As the mortality in critical care patients reduces, post-intensive care syndrome grows as a public health concern, specially following outbreaks. Consequently, to address that problem, post-ICU follow-up programs emerged as a possibility to understand the long-term outcomes better and support ICU survivors. This study aims to state the prevalence of those programs in Belgium and comprehend how Belgians manage the care of ICU survivors.
We performed a national survey in Belgium on the management and current practices concerning the post-intensive care follow-up. The Belgian Society of Intensive Care endorsed this research. This survey had two validation processes (questionnaire validation by experts and questionnaire applicability by the pilot phase) following by the executive phase: Electronic distribution of the questionnaire to the ICU directors.
Forty-three percent (36/82) of ICU directors responded to our electronic questionnaire. Six centers (17%) currently run an ICU follow-up clinic. The first ICU follow-up clinic reported in Belgium was established in 2017. All clinics were composed by a multidisciplinary team, which had as responsible, in the majority of cases, a physician. The tools used to assess survivors diverged among centers; each center applied what they were familiar with or the tool that better fit their workload. The timing frame of consultations varied as well among centers. Three centers (50%) presented only one consultation at three months after discharge, and one center follows patients up to one year after discharge. Among those ICU departments that do not have an ICU follow-up program running currently, the majority would like to implement it. However, the lack of human resources and financial constraints were the two most frequent reasons mentioned that prevent centers from developing an ICU follow-up clinic.
A minority of Belgian ICUs ran a program to care for the ICU survivors. The ICU follow-up clinic's organization varied among centers, such as eligibility criteria and the tools to assess patients' impairments. The main obstacle for a post-ICU care program implementation was the lack of human and financial resources.
ICU follow-up clinic Post-ICU follow-up, ICU rehabilitation program, Belgium survey
EAM: European Association of Methodology EQ-5D - EuroQol 5-dimensions; GP: General Practitioner; HRQoL: Health-related Quality of life; ICU: Intensive Care Unit; LOS: Length of Stay; MV: Mechanical Ventilation; PICS: Post-Intensive Care Syndrome; QoL: Quality of life; SF-36: 36-item Short form Health Survey SIZ - Belgian Society of Intensive Care; WAPOR: World Association for Public Opinion Research
As the critically ill patients' mortality decreases, the concern about the burden from survival enhances. The term "post-intensive care syndrome" (PICS) nowadays encompasses all the impairments in the patients' mental, cognitive, or physical (physical and pulmonary function) status after critical illness and persisting beyond the acute hospitalization [1-5]. The prevalence of those disorders varies in the literature [6-11]. Patients might present symptoms from one, two, or even from the three categories at the same time [12,13]. The critical illness also impacts patients' quality of life after hospital discharge, even after physical rehabilitation, their quality of life persists lower than the general population [14-17].
The earliest ICU follow-up clinic reported in the literature was established in 1985 in the United Kingdom to identify and rehabilitate patients after the acute critical illness [18]. Lately, the concept of an ICU follow-up clinic focusing on evaluation and rehabilitation of intensive care survivors has emerged across the world. Despite the increasing concern about ICU survivors and their health-related quality of life, there is no international consensus to describe the ideal model to deliver care after ICU discharge, neither there is enough scientific evidence to support current models adopted in post-ICU follow-up [19-22]. Instead, each hospital or country establishes its program, relying on its policies, regulations, and resources [23].
In Belgium, there are no standard guidelines for the care of ICU survivors after hospital discharge. Likewise, there is no register on the prevalence of Belgian ICUs engaged in that sort of program and neither how they perform this long-term follow-up. Within this national survey, we aimed to assess Belgium's reality about ICU survivor's management and their current follow-up programs.
We conducted a national survey in Belgium to assess the implementation of programs for ICU survivors. Questions addressed the following issues: The frequency of implementation of those programs, their organization, and how their potential utility was perceived. This survey was designed based on the International Handbook of Survey Methodology sponsored by the European Association of Methodology (EAM) [24], the Survey Methods and Practices from Statistics Canada's National Centre [25], and the Revised WAPOR Code of Ethics, 2011. The survey has been approved by the Institutional Review Board of Erasme Hospital (IRB: P2018/443) and is endorsed by the Belgian Society of Intensive Care (SIZ).
We developed the research protocol which initially had its content validated by four experts [26]. They held a Ph.D. and MD credentials and had at least ten years of experience carrying out research. Three experts were specialists in intensive care medicine, and one expert was a specialist in the methodology of surveys and questionnaires.
A second validation was established with a pilot test. The method applied was stratified random sampling. We compose a sample per the geographical distribution of Belgian hospitals. Ten percent of hospitals in each region (Flanders, Wallonia, and Brussels) were included. Besides, to avoid sampling error, we electronically randomized the choices of each unit by using Microsoft Excel software. The following formula was used: = RANDBETWEEN (1, the total number of hospitals in each region) and F9 to continue the randomization until the exact number of services completes the sample.
