Background: The aim of this study was to investigate the differences in radiological and neurological improvement between the groups that underwent suboccipital craniectomy with and without duraplasty.
Materials and methods: In this study, 46 patients who were operated on for Type I Chiari malformation (CM) in our clinic since 2010 were included. The preoperative and postoperative cranial and spinal MRI examinations of all patients were compared between the two groups in terms of hydrocephalus, tonsillar herniation level, the presence and level of syringomyelia, osseous anomalies, postoperative cisterna magna formation, postoperative obex structure, and syringomyelia status.
Results: Twenty-two (47.8%) of the patients were found to have syringomyelia at the time of hospital admission. Suboccipital craniectomy (SC) was performed on 29 patients (63%), and suboccipital craniectomy with duraplasty (SCD) was performed on 17 patients (37%). According to the assessment of the clinical improvement levels of the patients, in the SC group, 14 patients (50%) had moderate improvement and 14 (50%) had complete/near-complete improvement. In the SCD group, 8 patients (47.1%) showed complete/near-complete clinical improvement, 6 (35.3%) showed moderate clinical improvement, 2 (11.8%) showed no clinical improvement, and 1 (5.9%) had clinical decline.
Conclusion: Patients should be informed elaborately about the advantages and disadvantages of the surgical methods while deciding which method to be applied. The present study suggests that deciding the treatment method together with patients would help avoid medicolegal problems.
Chiari malformation, Duraplasty, Suboccipital craniectomy, Syrinx, Functional outcome
CSF: Cerebrospinal Fluid; CM: Chiari Malformation; SCD: Suboccipital Cranioectomy with Duraplasty; SD: Suboccipital Cranioectomy without Duraplasty; SPSS: Statistical Package for the Social Sciences; MRI: Magnetic Resonance Imaging
Type I Chiari malformation (CM), a developmental anomaly, was first described by Hans Chiari in 1891 as the caudal displacement of the tonsils [1-5]. Cerebellar tonsils descending over 3 mm in children and over 5 mm in adults through the foramen magnum are described as Type I CM [3,4]. Its natural course is not well known in symptomatic and asymptomatic people who do not receive surgical treatment. According to various studies, CM Type I was detected in 1% of the cranial and cervical MRI examinations and was accompanied by syringomyelia in 50%-75% of the patients and hydrocephalus in 1%-3% [6-10]. When deciding on the surgical treatment and planning patient management, the presence of syringomyelia and neurosurgical interventions are two crucial markers to consider [8,10-13].
The most common symptom for hospital admission is tussive pain in the occipital and cervical regions aggregated by the Valsalva maneuver [4,14]. The majority of patients with symptomatic CM Type I are treated surgically [13,15-17]. Although many techniques are employed in surgical treatment, among the most common techniques are suboccipital craniectomy, C1 laminectomy, tonsil resection, craniocervical decompression with duraplasty, endoscopic third ventriculostomy, and restoration of the cerebrospinal fluid (CSF) flow [8,10,13,15-19]. Currently, minimally invasive procedures are preferred since they are associated with fewer complications, a shorter operative time, and a shorter hospital stay. Therefore, the technique of suboccipital craniectomy without duraplasty (SC) has gained more popularity [13,15-17]. Although there is no clear consensus on surgical techniques of suboccipital craniectomy with duraplasty (SCD) and SC is superior, some argue that there is no complete improvement in the symptoms or the radiological findings because the arachnoid bands cannot be released in SC [13,15-17]. SC is a technique that has recently been applied in an increasing number of cases, and it is also associated with an increase in the number of cases requiring second surgery after SC [10,13,16].
Recently, there has been a radical increase in the number of clinical trials focusing on these two surgical techniques [16,20,21]. In consideration of the ongoing uncertainties associated with these techniques, our study has shed light on their outcomes from a different perspective.
This single-center, retrospective study was conducted upon the approval obtained from the university’s local ethics committee (22.11.2018, 2018/ 14-10). Patients who underwent surgery for Type I CM in our clinic since 2010 were evaluated retrospectively.
