There are contradictory results on the efficacy and safety of the use of neuromuscular blockers.
To address the efficacy and safety of neuromuscular blocking agents (NMBAs) in adults with acute respiratory distress syndrome (ARDS).
We searched CENTRAL, MEDLINE, EMBASE, LILACS, WHO International Clinical Trials Registry Platform (ICTRP), and reference lists of retrieved studies from database inception to June 8, 2019.
Randomized controlled trials (RCTs) comparing the administration of early NMBAs versus placebo or no treatment in patients with ARDS.
Two review authors independently screened the abstracts and titles for relevance. Screening for inclusion, data extraction, and risk of bias assessment were performed by one author and checked by the second. We assessed trials for the overall quality of evidence using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) instrument. We calculated the risk ratios (RR) and 95% confidence intervals (95% CI) for dichotomous outcomes, while for continuous results we obtained the mean difference and performed a random-effects meta-analysis.
Six RCTs including 3351 patients proved eligible. All of the six trials included in this review were parallel comparisons with individual randomization. The included studies were generally judged as having either a 'low' risk of bias, 'unclear' risk of bias, or 'high' risk of bias. Early NMBAs were associated with a significant reduction of all-cause mortality (RR 0.84, 95% CI 0.74 to 0.95; moderate quality of evidence). There were less barotrauma events in the NMBAs group (RR 0.55, 95% CI 0.35 to 0.85; low-quality of evidence). There were no significant differences in other outcomes, such as health-related quality of life, ventilator free days, and hospital free days.
In adult patients with ARDS, NMBAs may result in a reduction of all-cause mortality with a non-significant increment in adverse events.
Neuromuscular blocking agents, Acute respiratory distress syndrome, Meta-analysis, Systematic review
Acute respiratory distress syndrome (ARDS) is a life-threatening disease characterized by an inflammatory lung lesion clinically manifested by hypoxia and decreased pulmonary compliance [1]. Currently, the mortality of moderate to severe ARDS remains more than 40% [2,3]. ARDS can develop in the context of pneumonia (35%-50% of cases), sepsis of non-pulmonary origin (30%), aspiration of gastric content (10%), and trauma (10%) [4]. Several other less-common scenarios are also associated with the development of ARDS, including acute pancreatitis or transfusions [5]. Recently, the use of e-cigarettes has also been described as a cause of respiratory distress, especially in young people [6,7].
The therapeutic approach to ARDS is based on a multimodal strategy that combines non-pharmacological strategies (protective ventilation, conservative fluid management, and prone position), as well as pharmacological interventions against the underlying cause [8,9]. Scarce pharmacological interventions have been reported in literature for the treatment of ARDS, regardless of its cause. NMBAs have been prescribed to patients with ARDS as they are thought to facilitate lung-protective ventilation, decrease inflammation, reduce oxygen consumption, improve oxygenation, and help facilitate ventilator synchrony [10]. NMBAs have been evaluated in patients with ARDS in several RCTs and have resulted in improved oxygenation, ventilator-free days, and mortality [11-15].
Currently NMBAs are the standard of care. Both recently published French and British clinical practice guidelines for the management of ARDS, suggest the use of a continuous 48 hour infusion for patients with moderate to severe ARDS [16,17]. NMBAs are frequently used in the Intensive Care Unit (ICU). In a survey of academic intensivist's use of neuromuscular blockade, 96.6% of respondents advised they would use NMBAs in patients with moderate to severe ARDS [18].
In the present meta-analysis, data from a new RCT conducted in the US was incorporated [19]. Furthermore, a recent network meta-analysis suggested that NMBAs did not affect mortality [20].
Given the discordant evidence, it is necessary to try to clarify the role of NMBAs in the treatment of ARDS.
We followed the steps outlined by the Cochrane Collaboration [21] and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines [22]. We included RCTs comparing the administration of NMBAs in patients with ARDS versus no treatment according to the accepted criteria [23,24]. Quasi-randomized studies and cross-design studies were not eligible to be included in this review.
