Introduction: The novel coronavirus disease 2019 (COVID-19) can be transmitted to clinicians involved in their care, particularly during aerosol-generating procedures. In spite centers for disease control and prevention (CDC) had put clear standards for precaution when dealing with such patients but unfortunately several health care providers had lost their lives around the world.
Objectives: To evaluate virtual/in-person medical simulation training about airway management of suspected/confirmed COVID-19 pediatric patients on pediatric health care provider in KFMC.
Methods: Cross-section study done on pediatric health care providers at King Fahad Medical City (KFMC), Riyadh, Saudi Arabia through google form questioner. Inclusion criteria: Health care providers involved in pediatric airway management for confirmed/suspected Covid-19 patients at KFMC, whether they attended virtual/in-person simulation training courses or didn't attend. We decided in this study to transmit the guideline on airway management for confirmed/suspected Covid-19 pediatric patients into simulation training courses to be run into in-situ simulation for multidisciplinary team, then when in situ area was converted into covid-19 care area we video tape this course and add it as QR barcode to the guideline.
Results: 70% of the responders had attended virtual/in-person simulation training, majorities were able to follow the guideline steps during airway management of suspected/confirmed COVID-19 pediatric patients. 85% of responders indicate that, simulation training either hands-on or video demonstration had helped them in Airway management for confirmed/suspected COVID-19.
Discussion: Most of the studies share the importance of generating guideline for pediatric airway management of suspected/confirmed COVID-19 pediatric patients. Adding simulation training as QR code to the guideline make it readily and easily accessed by healthcare providers and are crucial for involved health care providers for safe and best care.
Guideline, Simulation, COVID-19, Healthcare, QR barcode
The novel coronavirus disease 2019 (COVID-19) can be transmitted to clinicians involved in their care, particularly during aerosol-generating procedures such as, Positive pressure ventilation (PPV), endotracheal intubation and extubation [1]. In spite centers for disease control and prevention (CDC) had put clear standards for precaution when dealing with such patients but unfortunately several health care providers had lost their lives around the world [2]. For these reasons several countries had mobilized towards proper training and establishing guidelines to protect both patients and healthcare providers in preparing for the airway management of the COVID-19 patient group. The principles for airway management should be the same for all patients with COVID-19 (asymptomatic, mild or critically unwell). Safe, simple, familiar, reliable and robust practices should be adopted for all episodes of airway management for patients with COVID-19 [1]. Centers around the world had used different modalities to train health care providers on management of Covid-19 airway. Simulation bloomed during the epidemic due to its flexibility and capacity to train large number of health-care professionals at different levels in a timely manner either individually or in multidisciplinary teams through experiential learning. But simulation-based activities were limited due to multiple factors. Such as, infection control and social distancing measures, converting simulation centers into Covid-19 care area, financial and manpower limitations are other factors, attendance was suboptimal due to participants' fear of contracting the infection during the sessions, the shortage of available personal protective equipment. The busy schedule of both the trainers and trainees plus budget constraints and the limited availability of simulation technologists and support staff further exacerbated the aforementioned hindrances [3]. So we decided in this study to transmit the guideline on airway management for confirmed/suspected Covid-19 pediatric patients, which was created in our institute KFMC into simulation training courses to be run into in-situ simulation for multidisciplinary team, then when in situ area was converted into Covid-19 care area we agreed to video tape this course and add it as QR barcode to the guideline to be readily and easily accessed by any healthcare provider in the King Fahad Medical City (KFMC) institute.
To Evaluate virtual/in-person medical simulation training about airway management of suspected/confirmed COVID-19 pediatric patients on pediatric health care provider in KFMC.