A total of 46 patients who underwent surgery for Type I CM at our clinic since 2010 were retrospectively analyzed for demographic characteristics, symptoms, radiological findings, surgical treatment, and treatment outcomes. Axial and sagittal sections of pre- and postoperative cranial and spinal Magnetic Resonance Imaging (MRI) examinations of all patients were evaluated by a neuroradiologist who was unaware of the surgery. Measurements were made in the sections with the largest syringomyelic diameters. The syrinxes were grouped as cervical, cervicothoracic, and holocord syrinxes based on the level at which they were detected in the imaging examinations of the patients. Cranial and spinal MRI examinations in patients with hydrocephalus, tonsillar herniation level, the presence and level of syringomyelia, osseous anomalies, postoperative cisterna magna formation, postoperative obex structure, and syringomyelia were evaluated for radiological changes in the postoperative period. The demographic, clinical, and radiological data were found to be evenly distributed between the two groups of patients treated with two different surgical techniques.
Patients were treated with either the SC or SCD technique. The groups of patients treated with either SC or SCD were then analyzed for any differences in terms of clinical course, syringomyelia status, cisterna magna formation, and obex structure during the postoperative period.
Postoperative physical examination findings, symptoms, and radiological examinations were retrospectively evaluated. The patients were divided into three groups based on their syringomyelia status during the postoperative period: Those whose syringomyelia shrank (group 1), remained unchanged (group 2), or grew (group 3) in comparison to the preoperative state of their syrinxes. The patients were also divided into four groups based on their level of postoperative clinical improvement: patients with deterioration (group i), no clinical improvement (group ii), moderate improvement (group iii), and complete/near-complete improvement (group iv). They were also divided into three groups according to postoperative cisterna magna formation: Patients with no cisterna magna formation (group a), minimal formation (group b), and sufficient formation (group c).
Both surgical treatments were evaluated for their effects on clinical improvement and radiological findings in Type I CM. Additionally, the two groups of SCD- and SC-treated patients were compared in terms of treatment outcomes based on their examination of tonsillar herniation level, the presence of syringomyelia, clinical improvement level, and postoperative radiological findings.
In descriptive statistics, the continuous data are shown as mean, standard deviation, median, and minimum and maximum values.
To statistically compare the data, the Kolmogorov-Smirnov analysis was performed to determine whether the continuous data were normally distributed or not. To compare continuous data between independent groups, Mann-Whitney U test was applied for the comparison of two groups. Chi-square test was performed to compare the categorical data. McNemar’s test was conducted to compare the preoperative and postoperative results between dependent groups.
p < 0.05 in the 95% confidence interval was considered statistically significant. Statistical Package for the Social Sciences (SPSS) v21.0 program was used to conduct the statistical analysis.
Of the 46 patients with Type I CM in our study, 25 (54.3%) were female and 21 (45.7%) were male. They had a mean age of 33.8 years and a mean postoperative follow-up period of 31.2 months.
Of all the symptoms and findings of the patients at the time of admission, headache was reported in 25 patients (54.3%) and was found to be the most common symptom in our study. Twenty-three (50%) of the patients had sensory deficits, 19 (41.3%) had motor deficits, 18 (39.1%) had pain (excluding headache and neck pain), 16 (34.8%) had cerebellar involvement, 16 (34.8%) had upper/lower motor neuron involvement, 6 (13%) had cranial nerve involvement, 2 (4.3%) had hydrocephalus symptoms, and 1 (2.2%) had sphincter disorders (Table 1).
Table 1: Symptoms of type I chiari malformation and preoperative radiological findings. View Table 1
MRI examinations of the patients revealed that 22 (47.8%) had syringomyelia at the time of hospital admission. 10 (21.7%) had cervical synrix, 10 (21.7%) had cervithorocic syrinx, and 2 (4.3%) had holocord syrinx. Regarding the preoperative tonsillar herniation levels, 25 patients (54.3%) were found to have tonsillar herniation at C1, 7 (15.2%) at the C1-C2 junction, 7 (15.2%) at the foramen magnum-C1 junction, 6 (13.0%) at C2, and 1 at the C2-C3 junction (2.2%). In the preoperative MRI examinations of the patients, 38 (82.6%) had cisterna magna and 29 (63.0%) had obex. Additionally, 1 patient (2.2%) in our study had accompanying platybasia and 1 (2.2%) had accompanying scoliosis (Table 1).
