Hemifacial spasm, Blepharospasm, Trigeminal neuralgia, Neurovascular compression of the Vth nerve
Blepharospasm (BB) in an involuntary movement disorder characterized by stereotyped, bilateral, and synchronous spasms of the orbicularis oculi (OO) muscles. Spasms may be either brief or sustained and give rise either to narrowing or spasmodic closure of eyelids thus leading to functional blindness [1]. Dystonia of the lower face is frequently associated with BB [2]. Risk factors for cranial dystonia include being of female sex, having a family history of dystonia or postural tremor, eye disease, and surgical procedural on the mandibula [3,4]. Several neurological syndromes arise from neurovascular compression between cranial nerves (CN) and pulsatile blood vessels such as arteries. Chronical irritation induced by this intermitting pressure may give rise to trigeminal neuralgia (TN: compression of CN V), hemifacial spasm (HFS: CN VII), vestibulo-cochlear neuralgia (CN: VIII), and glossopharyngeal neuralgia (GN: CN IX) [5-7]. Although hemifacial spasm (HFS) appears to be a distinct disorder, a coexistence of both disorders has been described in up of the 5,5 % of affected patients [8]. Magnetic Resonance Imaging (MRI) of the brain revealed neurovascular compression of the the ipsilateral facial nerve in five out of the nine patients co-affected by either HFS and BB, without any detectable lesion within the basal ganglia [8].
A 58 years old man presented to our attention complaining painful sensation similar to electric shocks in the left side of his face, persistent ptosis and sporadic clonic movements of the OO as well as of the ipsilateral orbicularis oris. Phenomenology had started one year earlier. He also complained of superficial anesthesia in the region of the skin depending by the second branch of the ipsilateral Vth nerve. Neurological examination revealed sporadic clonic contractions of the left OO, rare spasms of a small portion of the left angle of the orbicularis oris and hypoesthesia to both painful and light tactile stimuli in the region innervated by the maxillary branch of the ipsilateral trigeminal nerve.
