Context: Rib fractures are mostly traumatic. Commonly seen in patients suffering from multiple injuries due to road traffic accidents or fall from height, conventional treatment is with intravenous/oral analgesics or opioid patches. The innervation of the ribs passes through the Serratus Anterior Plane and hence we aim to administer anaesthetic in this plane to achieve reliable and quality pain relief.
Methods and materials: 20 patients presenting with a rating of 8 on the visual analogue scale, whose pain was not relieved by intravenous analgesics and showed signs of rapid shallow breathing were administered SAPB unilaterally using ultrasound guidance.
Results: The patients pre-block median pain scores were 60 minutes Post block the median pain scores were. There were no complications due to the block the 24-hour post block period was uneventful.
Conclusions: Patients with multiple rib fractures (MRF) can be treated with SAPB with very good results and should be tried when patients are in severe pain not responding to intravenous anaesthetics and with deterioration of pulmonary function.
Regional anaesthesia, Rib fractures, Serratus anterior plane block, Ultrasound
Rib fractures are mostly traumatic. Commonly seen in patients suffering from multiple injuries due to road traffic accidents or fall from height, occasionally from cardiopulmonary resuscitation done on the ribs instead of the sternum.
Statistically up to 10% of patients presenting to the emergency department complain of Multiple rib fractures (MRF) often in conjunction with other trauma [1].
Thus far this condition was treated by multi-modal analgesia-intravenous/oral/opioid patches. MRF is a major cause of morbidity in patients will multiple injuries. It can lead to flail chest and splinting, which can compromise the respiration and lead to complications and deterioration of overall patient well-being. Opioids are not always advisable and sometimes detrimental in patients with pre-existing pulmonary disease. This leads to inadequate pain management [2].
The definitive treatment of MRF is a thoracic epidural for continuous infusion of analgesia, but this is not always easy or possible in all patients due to issues like coagulopathy, technical difficulties, need for monitoring and lack of cooperation due to need for positioning of patient due to the pain [3,4].
Ultrasound-guided Serratus Anterior Plane Block (SAPB) is a newer technique which is being used for managing post-thoracotomy, thoracoscopic surgery, or post mastectomy pain by anaesthesiologists [5,6].
SAPB is a single shot block that is relatively easier to administer, does not require elaborate patient positioning, can be learnt easily and done in the emergency department and emergency operation theatres [7,8].
Here we aim to use SAPB to provide localised pain relief that can last for up to 48 hours. If given in the acute phase of pain, it can improve pulmonary function and provide excellent pain relief that may not be possible with other methods.
20 patients with MRF of 2 or more, who had Visual analog scale (VAS) score of 7 or more persistently even after intravenous analgesia and gave their consent for the SAP block were taken into consideration for the study.
Many of the patients had multiple injuries, and so the VAS score was recorded during movement of the ribs i.e., coughing and deep breathing. The pain scores were recorded before the SAPB and 60 minutes after by post-graduate residents who were not directly involved in administering the block. The VAS scoring system was used as it is the most commonly used simple method of pain assessment which utilizes a simple numeric scale from 0-10, 0 being no pain and 10 being the worst possible pain. It also has color to aid in the description of pain as green is no pain and red is worst possible pain helping those who communicate through colors and visual perceptions of pain, it also has happy face to sad or crying face to help assist those with language barriers or children.
The patients were then shifted to a block room and monitors were connected, intravenous fluid on flow.
The patient was positioned supine with the arm abducted or in lateral position if abduction was not possible.
Drugs used- 1 ml/kg body weight of 0.25% Bupivacaine with 8 mg (2 ml) dexamethasone; In case of B/L fracture, volume not more than 40 ml of 0.25% Bupivacaine.
Equipment: Ultrasound machine with a high frequency 7-12 hz transducer.
All blocks were done in a room where emergency equipments and drugs were available.