Of the patients included in our study, SC was performed in 46 and SCD in 17 (37.0%) (Table 2). The remaining 29 patients (63.0%) were operated on using the SC technique. The clinical improvements and postoperative radiological changes obtained by the two surgical techniques were then evaluated and compared.
Table 2: Surgical techniques applied. View Table 2
There were no statistically significant differences between the two groups when age, gender, clinical status at the time of admission, obex structures in preoperative MRI imaging, presence of cistern, the presence and level of syringomyelia, and postoperative follow-up periods were compared (Table 3 and Table 4).
Table 3: Relationship between the surgical techniques and symptoms. View Table 3
Table 4: The relationship between postoperative radiological findings and surgical techniques applied. View Table 4
The two groups were compared in terms of the preoperative locations and incidence of syringomyelias and the tonsillar herniation levels (Table 5). Of the patients undergoing SCD, 9 (52.9%) had syringomyelia that was most localized as cervical syrinxes (29.4%). In the SC group, 13 patients (44.8%) were found to have syringomyelia that was most located in the cervicothoracic region (24.1%). The most common level of tonsillar herniation was the C1 level in both groups. According to the analyses of these findings, the two groups had similar distributions.
Table 5: Relationship between syrinx location. tonsillar herniation level. and surgical technique. View Table 5
Regardless of the applied surgical technique, the patients were postoperatively examined via MRI for clinical improvement, the presence of syringomyelia, cisterna magna formation, and obex structures (Table 6). In total, 22 patients (48.9%) had complete or near-complete improvement in their complaints, 20 (44.4%) had mild/moderate improvement, and 2 (4.4%) had no change in their clinic status. Only 1 patient (2.2%) experienced clinical decline. In the control imaging of this patient, hydrocephalus developed as a complication, leading to clinical decline. As a result, ventriculoperitoneal shunting was performed.
Table 6: Analysis of postoperative clinical improvements and radiological findings. View Table 6
According to the postoperative MRI imaging, syringomyelia decreased in 13 patients (56.5%) patients, remained unchanged in 9 (39.1%), and developed in 1 (4.3%) during the postoperative period. While cisterna magna was not present in 38 patients (82.6%) during the preoperative period, 20 patients (43.5%) had minimal formation of cisterna magna in the postoperative period and 18 (39.1%) had sufficient formation. In the preoperative MRI examination, the obex structure was present in 17 patients (37%). During the postoperative period, the number of cases with the presence of obex structures reached 39 (84.8%).
Postoperative clinical improvement levels, cisterna magna formation levels, and changes in syringomyelias and obex structures observed in the postoperative MRI examinations were evaluated in the two groups (Table 7).
Table 7: Histogram of parenchyma of healthy lungs in male group. View Table 7
According to the assessment of the clinical improvement levels of the patients, in the SC group, 14 patients (50%) had moderate improvement and 14 (50%) had complete/near-complete clinical improvement. In the SCD group, 8 patients (47.1%) were found to have complete/near-complete clinical improvement, 6 (35.3%) had moderate clinical improvement, 2 (11.8%) had no clinical improvement, and 1 (5.9%) experienced clinical decline. Clinical improvement was observed with both surgical methods. However, there was not a statistical significance (p = 0.094).
Postoperative cisterna magna formation was observed in 5 patients (17.2%) in the SC group and 13 (76.5%) in the SCD group. Although postoperative cisterna magna formation has been also observed in both groups, it was observed in a higher number and sufficient size in the SCD group and was statistically significant (p < 0.001).