We performed a comprehensive search of MEDLINE, EMBASE, CENTRAL, LILACS, and the International Clinical Trials Registry Platform (ICTRP) for RCTs from database inception to June 8, 2019. Keyword search terms included "acute respiratory distress syndrome", "adult respiratory distress syndrome", "shock lung", "non-cardiogenic pulmonary edema", or "ARDS" AND "neuromuscular blocking agents" or "neuromuscular blockade" in a search that did not apply any language restrictions. We planned to identify other potentially eligible trials or ancillary publications by searching the reference lists of the retrieved and included trials, systematic reviews, meta-analyses, and health technology assessment reports. In addition, we contacted the authors of the included trials to identify any further studies that we may have missed. No summaries or congress summaries were used for the data extraction, because this source of information did not meet the requirements of the Consolidated Study Reporting Standards (CONSORT) [25].
We performed all of the screening in duplicate (A.A. and C.R.), with disagreements being resolved by discussion and third-party adjudication as required (G.C.). After implementation of the search strategy, the reviewers worked in pairs to screen all of the potentially relevant citations and references. Reviewers performed the screening in two stages, initially assessing titles and abstracts and then full articles for those possibly eligible. We present an adapted PRISMA flow diagram to show the process of trial selection (Figure 1). We captured the reasons for exclusion at the full article review stage.
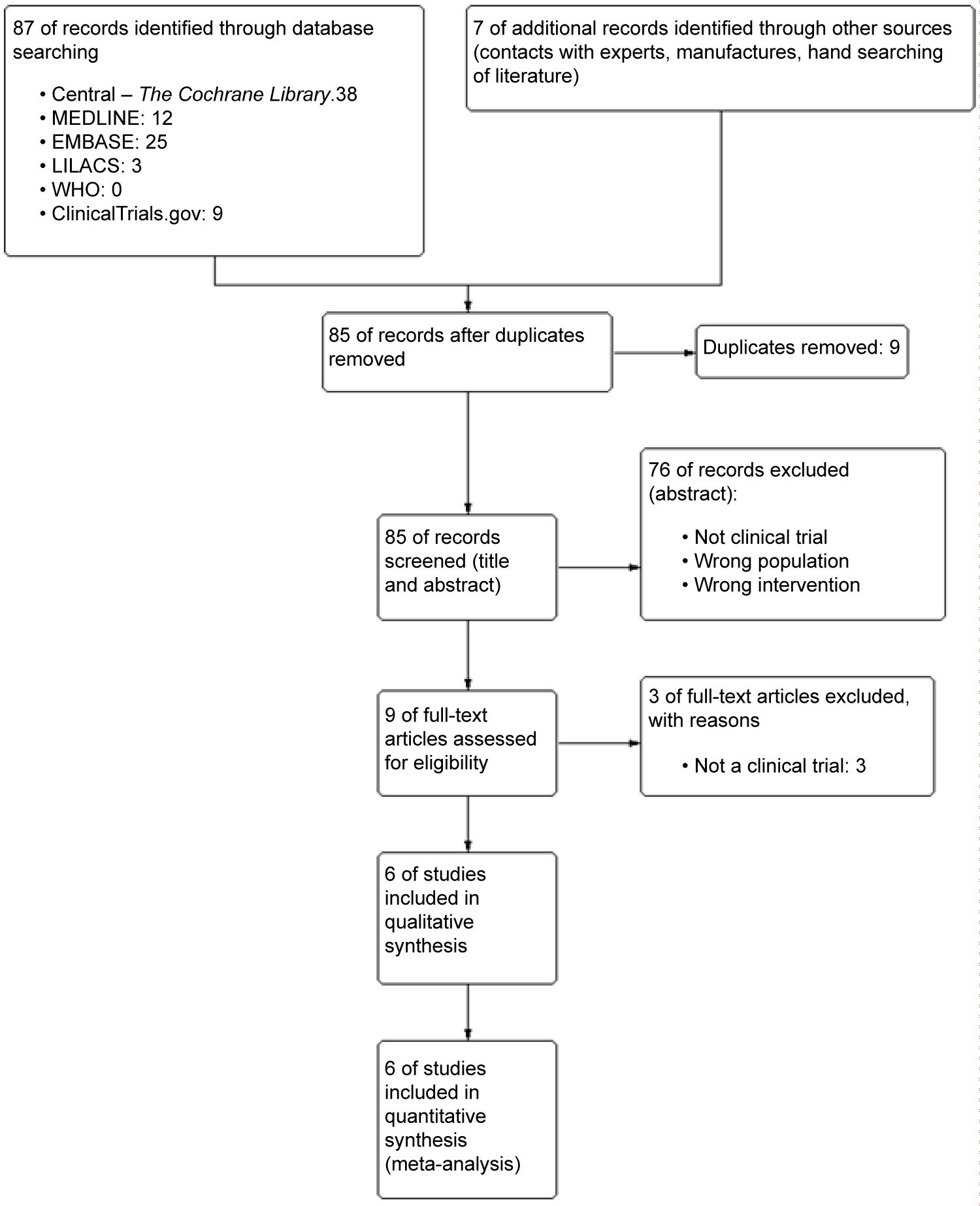 Figure 1: PRISMA Flow Diagram.
View Figure 1
Figure 1: PRISMA Flow Diagram.
View Figure 1