After positioning, the block area was sterilised, and the probe was made sterile using transducer cover and sterile lubricant gel was used.
The authors trained in procedural ultrasound administered the blocks.
The transducer was placed in the mid-axillary line on the 5 th rib. (By counting the ribs) in the sagittal plane using the technique suggested by Hadzik, et al. In this view, the latissimus dorsi (LDM) and the serratus anterior muscles (SAM) were identified as shown below [9,10].
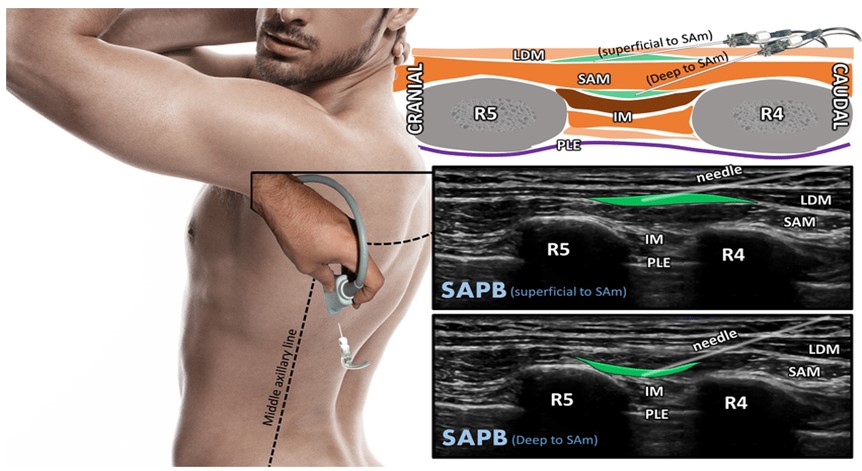
When there was a doubt about the plane, it was identified using the thoracodorsal artery using color doppler.
The point of entry was anaesthetised using local anaesthetic 2% lignocaine to raise a wheal.
Using a 20 gauge cannula, the SA plane was entered using in-plane technique (cranial to caudal) with a high frequency transducer.
After hydro-dissection, the drug was slowly injected after regular aspiration (to rule out vascular puncture) into the SA plane with the vitals being closely monitored.
Below is an image of the drug after injection lifting off the serratus muscle and the latissimus dorsi as shown in the above picture (superficial to SAM).
The VAS was again recorded 60 minutes post block. Dynamic (Cough or deep breath) VAS less than or equal to 4 was taken as a successful block. Failure to relieve pain to at least 50% of pre-block pain within 60 minutes was taken as block failure. Breakthrough pain or block failure was treated with IV Opioids.
Patients were kept in the observation room for 60 minutes post block to look for any signs of CVS/CNS signs of local anaesthetic systemic toxicity. The saturation and ET - CO 2 (end-tidal CO 2 levels) were recorded via pulse-oximetry and capnometry.
There were no patients who had any side effects.
The Patients were followed up for a period of 24 hours and the duration of block was recorded.
There were no patients whose condition deteriorated post block. Some patients who had hemopneumothorax were followed up for worsening. Over all the procedures were uneventful.
|
Descriptives |
Pain score during movement before block |
Pain score during movement after 60 min of SAP block |
|
N |
20 |
20 |
|
Median |
9.00 |
2.00 |
|
IQR |
1.25 |
1.25 |
|
Minimum |
7 |
1 |
|
Maximum |
10 |
4 |
The Pain scores were significantly lower after 60 minutes of the SAP block, The median pain score before the block was 9 on the VAS scoring and 2 on the VAS score 60 minutes after the SAP block. These were dynamic pain scores i.e., pain on coughing or deep breath. The interquartile range is 1.25 for which means that the reduction in the pain score can possibly be predicted, in other words we can expect a reduction of up to 60% of the pain after SAP block.