In the postoperative MRI examination, the obex structure was present in 23 patients (79.3%) in the SC group and in 16 (94.1%) in the SCD group. Although the radiological improvement was higher in the SCD group, the difference was not statistically significant (p = 0.234). The number of patients with no preoperative obex structure decreased by 68.4% in the SC group and by 90% in the SCD group (Table 7). These results were found to be statistically significant (p < 0.001 and p = 0.004, respectively).
The regression in syringomyelia on postoperative MRI is the most objective indicator of surgical benefit. According to the postoperative MRI examination, the syringomyelia disappeared significantly in 5 patients (38.5%) in the SC group and in 8 (80%) in the SCD group. In Figure 1, which demonstrates the postoperative MRI of a patient operated with the SCD technique at our clinic and included in our study, it can be observed that syringomyelia disappeared completely. In the SCD group, syringomyelia was found to remain unchanged in 1 patient (10%), whereas the number of patients with unchanged syrinx was 8 (61.5%) in the SC group. Syringomyelia was found to be increased postoperatively in 1 patient (10%) who underwent SCD. The radiological improvement of syringomyelia was higher in the SCD group and was found to be statistically significant (p = 0.019). According to statistical analyses, the sample size for group comparisons is quite a small number. The results can therefore be considered preliminary and may provide guidance for further studies conducted to test this hypothesis in larger groups.
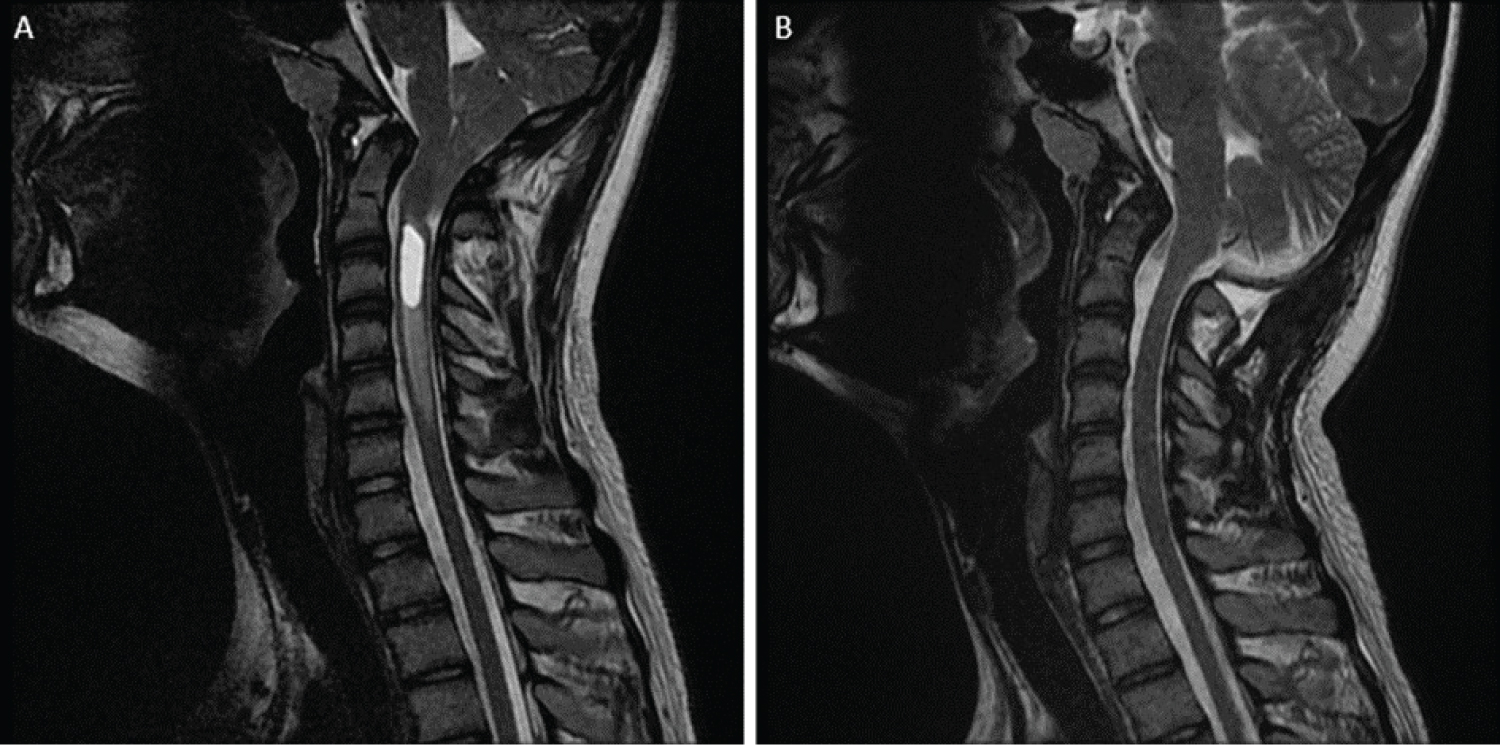 Figure 1: A) Preoperative Magnetic Resonance Imaging (MRI) of the patient diagnosed with Type I CM reveals tonsillar herniation and syrinx; B) Postoperative MRI of the patient undergoing suboccipital cranioectomy with duraplasty surgery reveals that the syrinx completely disappeared.
View Figure 1
Figure 1: A) Preoperative Magnetic Resonance Imaging (MRI) of the patient diagnosed with Type I CM reveals tonsillar herniation and syrinx; B) Postoperative MRI of the patient undergoing suboccipital cranioectomy with duraplasty surgery reveals that the syrinx completely disappeared.
View Figure 1