Our primary outcomes were all cause mortality. Our prespecified secondary outcomes were health-related quality of life, adverse events, organ failure improvement, improvement of PaO2/FiO2, days free of ventilation, days not in ICU, and days not in hospital.
Reviewers performed the data extraction independently and in duplicate using predefined data abstraction forms. A third reviewer resolved disagreements. Abstracted data included the study title, first author, demographic data, details of the intervention and control, primary and secondary outcome data, and risk of bias (RoB) for each study.
RoB was assessed, independently and in duplicate, for each outcome of individual studies using a modified Cochrane RoB2 tool [26] that classifies RoB as "low", "probably low", "probably high", or "high" for each of the following domains: Sequence generation, allocation sequence concealment, blinding, selective outcome reporting, and other bias. We rated the overall RoB as the highest risk attributed to any criterion. We also assessed publication bias for every outcome. We assessed the overall certainty of evidence for each outcome using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework [27]. Disagreements for RoB and GRADE assessments were resolved by discussion. We present a 'Risk of bias' graph and a 'Risk of bias' summary figure (Figure 2).
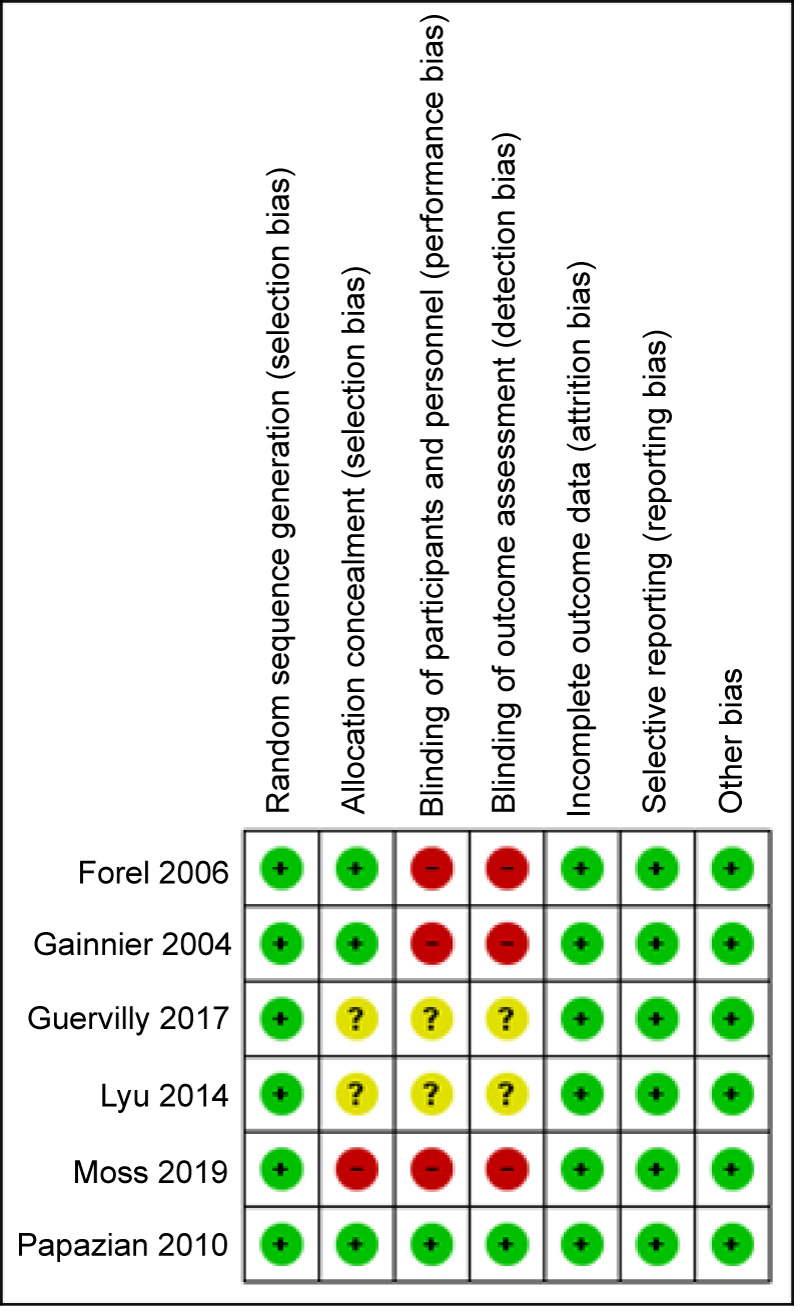 Figure 2: Risk of bias graph; reviewing author’s judgments about each risk of bias item presented as percentages across all included studies.
View Figure 2
Figure 2: Risk of bias graph; reviewing author’s judgments about each risk of bias item presented as percentages across all included studies.
View Figure 2
