative disorders including incident dementia and Alzheimer’s disease [8,10-14]. Moreover, it has also been reported that levels of GFAP are elevated in individuals with PTSD. However, the findings are not consistent across studies, and more research is needed to establish a clear and reliable connection [15,16]. To investigate this issue, we examined GFAP levels in a pilot cohort who were diagnosed with PTSD and taking SSRIs and determined GFAP levels in individuals who were prescribed an SSRI irrespective of their PTSD diagnosis.
Details of study participants, psychological and psychiatric assessment, clinical characteristics, sampling, and laboratory methods have been published previously [1]. In brief, study individuals were recruited in the US between January 2019 and June 2019. In total, N = 40, age and sex matched individuals were involved in the pilot study; n = 20 control individuals, and n = 20 clinically diagnosed individuals with PTSD. Informed written consent was obtained from all participants. Venous blood samples and a detailed clinical history (and current medications) were obtained from all individuals. The study conformed to all Data Use Agreements (DUA). Individual samples were deidentified and publicly available and are thus exempt from the requirement of the Institutional Review Board (IRB) approval (Exempt Category 4).
As detailed previously [1] GFAP was measured in duplicate at Randox Clinical Laboratory Services (RCLS) (Antrim, UK), using the Cerebral Array I on an Evidence Investigator according to manufacturer’s instructions (Randox Laboratories Ltd, Crumlin, UK). The limit of detection (LOD) for GFAP was 180 pg/ml and GFAP values below the assay LOD were recorded as 90% of LOD.
Statistical analyses were performed using R Version 3.5.1, and IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp, Armonk, New York) [17]. Continuous variables are presented as mean ± standard deviation (mean ± SD). Comparisons were made using the Wilcoxon rank sum test and Kruskal-Wallis. Categorical variables are presented as percentage (%) and were compared using a 2-sample test for equality of proportions without continuity correction. A p value < 0.05 was considered significant.
Patient demographics have been described elsewhere [1]. Briefly, the control and PTSD individuals were matched for age (39.0 ± 2.64 vs. 41.5 ± 11.0 years, p = 0.386), gender (10/20 (50%) vs. 9/20 (45%), male/female, p = 0.752) and BMI (29.7 ± 7.9 vs. 27.9 ± 6.3, p = 0.496), respectively. Unsurprisingly, the control individuals were prescribed fewer medications when compared to the individuals in the PTSD group (1.1 ± 1.4 vs. 3.2 ± 2.8, p = 0.008), respectively.
Four (20%) of the individuals in the control group were prescribed SSRIs. However, in the PTSD group, 11 (55%) were prescribed SSRIs; almost a 3-fold increase (p = 0.022).
Serum GFAP levels were not significantly different between the control (627.0 ± 355.4 pg/ml, n = 20) and the PTSD group (963.7 ± 732.5 pg/ml, n = 20) (p = 0.196) (Table 1). However, when the serum GFAP levels were compared between all participants, individuals prescribed SSRIs has significantly higher GFAP levels (1042.8 ± 715.4 pg/ml, n = 15 vs. 646.9 ± 460.6 pg/ml, n = 25, respectively) (p = 0.041) (Table 2).
Table 1: Serum GFAP levels in control and PTSD individuals. View Table 1
Table 2: Serum GFAP levels in individuals prescribed SSRIs. View Table 2
When the n = 40 individuals were assessed based on whether they were diagnosed with PTSD and were prescribed an SSRI(s), four groups were identified (PTSD 0 and SSRI 0; PTSD 0 and SSRI 1; PTSD 1 and SSRI 0; PTSD 1 and SSRI 1; where 0 = negative and 1 = positive). There was no significant difference in the levels of GFAP across the 4 groups (Kruskal-Wallis p = 0.098) (Table 3 and Figure 1). However, there was a trend for GFAP levels to be higher in the PTSD 0 and SSRI 1 group when compared to the PTSD 0 and SSRI 0 group.