The rates of postoperative MRI syrinx status change were found to vary at a statistically different level between the two surgical techniques (p = 0.019). According to the posthoc pairwise comparisons, the SCD group had a higher rate of patients who improved postoperatively (group 1) and a lower rate of patients who remained unchanged postoperatively (group 2). The two surgical techniques did not have any statistically significant difference in terms of the rates of patients with clinical decline (group 3). The sample size for group comparisons for statistical analyses is quite small, which is a limitation of the study. The results can therefore be considered preliminary and may provide guidance for further studies conducted to test this hypothesis in larger groups.
Type I CM is a congenital or acquired condition where cerebellar tonsils herniate toward the spinal canal, and surgical treatment is required after the onset of symptoms. Its treatment prioritizes clinical recovery. However, the presence of syringomyelia, whose pathophysiological mechanisms are still unknown, is another important indicator for deciding the surgical treatment in symptomatic patients [8,13,22,23].
Suboccipital craniectomy is the main step of Type I CM treatment. Suboccipital craniectomy can also be accompanied by C1 or C2 laminectomy and tonsillar coagulation. However, it is still controversial whether decompression should be performed with or without duraplasty [8,18,22,24-26]. Various treatment methods have been accepted and are applied by different healthcare centers. The results from the comparisons of different approaches in the literature show that no clear consensus has been reached. According to the analyses conducted regardless of the applied surgical technique, 22 patients (48.9%) had complete or near-complete improvement and 20 (44.4%) had mild/moderate improvement in their complaints during the postoperative period. The rates of symptomatic improvement were similar to those in the literature [8,22,27].
Type I CM is known to be accompanied by syringomyelia in the imaging examinations of 20%-70% patients with Type I CM. In our study, this rate was found to be 47.8%, similar to that reported in the literature [6-9,28]. In some patients accompanied by syringomyelia, the neurological clinical findings were reported to be worse [29,30]. One of the objectives of the current treatment is to treat syringomyelia [31]. However, the improvement in complaints and the shrinkage of the syringomyelia following the treatment may not always go hand in hand [26]. Some studies have reported that the SCD technique achieved better results in the presence of syringomyelia [7,32,33]. In our study, we also observed that SCD technique outcomes were better in the presence of syringomyelia. In the literature, the rates of radiological improvement after treatment ranged from 44% to 100%, while the rates of clinical improvement ranged from 35% to 100% [34].
