Asthma is one of the leading causes of respiratory failure. It is important to predict which patients might suffer from respiratory failure. The aim of this study is to investigate the possibility of using pulse oximetry as alternative to arterial blood gas analysis for measuring oxygen saturation (SaO2) to predict hypoxic respiratory failure.
A prospective study was conducted in the Emergency Department (ED) of Baghdad Teaching Hospital over one year. A convenient sample of 100 consecutive adult patients over the age of 14 years, who presented with dyspnea and known past history of asthma, were recruited over the study period. They all underwent history, clinical examination & investigations with arterial blood gas tensions and pulse oximetry tests. Respiratory failure was defined as PaO2 < 60 mmHg and/or PaCO2 > 50 mmHg.
Eighty-eight patients had oxygen saturation of 92% or higher of which only one (1.13%) had respiratory failure. There were 7 patients with O2 saturation levels between 90% and 92%, out of which 2 (28%) had respiratory failure. In the third group, out of 5 patients with O2 saturation less than 90%, 3 (60%) were found to have respiratory failure.
In severely ill patient, we can depend on pulse oximetry to predict hypoxic respiratory failure in patients with known medical history of asthma if initial value of O2 saturation is > 92%.
(MeSH) respiratory insufficiency, Asthma, Oximetry, Blood gas analysis
Asthma is one of the leading causes of respiratory failure: A syndrome where the respiratory system is unable to perform its gas exchange functions. These include oxygen consumption and carbon dioxide elimination. The two types of respiratory failure are medically categorized as hypoxemic or hypercapnic [1]. If the arterial oxygen tension (PaO2) is less than 60 mmHg and the carbon dioxide tension (PaCO2) is normal or low, the failure is classified as hypoxemic (type I). On the other hand, if the PaCO2 levels are higher than 50 mmHg, the failure is classified as hypercapnic (type II) [2].
Pulse oximetry-the "fifth vital sign"-is a useful method in assessing asthma. It permits the checking of SpO2 levels on a nonstop premise [3]. A sensor is positioned on a thin part of the patient's body, usually a fingertip or earlobe. If the patient is an infant, the sensor is placed across a foot. Furthermore, a pulse oximeter is a medical contraption that indirectly monitors both oxygen saturation levels of a patient's blood (rather than directly measuring oxygen saturation via a blood test), and the fluctuations in the blood volume of the skin, producing a photoplethysmogram [4].
An arterial blood gas test (ABG) analyzes a sample of blood from an artery. This arterial blood is extracted using a thin needle and syringe to obtain a small blood sample. In most cases, the radial artery in the wrist is an ideal puncture site; however, the femoral artery, in the groin, and other areas are used sometimes. Moreover, blood can also be withdrawn from an arterial catheter. The ABG test determines the arterial oxygen tension (PaO2), carbon dioxide tension (PaCO2), acidity (pH) and arterial oxyhemoglobin saturation (SaO2). This information is crucial when attending to patients suffering from severe diseases of all kinds, including respiratory illnesses. Consequently, the ABG is a common assessment conducted on patients in intensive care units (ICUs) [5].
Therefore, the purpose of this study is to assess the necessity of arterial blood gas estimation in all patients exhibiting acute severe asthma and the reliability of using pulse oximetry as an alternative method of measuring oxygen saturation (SaO2) to predict patients in hypoxic respiratory failure. The study also aimed to specify an SaO2 value under which arterial gases should be administered to safely manage severe asthma.
A prospective study was conducted in the Emergency Department of Baghdad Teaching Hospital over the span of one year. (1st of April 2015) to (31st of March 2016).
A sample of 100 consecutive adult patients was included. They all underwent history, clinical examination & investigations with Arterial blood gas tensions and pulse oximetry tests.
1- Age of 14 years or above.
2- Presented with dyspnea and known past history of asthma.
1- Patients with chronic obstructive airway diseases.
2- Patients with heart failure.
3- Patients who smoked recently (less than 4 hours).
For each patient, the following variables were assessed: Age, sex, chief complaint, clinical details of history & examination including the duration of the complaint and associated symptoms like coughs, chest pain and fever. Further on this, medication used to treat asthma, using steroid on a chronic basis or not, previous admission to the ICU or hospital from asthma, frequency of visiting the ER because of exacerbation, frequency of treatment needed per day and cardiac rhythm abnormality were also examined.
At presentation to the Emergency department, the patient usually complained of shortness of breath, even at rest, that prevent his compliance & cooperation with the physician. Therefore, after excluding other life threatening conditions by assessing airway, breathing, circulation, electrocardiogram and blood tests, oxygen was given to the patient through a face mask (10 liters). Then, the patient was given a thorough explanation on what an ABG is. Oxygen saturation was measured using Rossmax pulse oximeter SB 220.