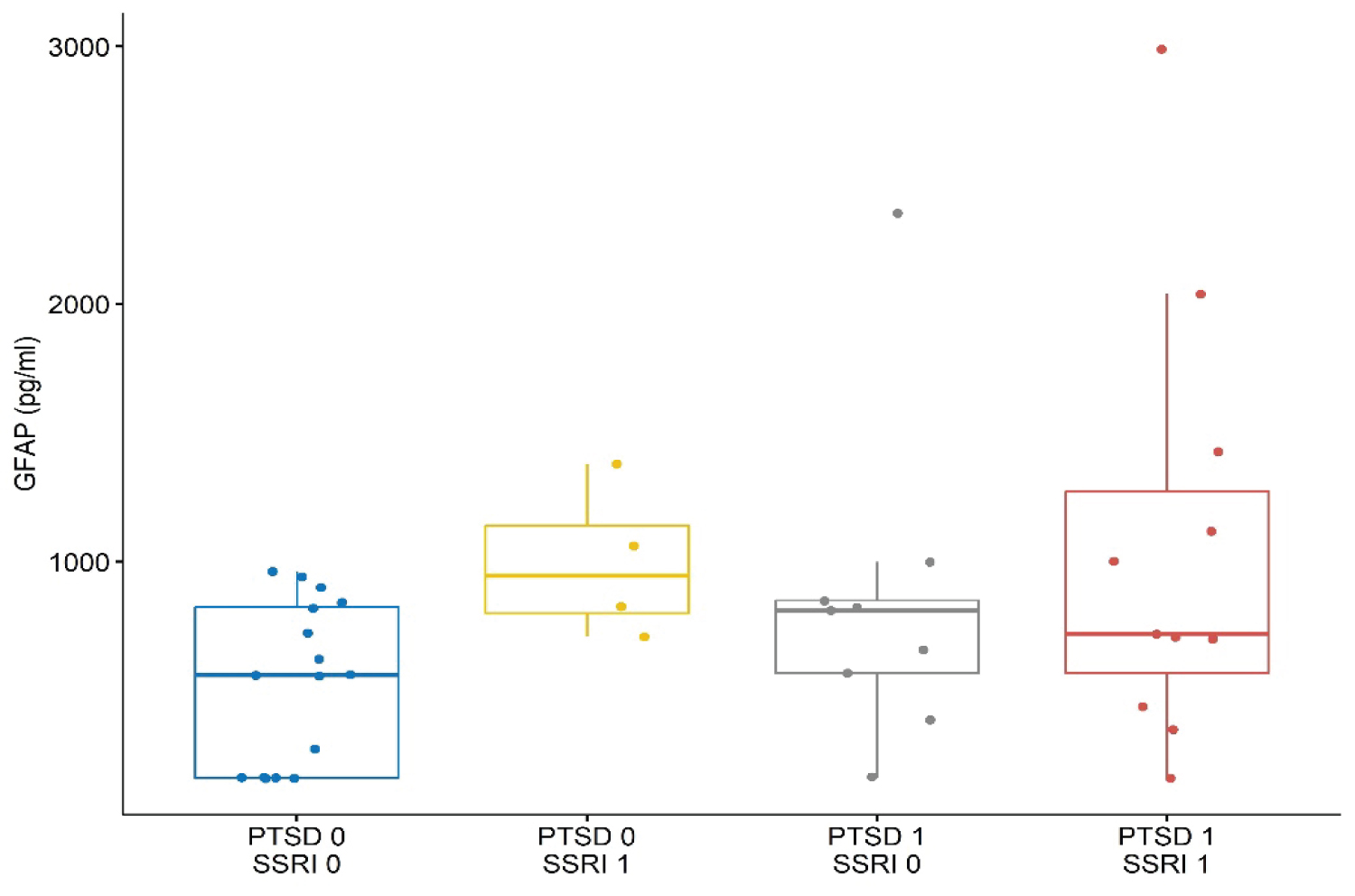 Figure 1: Serum GFAP levels across all groups.
View Figure 1
Figure 1: Serum GFAP levels across all groups.