After all the validation process, in March 2019, the questionnaire and the cover letter were addressed to all directors of ICUs in Belgian hospitals electronically. One questionnaire percenter. Hospitals with more than one site, only one site was considered to participate. The questionnaire was anonymous. Two weeks following the distribution, a reminder letter and the link to access the questionnaire were resent by email. Eight months later, a new reminder was sent by the Belgian Society of Critical Care, trying to increase the response rate.
Thirty-six from 82 distributed surveys were answered, indicating an overall response rate of 43% (Figure 1). Specifically, each region in Belgium (Flanders, Wallonia, and Brussels) contributed 35% (16/46), 46% (12/26), and 80% (8/10) of responses, respectively. The characteristics of responders are shown in Table 1. Six centers (17%) have an ICU follow-up program currently running. The first ICU follow-up clinic reported in Belgium was established in 2017 in the Flanders Region. Since then, one was established in 2018 in Brussels, following by two others in 2019 in Wallonia. Two responders did not specify the date of starting their program.
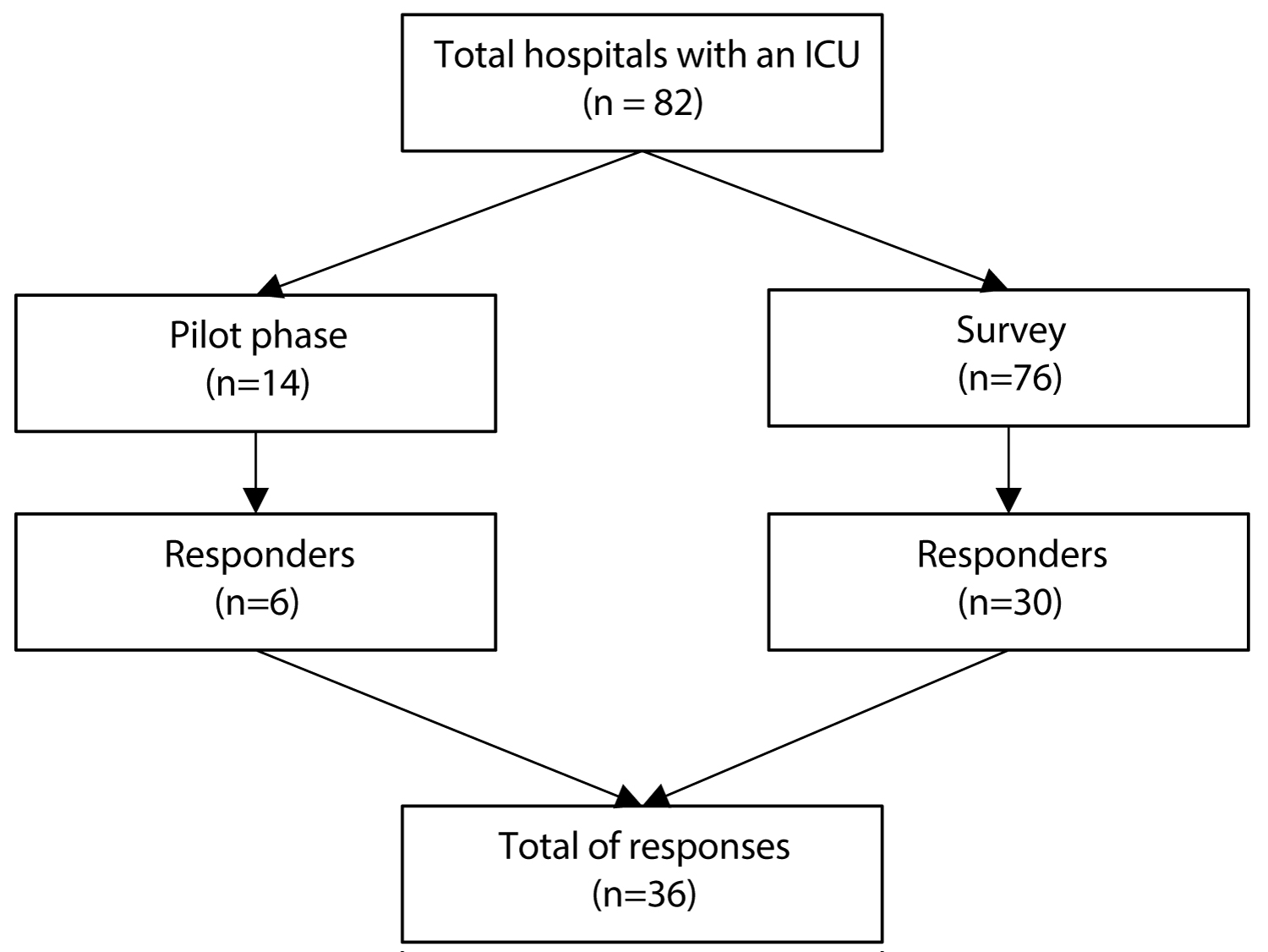 Figure 1: Flowchart of survey distribution stages and response rates.
