Background: The COVID-19 pandemic has led to millions of deaths throughout the world. Several randomized controlled trials have demonstrated that steroids reduce mortality in severe COVID-19 infection. The Center for Disease Control and Prevention has recommended dexamethasone as the first line of treatment. However, methylprednisolone is being used as the steroid of choice in many countries worldwide. We sought to perform a systematic review and meta-analysis to compare the outcomes with the use of these two steroids.
Methods: A literature search was performed on five databases - PubMed, Ovid Medline, Scopus, Web of Science, and Cochrane. Primary outcomes were mortality and the need for mechanical ventilation. Pooled odds ratio (OR) was calculated with a 95% confidence interval. Statistical analysis was performed using STATA 16.1 software.
Results: Five studies (four observational and one randomized controlled trial) were included in the meta-analysis. Pooled estimates showed a significant reduction in mortality (OR 0.60; 95% CI 0.41-0.86; p = 0.01) and need for mechanical ventilation (OR 0.48, 95% CI 0.24-0.96; p = 0.04) with methylprednisolone compared to dexamethasone. There was no difference in complications between the two groups (OR 0.46 95% CI 0.20-1.02; p = 0.06).
Conclusion: Our study shows that methylprednisolone was associated with a reduction in mortality and the need for mechanical ventilation. This suggests a higher dose of steroids or methylprednisolone may reduce mortality compared to the current standard of care. Large double-blinded randomized controlled trials are needed to assess the role of a higher dose of steroids.
COVID 19, Methylprednisolone, Dexamethasone, Steroids
The first case of novel coronavirus-19 disease (COVID-19) was reported in Wuhan, China in December 2019, leading to a global pandemic as declared by the World Health Organization (WHO) in March 2020 [1]. Unfortunately, it still continues to be a hostile pandemic [2,3]. The majority of infections result in mild symptoms of fever, cough, dyspnea, headaches, and myalgias. However, one global study estimates that about 33% of the hospitalized patients develop acute respiratory distress syndrome (ARDS) while 26% require intensive care unit (ICU) level of care and are associated with high mortality [4]. Recently, the more transmissible B.1.617.2 (delta) variant has resulted in higher incidence of ARDS in infected individuals [5].
ARDS from COVID-19 is caused by uncontrolled viral replication leading to a dysregulated host immune response associated with a massive efflux of cytokines, known as the cytokine storm release syndrome (CRS) [6,7]. Multiple studies have investigated therapies to mitigate these dysregulated immune responses, with corticosteroids being one of the drug classes. The use of corticosteroids has become a standard of care since the publication of the RECOVERY trial [7]. This trial showed a mortality benefit with intravenous (IV) dexamethasone compared to standard supportive care in mechanically ventilated patients with ARDS [8]. Other similarly designed studies evaluating corticosteroids have also revealed considerable mortality benefits with corticosteroids [3,9-11]. Although traditionally methylprednisolone has been the preferred agent in ARDS, dexamethasone has become the agent of choice among providers in the USA [12-14]. There is a paucity of data comparing methylprednisolone with dexamethasone in this patient population. Therefore, we conducted this systematic review and meta-analysis to understand better the role of dexamethasone versus methylprednisolone in COVID-19 management.
We designed and conducted our meta-analysis based on the patient intervention, comparison, and outcome (PICO) framework and in accordance with the Preferred Items for Systematic Review and Meta-Analysis (PRISMA) statement.
Patients: Patients hospitalized with a confirmed diagnosis of severe COVID-19. Severe COVID 19 infection was defined by radiological evidence of COVID 19 and the need for supplemental oxygen to maintain SpO2 more than or equal to 92%.
Intervention: Evaluation of methylprednisolone in severe COVID-19.
Comparison: Comparing dexamethasone in the management of severe COVID-19.
Outcome: Outcomes measured in terms of reduction in all-cause mortality, need for mechanical ventilation, length of hospital stay and adverse effects from steroid use.
A systematic literature search was conducted independently by two authors (DB and AA) utilizing five databases, including PubMed, Ovid Medline, Scopus, Web of Science, and the Cochrane database for articles comparing dexamethasone and methylprednisolone in hospitalized COVID-19 patients. We restricted our search to publications between December 1st, 2019, to July 7th, 2021. Searches were performed using the term "Methylprednisolone" AND "Dexamethasone" AND "COVID 19". Depending on each database, alternate forms of subject headings were included or excluded. The detailed search strategy is provided as part of the supplementary files.