Next, verbal consent was obtained and an Allen test (a standard test used to assess the arterial blood supply of the hand) was then done. An arterial sample was taken from all eligible patient using a plastic 3 ml syringe which had been primed with (1 ml) of heparin solution.
Samples were then run on the gas analyzer machine located in the Intensive Care Unit of Baghdad Teaching Hospital (ABL 800 flex).
The study excludes any patients below the age of 14. In addition to that, not all patients presented with dyspnea and history of asthma accepts to do the ABG test. Moreover, although most of asthma exacerbation happened at night, the study includes only patients presented at morning duties due to unavailable ABG facilities at night.
All patients ‘data entered using computerized statistical software; Statistical Package for Social Science (SPSS) version 21 used. Kolmogorov smirnov analysis verified the normality of data set. Multiple contingency tables conducted and appropriate statistical test performed. In all statistical analysis, level of significance (p value) set at < 0.05 and the result presented as tables and/or graphs.
The total number of all asthmatic patients enrolled in this study was 100. There were 46 (46%) males & 54 (54%) females. The demographic details of patients are shown in Table 1. Each patient had pulse oximetry and ABG measurement. Pulse oximetry readings range from 86% to 98%. 88 patient had SaO2 > 92% and 12 had SaO2 < 92%.
Table 1: Demographic detail of patients. View Table 1
Eighty-eight patients had oxygen saturation of 92% or higher of which only one (1.13%) had respiratory failure. There were 7 patients with O2 saturation between 90% and 92%, out of which 2 (28%) had respiratory failure. In the third group, out of 5 patients with O2 saturation of less than 90%, 3 (60%) were found to have respiratory failure (Table 2). Respiratory failure is defined as (PaO2 < 60 mmHg and/or PaCO2 > 50 mmHg) as measured by ABG (Table 3).
Table 2: Summary of oximetry readings. View Table 2
Table 3: Arterial gases and oximetry of patients in respiratory failure. View Table 3
Pulse oximetry correlates well with the arterial partial pressure of oxygen (Figure 1).
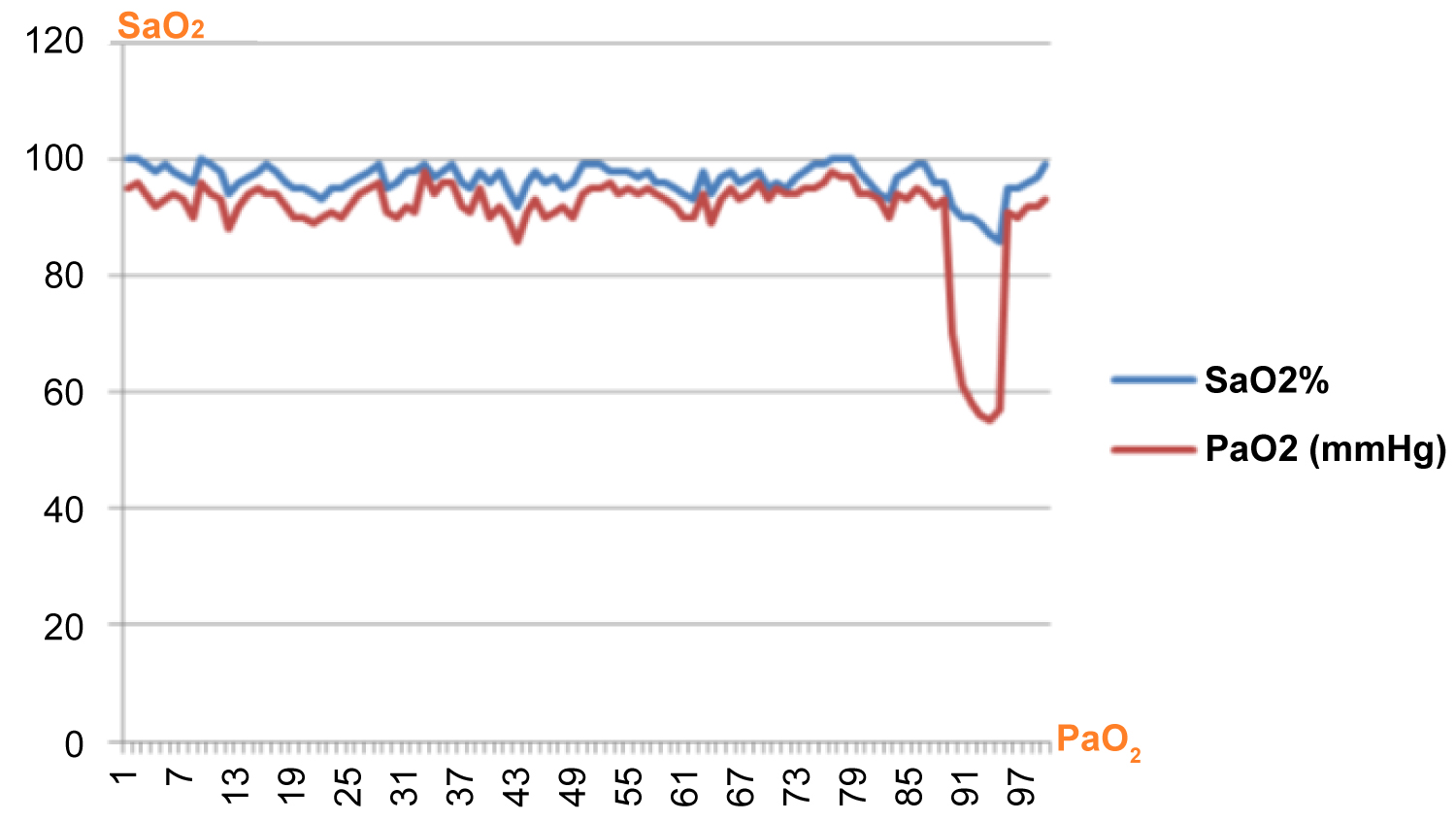 Figure 1: Correlation between SaO2 and PaO2.
View Figure 1
Figure 1: Correlation between SaO2 and PaO2.
View Figure 1
The correlation with the partial pressure of carbon dioxide is less clear, but the patient with severe hypoxia appears to have correspondingly higher PaCO2 (Figure 2).
 Figure 2: Correlation between SaO2 and PaCO2.
View Figure 2
Figure 2: Correlation between SaO2 and PaCO2.
View Figure 2