Cross-section study done on pediatric health care providers at King Fahad Medical City (KFMC), Riyadh, Saudi Arabia through google form questioner. Inclusion criteria: Health care providers involved in pediatric airway management for confirmed/suspected covid 19 patients at KFMC, whether they attended virtual/in-person simulation training courses or didn't attend. So we decided in this study to transmit the guideline on airway management for confirmed/ suspected Covid-19 pediatric patients, which was created in our institute KFMC into simulation training courses to be run into in-situ simulation for multidisciplinary team, then when in situ area was converted into Covid-19 care area we video tape this course and add it as QR barcode to the guideline to be readily and easily accessed by any healthcare provider in the KFMC institute.
The questioners were sent electronically to all pediatric health care providers at KFMC whom fulfill inclusion criteria. It indicates if the simulation courses had helped the health care provider on proper personal protection equipment (PPE) during donning, doffing and on prevention of aerosol transmission Covid-19 infection during detailed steps of airway management as pre-oxygenation, intubation and extubation (Appendix A).
All categorical variables were presented as numbers and percentages. The comparison of the practice of pediatric airway management training for suspected/confirmed COVID-19 patients utilizing medical simulation between physicians and nurses had been conducted using Fischer Exact test. A P-value of 0.05 was considered statistically significant. The data were analyzed using Statistical Packages for Social Sciences (SPSS) version 26 (Armonk, NY: IBM Corp, USA).
This cross-sectional study evaluates healthcare providers' (HCPs) pediatric airway management training for suspected/confirmed COVID-19 patients utilizing medical simulation. As described in Table 1, nearly 70% of HCPs attended hands-on simulation training on airway management for confirmed or suspected COVID-19 patients. Of them, 61% had attended once. The prevalence of HCPs who attended video demonstrations on airway management for confirmed or suspected COVID-19 was 81.4%. Of them, 65.2% attended at least once. The proportion of HCPs who were involved in airway management on real confirmed or suspected COVID-19 pediatric patients was 59.3%. Of those who were involved, 34.3% provided IV medications.
Table 1: Assessment of Pediatric Airway Management Training for suspected/Confirmed COVID 19 patients utilizing Medical Simulation (n = 59). View Table 1
Table 2a and Table 2b presented the HCPs practice for those who were involved in airway management on real confirmed or suspected COVID-19 pediatric patients. Based on the results, 3 HCPs were not able to wear PPE completely with unavailability of PPE reported by 2 HCPs. Also, approximately 14.3% were partially or were not able to learn (5.7%) the precautions during intubation and the most common obstacle was the unavailability of a nylon cover (85.7%). The most common BVM ventilation method was the VE maneuver (65.7%). A high proportion of HCPs (80%) reported that the timing of inflation of the ETT cuff was done properly. Confirmation of intubation was done by both visualization and End-PCO2 (65.7%). Proper discarding of soiled equipment was reported by 85.7% and proper doffing was reported by 97.1%. During extubation, proper wearing of PPE according to the role was reported by 82.9%. Nearly all HCPs (91.4%) used protective sheets and most of them (88.6%) were carefully done the sequence of proper extubation precautions. Of those who were not able to achieve proper extubation precautions (n = 4), 2 of them stated that the nylon covers were unavailable at that time and the other 2 said, PPE was not available. Approximately 88.6% of HCPs indicated that the time required for donning and doffing is longer in COVID-19 cases than in other cases. Similarly, 80% and 51.4% of HCPs reported that the procedure for intubation and extubation for confirmed/suspected COVID-19 patients is more difficult than the other patients. The proportion of HCPs who reported that the simulation training either hands-on or video demonstration had helped them in airway management for COVID-19 cases was 85.7%. In addition, 82.9% indicated that they reviewed the guidelines for airway management related to COVID-19 patients (Figure 1).