A fixed-effects meta-analysis was used to combine the data when it was reasonable to assume that the studies were estimating the same underlying effect of treatment. If there was sufficient clinical heterogeneity to expect that the effects of the underlying treatment would differ between studies or if substantial statistical heterogeneity was detected, a random effects meta-analysis was used. We presented results as RRs for dichotomous outcomes and as mean difference (MD) for continuous outcomes, both with 95% CIs. We assessed for heterogeneity between the studies using the chi-square test for homogeneity, the I2 statistic, and visual inspection of forest plots. We considered the magnitude and direction of heterogeneity when considering whether to rate down our certainty in the evidence for inconsistency.
The protocol was not registered previously.
Table 1 shows the demographic characteristics of the studies included in the systematic review. Eighty-seven studies were identified as potentially eligible for inclusion in this review. A total of 1565 patients with ARDS participated in the six finally included studies comparing neuromuscular blockade with placebo or no treatment.
Table 1: Demographic table. View Table 1
A total of 698 participants were randomly assigned to receive neuromuscular blockade. One study used vecuronium [14], while the rest used cisatracurium. The comparison group included 885 participants: 162 in the placebo group and 723 in the no treatment group. Only one study used placebo as a comparator [16].
Regarding geographical location, one investigation was carried out in a center in China [14], four studies were carried out in multiple centers in France [11,12,15,16], and one study was carried out in 13 centers in the US [19].
All studies were conducted from 2004 to 2018. The duration of intervention varied from 48 hours [11-13,15,27] to 72 hours [14]. The duration of follow-up varied from until discharge from the ICU [11,12,15] up to 12 months [27]. Only the ROSE trial was stopped for futility.