The study revealed a sensitivity of 83.33 and a specificity of 92.55. Moreover, the positive predictive value was 41.66 and the negative predictive value was 98.86. Additionally, the likelihood ratios were 11.18 for a positive test result and 0.18 for a negative result for patient who is SaO2 > 92%.
The results obtained from this study conveyed that oxygen saturation, measured by pulse oximetry, can give an indication of which patients require more rigorous care because they will experience respiratory failure. When oxygen saturation is 92% or greater, respiratory failure is highly unlikely. Therefore, blood gas analysis should be measured in patients with acute severe asthma whose SaO2 is below 92% on admission for the safe management of patients.
This is the same result reached by DM Carruthers, et al. in Respiratory Medicine Unit, Western General Hospital, UK [6].
Another study done by Gustavo J. Rodrigo, et al. in the United States revealed that an ABG test is only required for asthmatic patients whose oxygen levels were not restored to more than or equal to 90% (> 90%) after oxygen therapy. This is because pulse oximetry is a highly accurate and useful method to determine oxygenation levels [7].
When interpreting pulse oximetry in a clinical setting, it's important to take into account the limitations like recent smoking, nail polish, peripheral perfusion and cardiac arrhythmia.
History of recent smoking affects the results obtained from the pulse oximetry analysis. This is because oxygen saturation (SpO2) does not distinguish carboxyhemoglobin (COHb) from oxyhemoglobin (O2Hb). This gives a false impression of the apparent degree of oxyhemoglobin saturation in smokers who have elevated levels of COHb [8].
Exposure to smoking correlates with COHb levels; therefore, correction for smoking exposure is needed to improve the accuracy of pulse oximetry. Furthermore, it was observed that smokers always obtained high, inaccurate readings from the pulse oximetry analysis. In addition, it was observed that smoking a cigarette influenced the pulse oximetry results for up to four hours after the cigarette was consumed [9].
Therefore, I excluded any patient who had recently smoked (less than 4 hours). In this study there are 14 patients who are currently smokers, one had SaO2 below 92% and the rest (13 patients) had SaO2 above 92%.
Cardiac arrhythmias may cause very inaccurate measurements, especially if there are significant apex/radial deficits [10].
Only 2 patients in this study had atrial fibrillation with good peripheral pulse.
In conclusion, in severely ill patients, we can depend on pulse oximetry to predict hypoxic respiratory failure in patient with known medical history of asthma if initial value is > 92%.
This work is dedicated to my father and mother; for all the care and love they have given me. In addition to any member who supports me to achieve this study.