Frequencies of Pain score during movement before block
|
Pain score during movement before block |
Counts |
% of Total |
Cumulative % |
|
7 |
3 |
15.0% |
15.0% |
|
8 |
6 |
30.0% |
45.0% |
|
9 |
6 |
30.0% |
75.0% |
|
10 |
5 |
25.0% |
100.0% |
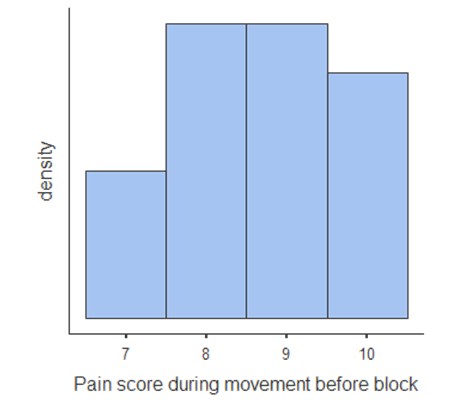
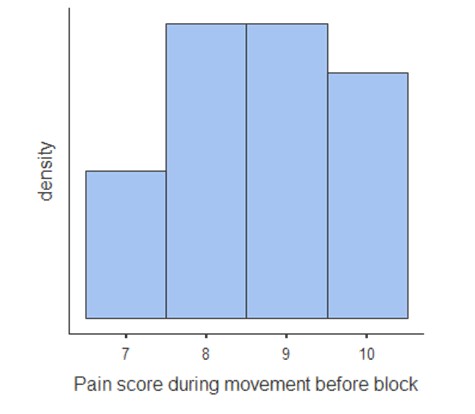
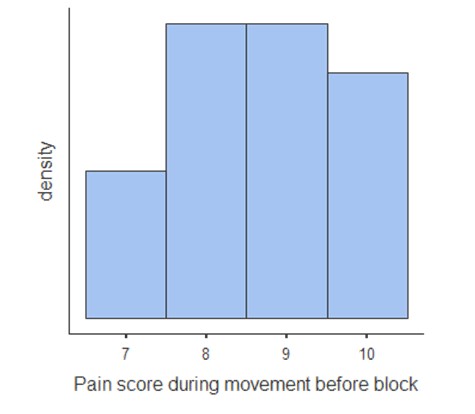
The above table shows that the majority of the patients had extreme pain with 85 percent of the patients reporting a pain scale above 8. Hence there is a need to address pain from multiple rib fractures seriously.
Frequencies of Pain score during movement after 60 min of SAP block
|
Pain score during movement after 60 min of SAP block |
Counts |
% of Total |
Cumulative % |
|
1 |
5 |
25.0% |
25.0% |
|
2 |
9 |
45.0% |
70.0% |
|
3 |
4 |
20.0% |
90.0% |
|
4 |
2 |
10.0% |
100.0% |
The above table represents the number of patients who have reported a VAS score of 1, 2, 3, and 4. 9 patients have reported a VAS score of 2 which means mild pain only and 5 patients have reported a VAS of! which is very little pain.
4 patients have reported a VAS score of 3 which means mild to moderate pain and 2 patients have reported a pain score of 4 which is moderate pain.
From this it can be concluded that there is a high patient satisfaction with 70% of patients reporting very little to mild pain and 30% reporting moderate pain.
On the whole all patients have at least 50% reduction in their pain scores.
Pain score during movement after 60 min of SAP block
The above plots show that the patients with the higher VAS scores achieved higher pain relief as compared to the ones with lower pain scores. This is in accordance with the subjective quality of pain wherein the patient focuses more on the areas that hurt more and hence report higher relief/satisfaction when that area of pain is relieved.
|
|
|
|
Statistic |
p-value |
Mean difference |
SE difference |
|
Pain score during movement before block |
Pain score during movement after 60 min of SAP block |
Wilcoxon W |
210 |
< 0.01 |
6.50 |
0.246 |
Note. Hₐ μ Measure 1 - Measure 2 ≠ 0
There is a significant difference in pain score during movement after SAP Block, the median pain score was 9 before the block, reduced to 2 after SAP block (P value < 0.001) [11,12].