MRI as well angio-MRI of the brain was suggested in search of the eventual presence of neurovascular compressions or other abnormalities within the basal ganglia. One year later the patient presented to a follow-up visit. The required MRI clearly showed a sharp compression of the left Vth nerve by the superior cerebellar artery (Figure 1) as well as of the glossopharyngeal nerve (IXth) nerve with the postero-inferior cerebellar artery (PICA) (not shown). The patient himself and the clinical observation confirmed that symptomatology had progressed to a bilateral, although asymmetric blepharospasm with the left orbicularis oculi more affected (Video 1). The disturbance itself did not show any sign of inconsistency, bizarre phenomenology, unjustified relief or fluctuation. Several maneuvers were attempted to distract the patient but all failed.
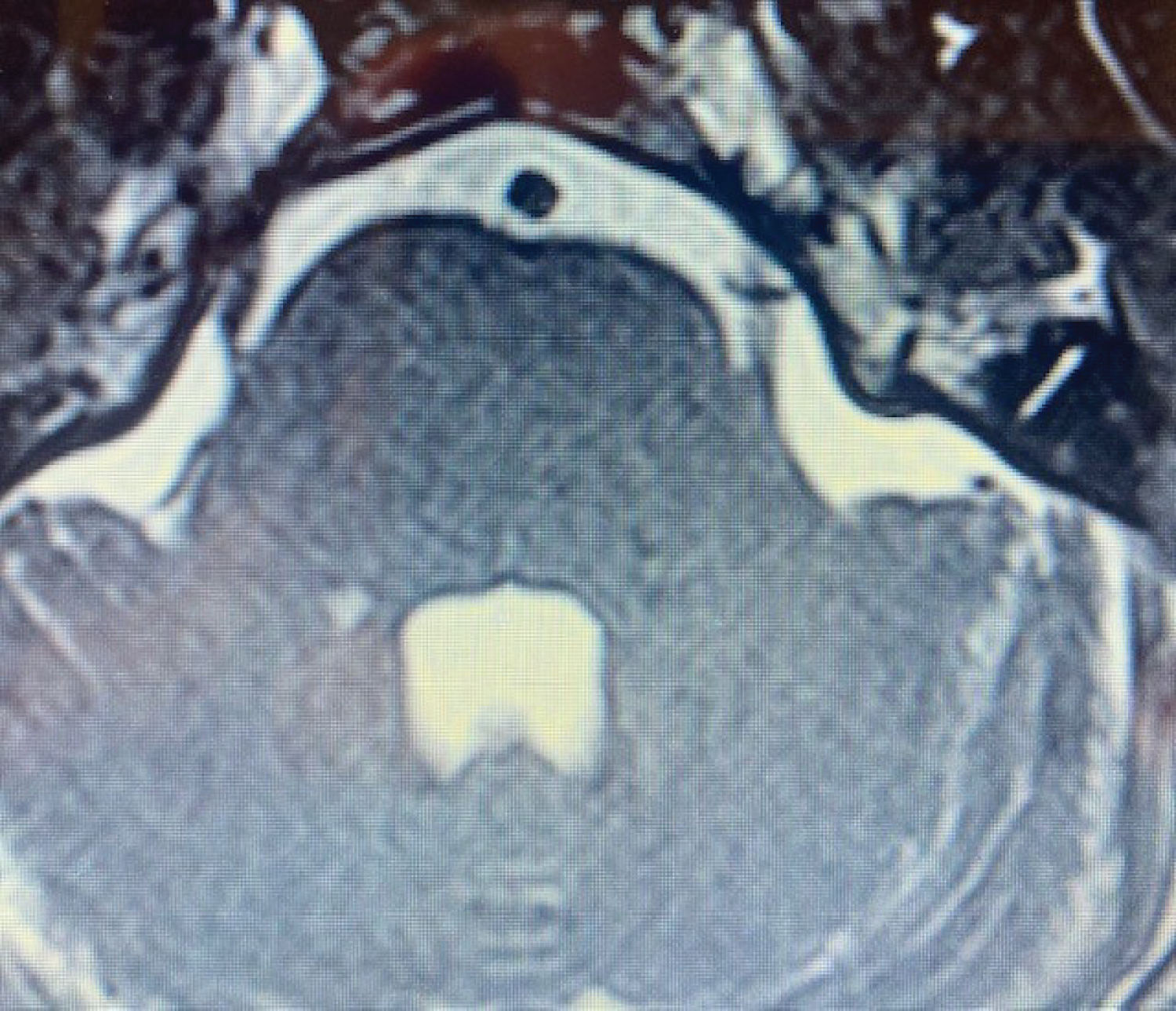 Figure 1: MRI imaging showing compression of the root of the left Vth nerve by left cerebella superior artery.
View Figure 1
Figure 1: MRI imaging showing compression of the root of the left Vth nerve by left cerebella superior artery.
View Figure 1
Video 1: Asymmetric blepharospasm with left sided more affected.
BB and HFS may share altered functional connectivity and sensory processing [9]. Relevance of this case report stands on absence of vascular compression of the facial nerve (VIIth cranial nerve) and the presence of compression of the trigeminal nerve. Although this finding might be only accidental and not pathogenic, one hypothesis may be launched based on the scientific background already known. Trigeminal and facial connections within the encephalic trunk manage the blink reflex and involve both afferent and efferent pathways [9]. Impairment of the inhibitory trigemino-facial responses in the perioral muscles suggest a central control of these reflexes [10]. These circuits are under the control of the cortex and of subcortical structures such as basal ganglia by the mean of descending pathways. Findings on our patient may suggest that peripheral mechanisms (the vascular compression of the trigeminal nerve by the superior cerebellar artery) may have triggered onset of spasms associated with neuralgia (tic convulsif) and, later on, may have induced spreading of these involuntary movements up to blepharospasm through dysfunctional circuits within the Central Nervous Systems.
None.
A written informed consent was obtained from the patient for publication of this case report. The patient is not recognizable.
None.
Maurizio Giorelli conceived the work and wrote the article, Sergio Altomare, Maria Stella Aniello, and Ruggiero Leone commented the case and suggested corrections.
All figures are the original one made by the authors for this article and have not been published previously.