The presence of syringomyelia is an important marker to be considered while making the surgical treatment decision. The SCD technique can lead to improved outcomes in patients since it achieves more effective decompression and better restoration of the CSF flow if applied in the presence of syringomyelia. However, there is no significant correlation between the shrinkage in syringomyelia size and the degree of clinical improvement alone [7,16,35]. Similarly, clinical improvement was found to be similar in both groups. In a meta-analysis comparing the SC and SCD techniques, it was shown that there was no significant difference between the two techniques in terms of radiological and clinical improvements [7]. However, syringomyelia shrinkage is considered an indication of sufficient decompression, and a lack of syringomyelia shrinkage is considered a poor prognostic indicator in the long run [8]. The primary objective of medical treatments should be to ensure the patient’s recovery. Radiological improvement after treatment may not always guarantee patient recovery. Therefore, both clinical and radiological findings should be evaluated simultaneously when deciding the surgical technique to be applied.
In many studies in the literature, it is stated that patients who were treated via the SC technique had persistent symptoms and required a second surgical treatment [8,16,17,32,36]. Yeh, et al. also reported that the group of patients operated on with duraplasty had better radiological and clinical improvement [7]. Based on these studies, it may be considered that duraplasty should be incorporated into the surgical treatment for effective decompression. There could be numerous explanations for why duraplasty, a simple procedure for a neurosurgeon, may not always have been preferred. The first may be to shorten the operation time. Shorter operation times can be perceived as a positive situation for the surgeon, anesthesiologist, and patient. It was also observed that the incidence of CSF fistula was higher in patients who were operated using the SCD technique [16,18,24,26,37]. CSF fistulas can persist long enough to be difficult and inconvenient for both the neurological surgeon and the patient, leading to serious complications. Recurrent suturing, drainages, and repeated surgical interventions may be required for their treatment. Each case of CSF fistula is accompanied by the risk of infection. In other words, it can become a condition that adversely affects mortality and morbidity. Another problem is the formation of pseudomeningoceles. The incidence of this undesired complication is approximately 10 times lower in patients with SC than in those operated with duraplasty, and this complication usually requires primary repair [7,38]. Both of the methods have their own advantages and disadvantages. However, to avoid cerebellar slump syndrome, the decompressive craniectomy area should not exceed 4 × 4 cm [10].
According to the postoperative radiological examinations of the patients for cisterna magna formation and obex structure, the SCD technique was notably superior to the SC technique in terms of cisterna magna formation during the postoperative period. This difference between the two techniques was statistically significant. Additional duraplasty achieves better decompression and consequently leads to a further increase in CSF flow. Although the postoperative obex structure was also better in the SCD group, the difference was not statistically significant.
There is still no clear information in the literature about the superiority of these surgical techniques. Therefore, it is crucial to inform the patient thoroughly about the treatment method and obtain their consent.
This retrospective study has shown that both clinical and radiological findings are the most important markers to be considered while deciding the surgical technique to be applied to treat patients with Type I CM. In particular, there was not enough improvement in the radiological and clinical findings of those patients operated with the SC technique in the presence of syringomyelia. Patients should be informed elaborately about the advantages and disadvantages of the surgical methods before deciding on the method to be applied. According to the findings of this study, deciding on a treatment method with patients can help avoid medicolegal issues.
We/The authors thank Enago - https://www.enago.com.tr/ceviri/ for their assistance in manuscript translation and editing.
Mahmut Camlar: Writing and editing the manuscript, data collection; Mustafa Eren Yuncu: Literature search and collected data; Ali Karadag: Literature search and collected data; Merve Oren: Data collection; Caglar Turk: Data collection; Ozgur Oztekin: Editing and revised the manuscript; Fusun Ozer: Editing and revising the manuscript.
The authors declare no competing financial interests and no sources of funding and support, including any for equipment and medications.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (name of institute/committee) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required. Approval no: 2018/14-10 (Ethical Committee of the Health Science University İzmir Tepecik Research and Training Hospital).