The average age of the participants varied from 56 years [27] to 66 years [15]. Baseline demographic characteristics were similar between the treatment groups in most of the studies. The Simplified Acute Physiology Score (SAPS) II average varied from 44 points [11] to 49 points [13]. The Sequential Organ Failure Assessment (SOFA) score ranged from 9.5 points [15] to 15.4 points [14]. Direct lung injury was the main mechanism of ARDS in all of the studies and the main cause of direct lung injury was pneumonia in most of the studies (including aspiration pneumonia, community acquired pneumonia, nosocomial pneumonia, and/or ventilator associated pneumonia). Only one study did not report on the main cause of the direct lung injury [16].
The diagnostic criteria for ARDS differed between the studies. Three studies used the American-European Consensus definition [11,12,16] and three studies used the 2012 Berlin definition [14,15,19].
Table 2 shows a summary of findings for primary and secondary outcomes based on meta-analysis of the identified trials and includes the certainty of the evidence and the reasons for rating down certainty.
Table 2: Summary of findings table including relative effect measure, absolute effect measure, and certainty of evidence. View Table 2
Figure 3 shows a forest plot of the comparison between NMBAs and placebo or no treatment for the different mortality subgroups.
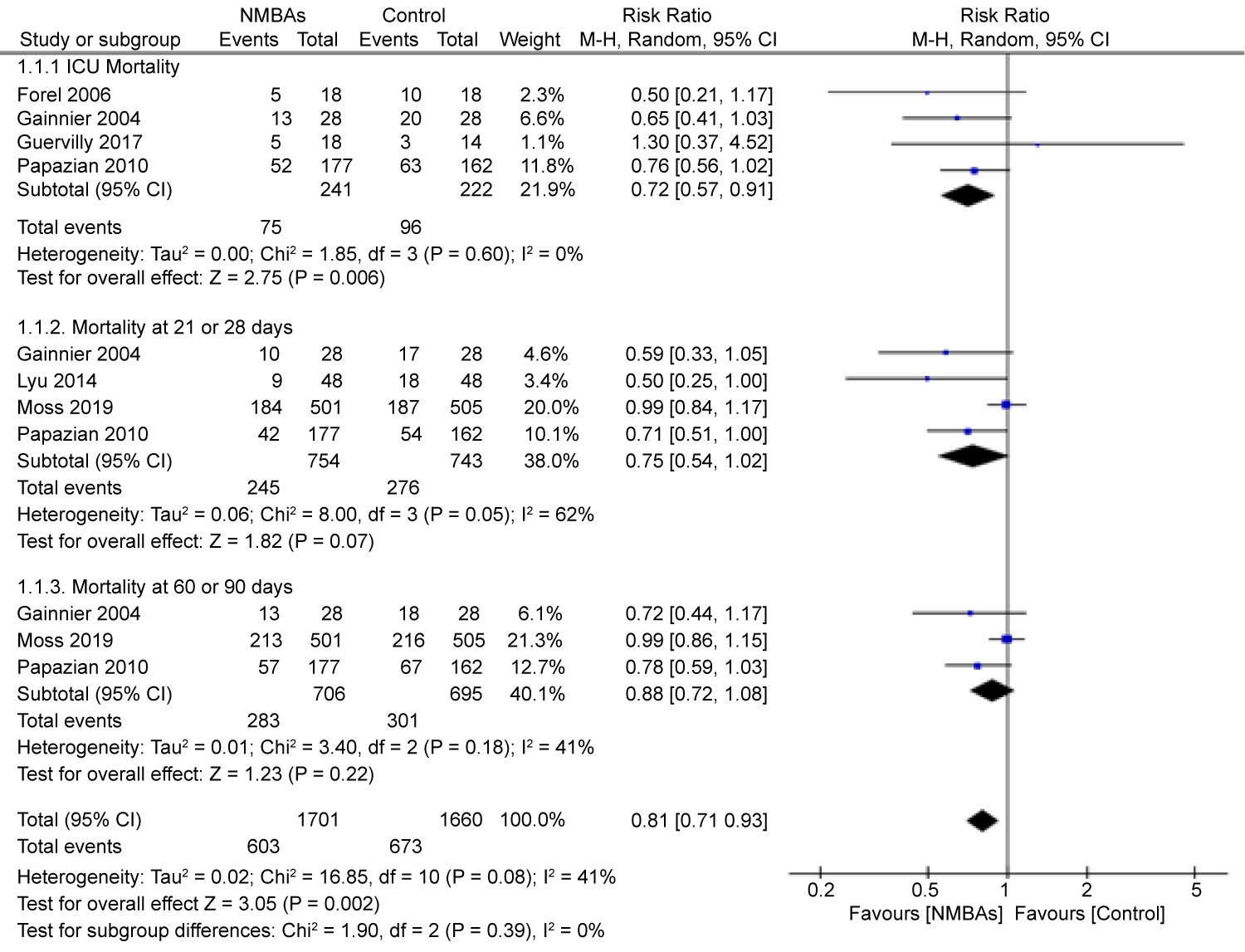 Figure 3: Forest plot of comparison: Neuromuscular blocking agents versus placebo or no treatment (parallel randomized controlled trials [RCTs]), outcome: Mortality.