All studies comparing methylprednisolone and dexamethasone in the treatment of COVID-19 infection among hospitalized patients were included in our meta-analysis. Only studies published in the English language or available in English translation were included. We included both prospective and retrospective studies. Any studies in the form of only abstracts, letters without original data, case reports, animal studies, or did not describe the comparison of methylprednisolone and dexamethasone were excluded.
Each published study was screened by the investigators' DB and AA according to PRISMA guidelines. A third investigator, UB, resolved any conflict during the selection process. Our study used an online tool, Rayyan [15], to collect, screen, and save the selected articles and adhere to PRISMA guidelines. Detailed information was manually collected from online text manuscripts, figures, and tables from the selected articles. The efficacy end-points were overall mortality and the need for mechanical ventilation. Data about length of hospital stay and adverse effects with steroid use was also collected, where available.
The quality of the included studies was assessed by the two investigators DB and AA, independently, and the third author, UB, resolved any discordances. We used the Risk of Bias In Non-Randomized Studies - of Interventions (ROBINS-I) tool for non-randomized studies and Cochrane Collaboration's tool for the randomized study for quality assessment [16,17].
The primary outcomes of interest were pooled all-cause mortality and the need for mechanical ventilation in COVID-19. Secondary outcomes were adverse effects with steroid use and length of hospital stay. Categorical variables were reported in percentages and continuous variables as means with standard deviation. The pooled estimates with a 95% confidence interval (CI) were synthesized by meta-analysis using the ‘DerSimonian-Laird random-effects model.' Heterogeneity across the included studies was assessed using inconsistency index I2. The heterogeneity was classified as low, moderate, and substantial heterogeneity when the inconsistency index was 25%, 50%, and 75%, respectively. The publication bias was to be assessed by visual inspection of the funnel plot and Egger's test. A P-value of < 0.05 was considered statistically significant. Statistical analysis was performed using STATA 14.2 (StataCorp. 4905 Lakeway Drive, College Station, Texas 77845 USA).
A total of 357 studies were initially identified. A total of 78 articles were chosen for detailed review. A total of five studies were selected for use in this meta-analysis. There were two retrospective and three prospective studies, one of which was a randomized controlled trial (RCT) [18-22]. There were a total of 743 patients from the five included studies. There were 379 patients in the dexamethasone group and 364 patients in the methylprednisolone group. Figure 1 demonstrates the study selection process. Table 1 lists the studies included in the meta-analysis and study characteristics.
 Figure 1: PRISMA flow chart for article selection. View Figure 1
Figure 1: PRISMA flow chart for article selection. View Figure 1
Table 1: List of studies included in the meta-analysis with details. View Table 1
The mortality rate in COVID-19 patients was significantly lower in the methylprednisolone group versus the dexamethasone group (19.2%, 70/364 vs. 34.03%, 29/379; OR 0.60; 95% CI 0.41-0.86; p = 0.01). Forest plot analysis of mortality rate is shown in Figure 2. There was low heterogeneity among the included studies (I2 = 0%). The need for mechanical ventilation was also lower in the methylprednisolone group compared to the dexamethasone group (24.7%, 90/364 vs. 39.5%, 150/379). The pooled odds ratio (OR) was 0.48 (95% CI 0.24-0.96; p = 0.04). Forest plot analysis of this outcome is shown in Figure 3.