View Figure 1
Figure 1: Flowchart of survey distribution stages and response rates.
View Figure 1
Table 1: Demographic characteristics of the responders per region. View Table 1
For all centers, the program was a multidisciplinary follow-up within at least two healthcare workers involved. The ICU follow-up clinic coordinator for the majority of responders was a physician (4/6). In centers nurse-led, a physician was available for the consultations, if requested. Four out of 6 centers worked with a physiotherapist in the team for a physical evaluation. Another healthcare worker often presents in the follow-up was a psychologist. In three out of 6 centers, the patients could discuss their emotions and feelings with a specialist.
The eligibility criteria to participate in the follow-up consultations varied among centers. However, a higher number of centers adopted the ICU length of stay (LOS) and the mechanical ventilation (MV) use as inclusion criteria. The most frequent outcome evaluated during consultations was the health- related Quality of life (HRQoL), which was assessed with the 36-item Short-Form Health Survey (SF-36) or with the EuroQol 5-dimensions (EQ-5D). For other patients' functional recovery, locally derived questionnaires were the tools most frequently used.
Regarding the consultations' timing frame, for three centers, the follow-up consultation was offered only once. For two centers, patients attended two consultations, finishing at six months after ICU or hospital discharge. One center followed the patients three times up to one year after discharge. After the ICU follow-up consultations in all centers, patients could be referred to a specialist if needed. The most common specialist was a clinical psychologist. Two centers involved the general practitioner (GP) as a vital role in decision-making for the patient. The GPs are responsible for referring patients to a specialist if deemed appropriate.
Regarding the financial aspect of the ICU follow-up clinic, only one center was funded with external or private rewards. The other five centers do not have any specific funds. Two departments used the budget of the hospital to afford the ICU follow-up activities partially.
Thirty centers out of 82 (83.0%) did not run an ICU follow-up clinic currently. For those, we sought to understand why they did not have an ICU follow-up program implemented, and if they would like to have one. Although 26 centers (86.6%) were interested in starting an ICU follow-up clinic, the lack of human resources (20/30 66.6%) and financial constraints (12/30 40.0%) were the main restrictions (Table 2).
Table 2: Reasons not to implement an ICU follow-up clinic. View Table 2
This survey showed that ICU follow-up clinics are not common in Belgium, in spite of a growing interest towards PICS. The lack of financial support is the main obstacle that prevents the implementation of a program focusing on the care and rehabilitation of those patients. The health system in Belgium is particularly complex and differs from the public health provision in the UK and the private health system in the USA. Probably, the lack of a guidelines for the care of ICU survivors adapted to the Belgian health system reality is another relevant barrier that should be raised in future research.
Although we achieved the possibility of sending the electronic questionnaire to the majority of ICU directors in Belgian hospitals, one limitation of our study is the response rate. Unfortunately, it only allowed an analysis of 43% of ICU departments. That makes us not be sure if the finding can be representative of the whole country.
In our survey, 17% of the centers had an ICU follow-up clinic currently with 67% in the physician-led structure. In a similar survey performed in 2006 by Griffiths, et al. in the UK, ICU follow-up clinics were present in 30% of the hospitals, and 55% were nurse-led [18]. Similar results were found in a survey conducted in the Netherlands and published in 2015, which showed that 40% of the centers had a follow-up for ICU survivors, and 70% were nurse-led [27]. In Denmark, a survey conducted in 2017 showed that 84% of the intensive care units had an ICU follow-up clinic running. The Scandinavian health system's organization can explain this higher implementation of a follow-up service in this country. They incorporated the ICU follow-up program into the standard care offered.
According to all surveys, the main barrier to provide an ICU follow-up program is the lack of resources (human and financial) [18,27-29]. In our survey, 40% of hospitals appointed funding as a problem, even among the centers running an ICU follow-up, 83% were not funded. In 2014, after the recommendations for post-ICU rehabilitation been published in the UK, Connolly, et al. conducted a new survey which measured the adherence of British intensive care units to the national guideline (NICE CG83), and only 27.3% of the organizations had a post-ICU clinic, again been the critical limiting aspect the lack of source of funding.
In conclusion, this survey has shown an estimated number of Belgian ICU departments engaged in ICU survivors' care after hospital discharge. The majority of the ICU with the no-follow-up program would like to improve this service in their organization. However, the lack of funding is the primary limiting. New health policies and plans for ICU survivor's management should be developed and implemented.
We acknowledge the Belgian Society of Critical Care staff members for endorsing and disclosing this research.