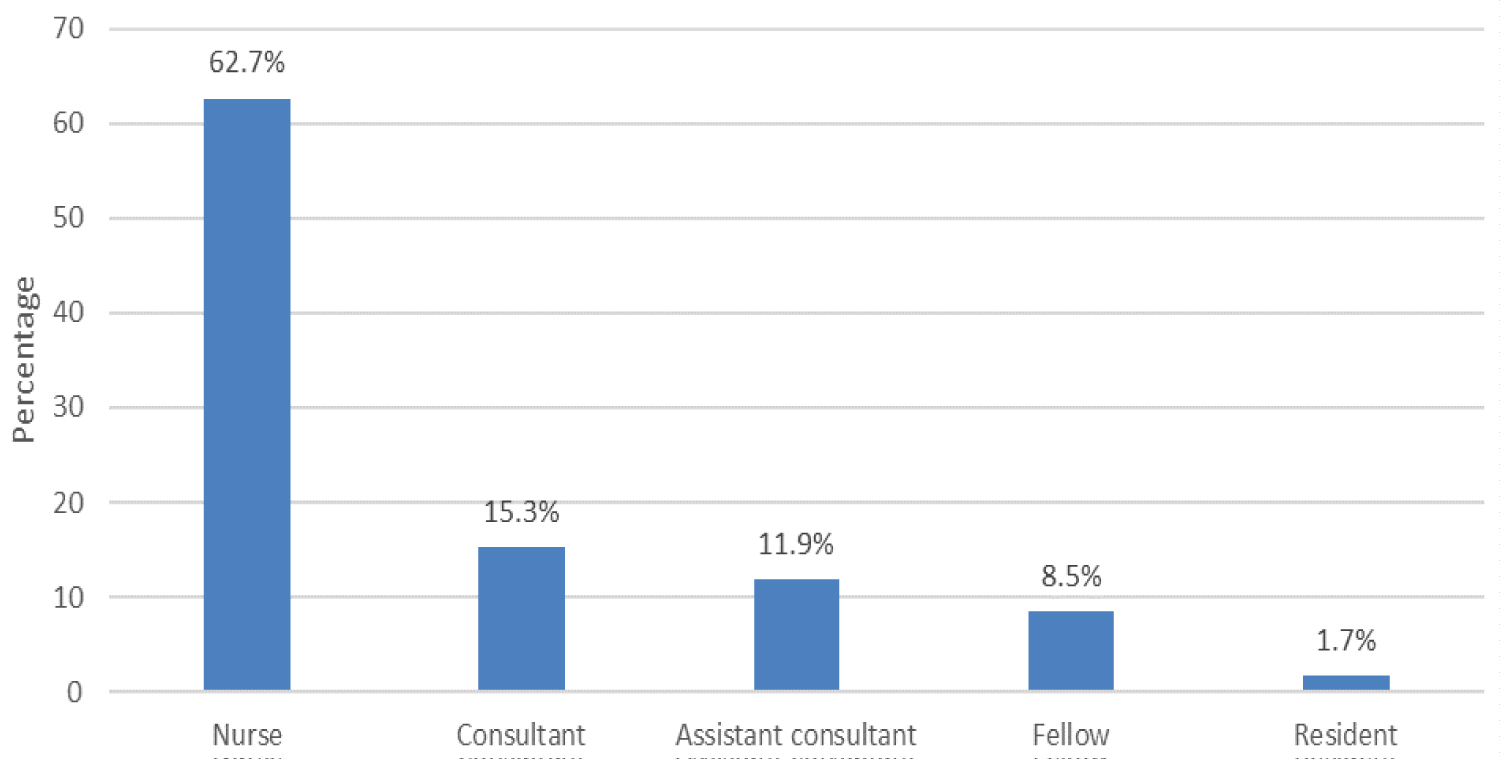 Figure 1: Distribution of the position of the sample population. View Figure 1
Figure 1: Distribution of the position of the sample population. View Figure 1
Table 2a: Healthcare provider practice on airway management on real confirmed or suspected COVID-19 pediatric patients (n = 35). View Table 2a
Table 2b: Healthcare provider practice on airway management on real confirmed or suspected COVID-19 pediatric patients (cont'd.) (n = 35). View Table 2b
In Table 3, the prevalence of those who attended hands-on simulation training for airway management (p = 0.041) and those who attended a video demonstration (p = 0.004) was significantly more among physicians while there were no significant differences in their involvement in airway management in actual confirmed/suspected COVID-19 pediatric patients between physicians and nurses (p = 0.412).