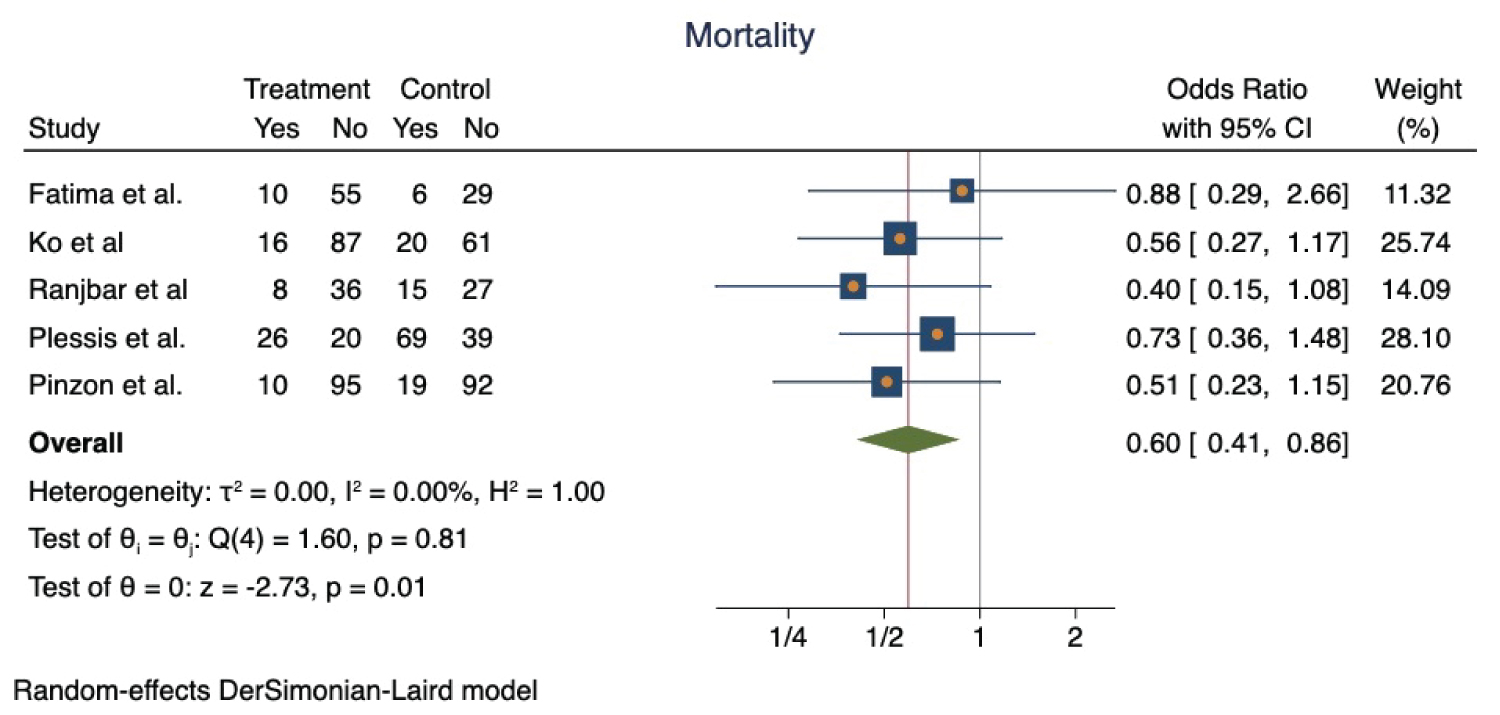 Figure 2: Forest plot for pooled odds ratio of mortality comparing methylprednisolone and dexamethasone. View Figure 2
Figure 2: Forest plot for pooled odds ratio of mortality comparing methylprednisolone and dexamethasone. View Figure 2
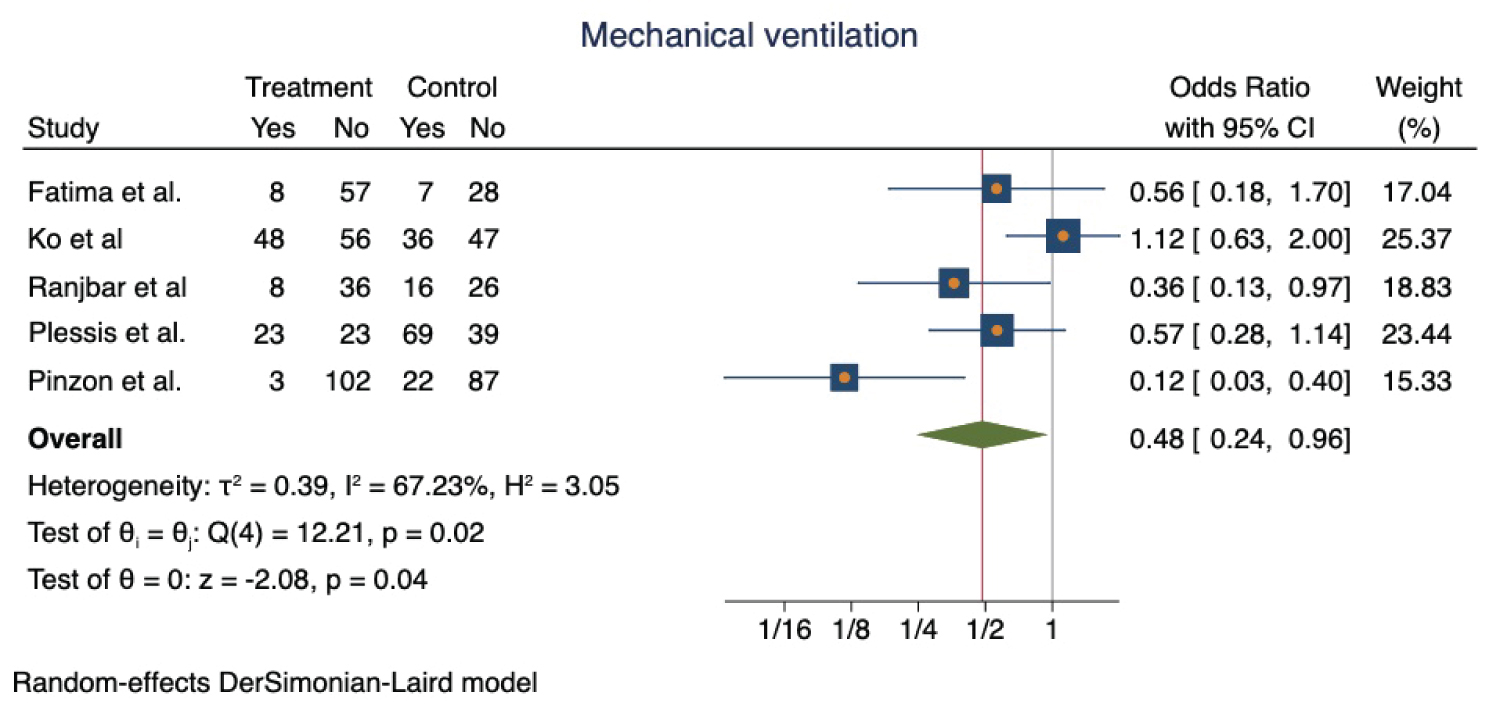 Figure 3: Forest plot for pooled odds ratio of need for mechanical ventilation comparing methylprednisolone and dexamethasone.
View Figure 3
Figure 3: Forest plot for pooled odds ratio of need for mechanical ventilation comparing methylprednisolone and dexamethasone.
View Figure 3
The incidence of adverse effects with methylprednisolone and dexamethasone groups was 26.6% (97/364) and 37.9% (144/379) respectively. The pooled odds ratio (OR) was 0.46 (95% CI 0.20-1.02; p = 0.06) suggestive of no statistically significant difference between the two groups. Forest plot analysis of this outcome is shown in Figure 4. Out of the five studies included in our meta-analysis, two of them (Ranjbar, et al. and Plessis, et al.) provided data about the length of hospitalization. There was no significant difference in the mean difference in the length of stay between the methylprednisolone and dexamethasone groups (-1.82 days; 95% CI, -3.82 - 0.18; p = 0.07). Forest plot analysis of this outcome is shown in Figure 5.