View Figure 3
Figure 3: Forest plot of comparison: Neuromuscular blocking agents versus placebo or no treatment (parallel randomized controlled trials [RCTs]), outcome: Mortality.
View Figure 3
Figure 4 shows a forest plot of the comparison between NMBAs and placebo or no treatment for the different adverse events subgroups.
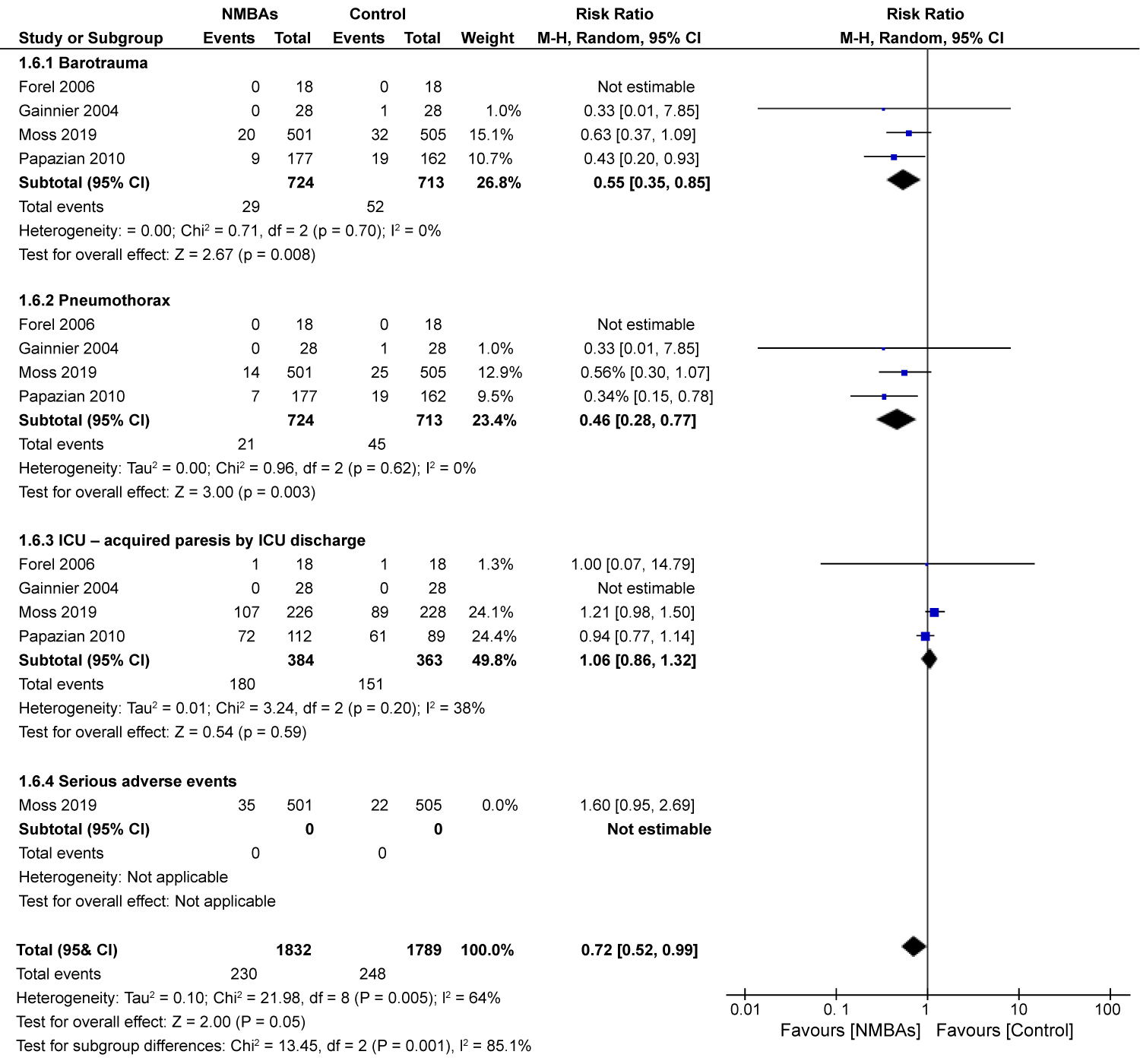 Figure 4: Forest plot of comparison: Neuromuscular blocking agents versus placebo or no treatment (parallel RCTs), outcome: Adverse events.
View Figure 4
Figure 4: Forest plot of comparison: Neuromuscular blocking agents versus placebo or no treatment (parallel RCTs), outcome: Adverse events.
View Figure 4
Only one trial reported health-related quality of life with a validated tool. There was no difference in the difficulty of a daily activity (MD 1.04 points, 95% CI 0.91 to 1.20, one RCT, 247patients, low certainty of evidence). There was no difference in the disability score (MD 0 points, -0.27 to 0.27, one RCT, 207 patients, low certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a significant increment in organ failure free days up to day 28 by system (MD 0.83 days, 95% CI 0.10 to 1.56, RCTs, 5315 patients, moderate certainty of evidence). There was no difference between the groups in the number of days without coagulation abnormalities (MD 0.84 days, 95% CI -1.04 to 3.09, two RCTs, 1344 patients, very low certainty of evidence). There was no difference between the groups in the number of days without cardiovascular failure (MD 0.76 days, 95% CI -0.66 to 2.18, two RCTs, 1344 patients, low certainty of evidence). There was no difference between the groups in the number of days without hepatic failure (MD 1.17 days, 95% CI -0.46 to 2.8, two RCTs, 1287 patients, very low certainty