View Figure 1
Table 3: Serum GFAP levels based on the combination of a PTSD diagnosis and prescribed SSRI medication. View Table 3
Treatment of PTSD involves both behavioural and pharmacological interventions e.g., SSRIs and SNRIs; however, the mechanism of action of SSRIs has recently been called into question and the theory that elevated serotonin improves mood is under scrutiny [3]. Previously, we measured serum biomarkers in individuals with PTSD, many of whom were prescribed SSRIs. One of the biomarkers investigated was GFAP, known to be linked to astrocyte damage. The aim of this study was to evaluate if GFAP levels varied between individuals prescribed an SSRI and those not taking a SSRI.
The results demonstrated that serum GFAP levels were not significantly different between the control and the PTSD individuals. However, across the whole cohort of individuals, serum GFAP levels were significantly higher in individuals prescribed SSRIs. Interestingly, there was no significant difference in the levels of GFAP when the cohort was divided into four groups based on whether they had PTSD and were prescribed SSRIs (p = 0.098) (Table 3 and Figure 1). However, there was a trend for GFAP levels to be higher in the PTSD 0 and SSRI 1 group when compared to the PTSD 0 and SSRI 0 group.
Antidepressants are the most common type of medication prescribed in the UK and SSRIs are the most prescribed type of antidepressant [18]. In 2022/23, over 80 million antidepressants were prescribed to an estimated 8.6 million patients in the UK, representing an increase of 200,000 more patients than 2021/22 [19]. Potentially almost 15% of the population in England received at least one prescription item for an antidepressant drug in 2021/2022 [20]. Interestingly, it has been calculated that the total unnecessary (i.e., non-indicated or dispensable) spend on antidepressants for 2021 was between £37-£46 million [21]. Unsurprisingly, reducing wasteful healthcare practices has become a priority for healthcare, including the UK’s National Institute for Health and Clinical Excellence (NICE) and the US Preventive Services Task Force [22].
SSRIs are generally the first-choice medicine for treatment of depression (UK) because they have less side effects that other antidepressants [23] and treatment usually continues for at least 6 months. However, some individuals may be prescribed SSRIs indefinitely if they have recurrent problems [23]. Recent reports have suggested that there is a potential link between cognition and incident dementia in patients that have been prescribed SSRIs [12-14] which highlights the need for constant review of medications and a requirement to implement deprescribing. However, it is common for individuals on all classes of dependency-forming drugs to experience severe withdrawal symptoms. For those trying to discontinue antidepressant medications, withdrawal symptoms are reported to affect > 50% of individuals, and up to a quarter of these individuals have reported severe withdrawal symptoms [24].
There is growing evidence which suggests a link between cognitive impairment and SSRI use. Although SSRIs can be used long-term, ideally once an individual’s crisis is alleviated, prescribing should gradually be reduced. In this study, the average age of individuals was 40 years and over one third of the individuals were prescribed SSRIs. It is of concern, that individuals taking SSRIs for many years are at potential risk of cognitive impairment. We propose that serum GFAP levels have the potential to be used to monitor decline in cognitive function related to SSRIs use. Our results suggest that a longitudinal study is warranted.
This study demonstrated that serum GFAP levels were not significantly different between the control and the PTSD group; albeit there was a trend for GFAP levels to be higher in the PTSD group. However, across the whole cohort, individuals prescribed SSRI medications had significantly higher levels of serum GFAP compared to individuals not taking SSRIs. Since elevated serum GFAP levels can be used for diagnosis of Alzheimer’s Disease and antidepressant use is significantly associated with an increased risk of developing dementia, monitoring of GFAP levels in individuals prescribed an SSRI is warranted.
The limitations of the study have been reported previously [1].
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests, Mary Jo Kurth, Joanne Watt, Paul Innocenzi, Laura Mooney, John Lamont, and Mark Ruddock are employees of Randox Laboratories Ltd but hold no shares in the Company. Peter Fitzgerald is the Managing Director of Randox Laboratories Ltd.
Randox have submitted a patent application to protect the biomarkers disclosed in the manuscript (Patent No. PCT/EP2020/081273).
The authors would like to thank the individuals who gave their time and consent to take part in the study.