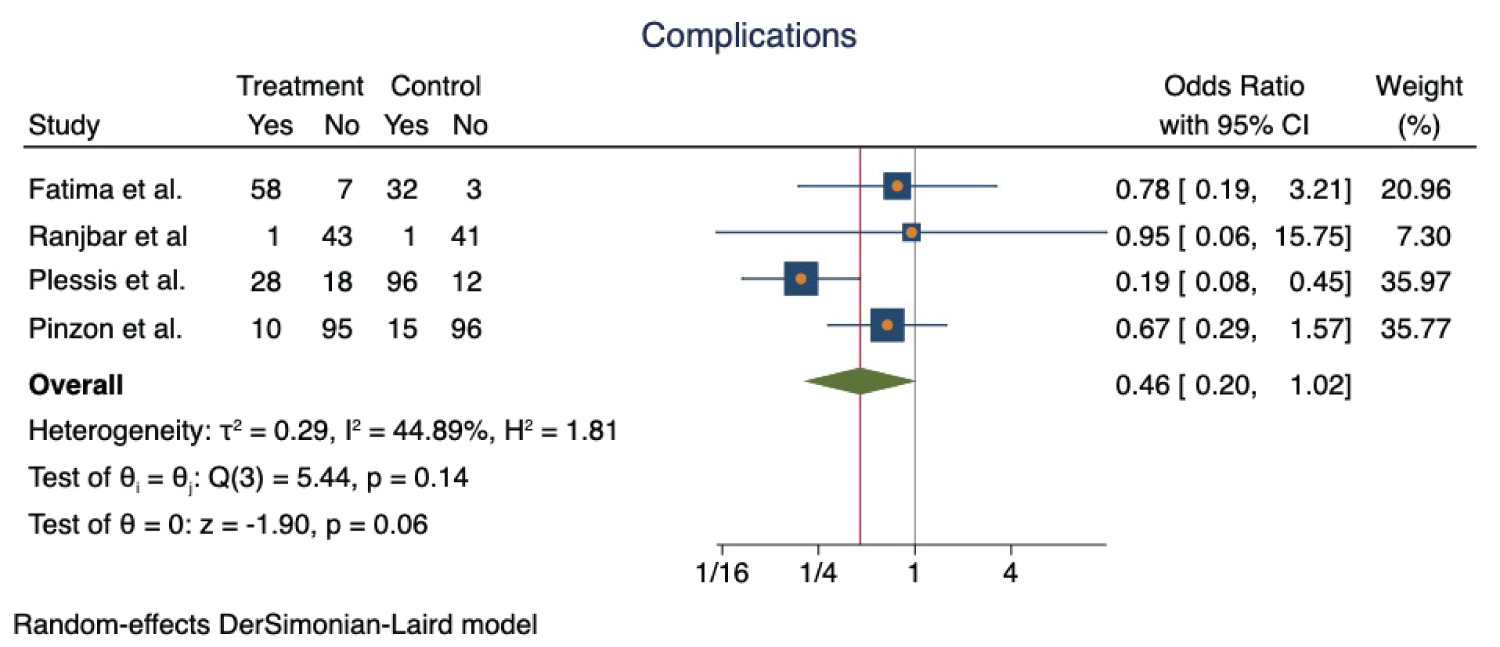 Figure 4: Forest plot for pooled odds ratio of adverse effects/complications comparing methylprednisolone and dexamethasone.
View Figure 4
Figure 4: Forest plot for pooled odds ratio of adverse effects/complications comparing methylprednisolone and dexamethasone.
View Figure 4
 Figure 5: Forest plot for pooled odds ratio of mean length of hospital stay comparing methylprednisolone and dexamethasone.
View Figure 5
Figure 5: Forest plot for pooled odds ratio of mean length of hospital stay comparing methylprednisolone and dexamethasone.
View Figure 5
The quality of the studies included in the metanalysis was graded based on the presence of selection bias, performance bias, detection bias, attrition bias, and reporting bias. ROBINS-I tool for non-randomized studies and Cochrane Collaboration's tools for the randomized study are shown in supplementary Figure 1 and Figure 2. Publication bias analysis for meta-analysis of fewer than ten studies is not useful, and therefore, we did not assess publication bias.
Our meta-analysis included three prospective and two retrospective clinical studies, with a total of 743 patients with COVID-19 infection requiring hospitalization [18-22]. The results indicated a significant reduction in mortality (OR 0.60, 95% CI 0.41-0.86) and the need for mechanical ventilation (OR 0.48, 95% CI 0.24-0.96) when methylprednisolone was used, compared to dexamethasone. There was no difference in adverse events (0.46, 95% CI 0.20-1.02; p = 0.06) or hospital length of stay (-1.82 days; 95% CI, -3.82 - 0.18; p = 0.07). The commonly reported adverse effects in the studies included were hyperglycemia, acute kidney injury, nosocomial sepsis and lung superinfection.
Current literature indicates that approximately 5% of the patients with COVID-19 develop severe ARDS and is the leading cause of mortality [23,24]. The dysregulation of cytokine production, resulting in early-onset organizing pneumonia, has been directly implicated to the severity of the disease [6]. The management of this entity has evolved with further understanding of this disease. At the onset of the pandemic, the Centers for Disease Control (CDC), Infectious Diseases Society of America (IDSA), and the WHO, all recommended against the use of corticosteroids for management of COVID-19 associated ARDS, based on previous experiences with other coronavirus outbreaks such as MERS-CoV and SARS-CoV-1 infection [25,26]. Previously documented adverse effects of steroid use included impaired host immune response, delayed viral clearance, risk of opportunistic infections, hyperglycemia, underreported delirium/psychosis, and increased mortality [19-21]. However, the results from subsequent large-scale RCTs have influenced a change in these initial recommendations.