Pain score during movement before block - Pain score during movement after 60 min of SAP block:
The above plot shows the mean and median on a graph, there is a significant drop in the VAS scores post SAP block.
|
Descriptives |
Duration of block in hours |
|
N |
20 |
|
Missing |
0 |
|
Mean |
15.3 |
|
Median |
14.5 |
|
Standard deviation |
3.07 |
|
Minimum |
11 |
|
Maximum |
20 |
The above table shows us the duration of block in each patient. The maximum being 20 hours and the minimum being 11 hours.
The mean and median were similar around 15 hours. The standard deviation is around 3 hours.
This shows that the SAP block can provide up to 15 hours of pain relief in patients with multiple rib fractures (Table 1).
Table 1. View Table 1
The above is the complete table with demographics and other co-injuries sustained. 15 patients were male and 5 patients were females. 8 patients had other injuries, among them 3 patients had chest wall, pleura, or lung injuries.
7 patients have pre-existing lung issues. 2 had COPD, 2 had Bronchial asthma and 1 had emphysema and 2 had reactive airways.
Traditionally, MRF has been managed using multi-modal analgesia, including opioids, which may not always be advisable due to potential complications, particularly in patients with pre-existing pulmonary diseases. Thoracic epidural, while effective, may not always be feasible. SAPB emerges as a promising alternative, offering localized pain relief that can last up to 48 hours.
This study involved 20 patients with MRF who had persistent severe pain despite intravenous analgesia. The SAPB technique was administered, and pain scores were recorded before and after the block. Results showed a significant reduction in pain scores after 60 minutes of the SAPB, with a median pain score dropping from 9 to 2 on the Visual Analog Scale (VAS). The majority of patients reported either mild or no pain after the block, indicating high patient satisfaction. There were no reported adverse effects of the block, and patients were followed up for 24 hours post-procedure without any deterioration in their condition. There were 7 patients in whom pre-existing lung disease was present and they reported no difficulty in breathing and their saturation remained above 95 percent with no carbon dioxide retention as recorded with capnometry.
Furthermore, the study highlighted the duration of pain relief provided by SAPB, with the mean duration being around 15 hours. This demonstrates the potential for SAPB to offer prolonged pain relief in patients with MRF.
The findings suggest that SAPB can be a valuable tool in managing pain associated with MRF, offering effective pain relief with minimal risk and relatively easy administration. However, the study sample size is small, and further research with larger cohorts is warranted to validate these findings. Additionally, long-term outcomes and comparisons with other analgesic techniques would provide a more comprehensive understanding of SAPB's role in MRF management.
In conclusion, SAPB presents as a promising alternative for pain management in patients with MRF, offering effective and localized pain relief with minimal risk and potential for prolonged duration. Its simplicity of administration and favorable outcomes make it a valuable addition to the armamentarium of pain management strategies for MRF.
The study evaluates Ultrasound-guided Serratus Anterior Plane Block (SAPB) for managing pain in multiple rib fracture (MRF) patients. With 20 participants, SAPB significantly reduces pain scores post-procedure, with a median drop from 9 to 2 on the Visual Analog Scale (VAS). Most patients report mild or no pain after SAPB, suggesting high satisfaction. No adverse effects are observed, and SAPB provides around 15 hours of pain relief. This highlights SAPB's potential as an effective, safe, and easily administered method for MRF pain management, warranting further investigation and potential integration into clinical practice.
Serratus anterior plane block shows promise as a safe, effective, and feasible method for managing pain in multiple rib fracture patients.
Not funded.
Dr Aaron Dsouza has given his expert advice and helped in reviewing the data, in research and article writing. Dr Divya Vincent was the primary pain physician administering the blocks and collecting the data.