of evidence). There was also no difference between the groups in the number of days without renal failure (MD 0.98 days, 95% CI -1.45 to 3.41, two RCTs, 1342 patients, very low certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a non-significant improvement in PaO2/FiO2 levels at 24 hours (MD 5.68 mmHg, 95% CI -3.56 to 14.91, three RCTs, 1235 patients, very low certainty of evidence). There was a non-significant improvement in the neuromuscular blockade group in PaO2/FiO2 levels at 48 hours as compared with placebo (MD 21.18 mmHg, 95% CI -0.17 to 42.53, p = 0.05, three RCTs, 833 patients, very low certainty of evidence). There was a significant improvement in the neuromuscular blockade group in the PaO2/FiO2 levels at 72 hours when compared with placebo (11.27 mmHg, 95% CI 2.12 to 20.43, three RCTs, 977 patients, low certainty of evidence). There was a significant improvement in the neuromuscular blockade group in the PaO2/FiO2 levels at 7 days compared with placebo (12.97 mmHg, 95% CI 0.26 to 25.68, two RCTs 596patients, moderate certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a non-significant reduction in plateau pressure (-0.30 cmH2O, 95% CI -0.77 to 2.27, five RCTs, 3219 patients, low certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a significant reduction in positive-end expiratory pressure (PEEP; -0.40 cmH2O, 95% CI -0.65 to -0.15, four RCTs, 4111 patients, moderate certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a significant reduction in FiO2 (-0.03%, 95% CI -0.04 to -0.02, four RCTs, 3701 patients, moderate certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a non-significant reduction in peak inspiratory pressure (-0.47 cmH2O, 95% CI -1.02 to 0.07, three RCTs, 2907 patients, low certainty of evidence).
Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a non-significant increment of ventilator free days at 28 days (0.67 days, 95% CI -0.50 to 1.85, five RCTs, 1461 patients, low certainty of evidence).
There was a significant increment of days not in the ICU at 90 days in patients from the neuromuscular blockade group as compared with the placebo or no treatment groups (8.20 days, 95% CI 0.82, 15.58, one RCT, 339 patients, moderate certainty of evidence). Compared to the placebo or no treatment groups, neuromuscular blockade was associated with a non-significant increment of days not in the hospital at 28 days (0.20 days, 95% CI 0.78 to 1.18, one RCT, 1006 patients, low certainty of evidence).
We included six published parallel trials in this review. There were a total of 1565 participants with ARDS who were followed-up for 2 weeks to 1 year. However, the diagnostic criteria were different between the trials; three used the Berlin definition and the other three used the American-European Consensus Conference criteria for ARDS.
We identified a variety of different interventions in the included trials of the review which we grouped into tree main comparisons: Four trials compared cisatracurium with no treatment; one trial compared vecuronium with no treatment; and one trial compared cisatracurium with placebo.
All of the included trials explicitly stated at least one primary endpoint in their publication. The most common primary outcomes were proportion of patients who died before hospital discharge and within 90 days after study enrolment, and improvements in oxygenation. Four trials investigated ICU mortality. Four trials reported mortality at 21 to 28 days. Three trials investigated mortality at 60 to 90 days. Four trials reported adverse events. One trial investigated health-related quality of life. Two trials investigated organ failure free days. Five trials reported respiratory parameters. Five trials reported days free of ventilation at 28 days. Three trials reported days not in the ICU. One trial reported days not in the hospital at 28 days. No trials investigated socioeconomic effects.
Overall, the results of this systematic review suggest that the use of NMBAs compared with placebo causes a statistically significant reduction in all-cause mortality. Regarding the safety of the NMBAs, we found a non-significant increase in the risk of developing at least one adverse event when compared with placebo. Unfortunately, based on the limited trial data included in this review, we were not able to analyze the health-related quality of life and socioeconomic effects of participants who received neuromuscular blockade, as compared with placebo.
In many trials the risk of bias was unclear, because their reports did not mention in detail the methods of allocation concealment, blinding of participants and personnel, and blinding of outcome assessment. One-third of the trials had a high risk of bias due to performance bias and detection bias. One trial had a high risk of bias due to selection bias. We used GRADE to assess the overall quality of evidence.
The quality of evidence for mortality was moderate when NMBAs were compared with placebo or no treatment due to serious inconsistency.
The quality of evidence for adverse events was low due to very serious imprecision (low median sample size and small number of trials and CIs for the pooled estimate consistent with benefit and harm) and inconsistency.
This review was performed using the standard Cochrane methodology without any restrictions regarding language or date of publication. All included trials were selected and assessed, and data were extracted by three reviewing authors to minimize biases in the process of the review. When we identified substantial heterogeneity, we tried to reduce it by data stratification. When data were missing, we attempted to contact the authors of the study.
This review suggests that early neuromuscular blockade causes a reduction in all-cause mortality. Similarly, we found a decrease in the incidence of barotrauma and pneumothorax, without an increase in weakness acquired in the ICU. However, all of the findings should be interpreted cautiously due to the moderate or very low-quality evidence and substantial heterogeneity between trials.
Further research is required to determine whether the use of NMBAs has any effect on morbidity, socioeconomic effects, and health-related quality of life in patients with moderate to severe ARDS, as well as whether this intervention might be useful in combination with other therapeutic interventions to reduce mortality.
Financial support for this study was provided by the American British Cowdray Medical Center, I.A.P.