Corticosteroids exert anti-inflammatory effects through genomic and non-genomic pathways and have been shown to reduce inflammation in lung disease [27]. A number of early trials demonstrated the mortality benefit of methylprednisolone in COVID-19 patients [27,28]. However, the use of steroids was not widely adopted until the preliminary results from the RECOVERY trial were released in June of 2020, now formally published [29,30]. The trial showed a reduction in the 28-day mortality by one-third in mechanically ventilated patients and one-fifth in hypoxic patients when treated with IV dexamethasone [8]. Subsequently, RCTs have confirmed the benefits of steroids in COVID-19 [9-11,31-33]. A recent meta-analysis also showed similar findings when comparing steroid administration to usual care (27.3 vs. 31.1%; RR: 0.85; 95% CI: 0.73-0.99; P = 0.04) [34].
However, there remains a wide variation in clinical practice worldwide regarding the dose and the choice of corticosteroid for COVID-19. In a Colombian study evaluating 216 hospitalized COVID-19 patients requiring oxygen, treatment with high dose IV methylprednisolone (500 mg daily for 3 days) followed by oral prednisone (50 mg daily for 14 days) was compared with IV dexamethasone 6 mg for 10 days. In their cohort, the methylprednisolone group of patients showed a significantly lower need for mechanical ventilation (19.8% vs. 2.9%) and ICU admission (14.4% vs. 4.8%), shorter recovery time (5-8 days vs. 3-4 days), lower inflammatory marker levels, and higher 30-day survival (63.1% vs. 92.6%) [18]. Consistent with these results, an Iranian study of 86 COVID-19 patients treated with IV methylprednisolone (2 mg/kg daily for 5 days, followed by a taper for 5 days) or IV dexamethasone 6 mg daily, also showed significantly lower mortality (18.6% in vs. 37.5%), shorter mean duration of hospitalization (7.43 ± 3.64 days vs. 10.52 ± 5.47 days), and lower needs for mechanical ventilation (18.2% vs. 38.1%) in the methylprednisolone group [22]. In another study conducted in Los Angeles, the 50-day mortality was found to be significantly lower in mechanically ventilated patients receiving at least 3 days of IV methylprednisolone 1 mg/kg/day compared to at least 7 days of IV dexamethasone 6 mg daily [19]. The quasi-experimental study from Pakistan showed comparable mortality when IV dexamethasone (8 mg/day) was compared to high dose IV methylprednisolone (1 mg/kg/day) in critically ill COVID-19 patients [12]. The observational cohort in South Africa demonstrated that results were equivocal when patients were sicker (mean P/F ratio < 100) and steroid doses were more comparable (hydrocortisone 100-200 mg 6-hourly vs. methylprednisolone 40 mg 12-hourly vs. dexamethasone 8 mg daily) [21].
The results of our meta-analysis showing that the use of methylprednisolone improved mortality in COVID-19 patients likely stems from higher doses of corticosteroids used. The equivalent dose of 6 mg of IV dexamethasone is 32 mg of IV methylprednisolone. The treatment effect seen may be dose-dependent. However, the tendency of methylprednisolone to concentrate in lung tissue more than dexamethasone may have also played a role in these results [35,36]. Ko, et al. demonstrated only a 31% mortality rate in patients on mechanical ventilation receiving 1 mg/kg/day of methylprednisolone; comparatively, the CODEX trial, where 20 mg of IV dexamethasone (equivalent to 106 mg of methylprednisolone) was used, demonstrated a 56.3% mortality rate in patients on mechanical ventilation [10]. Additionally, dexamethasone is longer acting than methylprednisolone, and consequently, the latter may have fewer side effects due to a shorter treatment duration [37]. One would argue that if these interventions had equivalent effects, there should not be a demonstratable difference between the outcomes with equivalent doses of these two corticosteroids.
There are several limitations to our study. First, the heterogeneity of the population and the compared interventions. None of the studies used equivalent doses of methylprednisolone compared to dexamethasone. This would make it difficult to draw conclusions solely based on the drug itself. Second, the retrospective nature of the included studies with the lack of large-scale RCTs results in the applicability of the conclusion drawn debatable. The results of this meta-analysis need to be further investigated in double-blinded RCTs. There are several ongoing trials, as listed in Table 2.
Table 2: Ongoing trials comparing dexamethasone with methylprednisolone in COVID-19. View Table 2
In summary, our meta-analysis reflects that methylprednisolone could have a potentially better effect than dexamethasone in treating severe COVID-19 infections in terms of a mortality benefit, prevention of mechanical ventilation, and reduced steroid-induced adverse effects. Results from larger double-blinded RCTs are needed to make further recommendations on whether methylprednisolone has mortality benefit over dexamethasone in treating severe COVID-19 related ARDS.