Table 3: Assessment of Pediatric Airway Management Training for suspected/Confirmed COVID 19 patients utilizing Medical Simulation between physicians and nurses (n = 59). View Table 3
In Table 4, the use of the VE maneuver as a method of BVM ventilation (p = 0.034), and the use of video laryngoscope (p = 0.012) were significantly more among physicians while the use of both visualization and end-PCO2 to confirm intubation was significantly more among nurses (p < 0.001). Other related practices on airway management on real confirmed or suspected COVID-19 patients were not significantly different between physicians and nurses including following the learned precautions during the intubation period (p = 0.680), clamping of ETT before inflating the cuff (p = 0.193), proper timing of inflation of ETT cuff (p = 0.831), the procedure of extubation for COVID-19 patients (p = 0.435) and review of institute guideline for airway management (p = 0.207).
Table 4: Practice on airway management on real confirmed or suspected COVID-19 pediatric patients between physicians and nurses (n = 35). View Table 4
Most of the studies share the importance of generating guideline on pediatric airway management. For many years, WHO has been working with countries to prepare for a global pandemic and has published guidance to help all countries prepare and brace for future outbreaks. For countries where resources are scarce or where there's risk of overwhelming a fragile health system, WHO has published guidance on COVID-19 preparedness and response in low capacity and humanitarian settings [4,5]. The Pediatric Difficult Intubation Collaborative (PeDI-C), which includes 35 hospitals from 6 countries, generated guidelines on airway management in pediatric anesthesia based on expert opinion, they identified certain goals including minimizing aerosolized respiratory secretions and number of clinicians in contact with a patient, use of in-line suction catheters, using appropriate personal protective equipment when performing aerosol-generating medical procedures in asymptomatic children, Airway procedures should be done in negative pressure rooms when available [6]. Airway management of patients with Covid-19 is a high-risk procedure, COVID-19 airway should be considered as potentially difficult and complicated. Triaging, personal protective equipment and isolation areas may cause challenges [7]. Beside The importance of creating an airway management team and the closed loop communication for managing COVID-19 airway [8]. Cook TM, et al. recommended to develop principles for airway management of patients with COVID-19 to encourage safe, accurate and swift performance [8]. In the Italian group's study, the use of checklist was put forward as it becomes extremely important for effective planning before tracheal intubation of Covid-19 patients [9]. Cheung JC, et al., recommend that endotracheal intubation is done by an expert specialized person and as early as needed. And if manual bagging is required, they suggested gentle ventilation via a supraglottic device instead of bag mask ventilation and to utilize a continuous waveform capnography monitoring device as it reflects correct endotracheal tube placement. Also they recommend Rapid sequence induction technique preferably rocuronium over suxamethonium for its longer half-life, which effectively prevents coughing or vomiting. ETT cuff should be inflated immediately to avoid leakage. The endotracheal tube should be connected to the ventilator via a filter [10]. Brewster DJ, et al. also recommended the use of a second-generation supraglottic airway device as its higher seal pressure during positive pressure ventilation decreases the risk of aerosolization of virus-containing fluid particles [1]. Video laryngoscopy can be used as an alternative to direct laryngoscopy for training and assessment in tracheal intubation in clinical settings and believe that all patients with COVID-19, and ideally every patient during the pandemic, should be intubated using video laryngoscopy [6,8,9,11,12]. During this pandemic, we encourage colleagues to prepare for difficulties during tracheal intubation and extubation as several reported cases of covid-19 association with airway edema, so especially emphasized that more care should be taken after documented difficult airway management or prolonged tracheal intubation. Advanced techniques in extubation include tube exchange catheters, Bailey maneuver and staged extubation set [13-15].
Several studies recommend to reduce the use of noninvasive ventilation and high flow oxygenation to reduce aerosolization [9]. Cheung JC, et al. documented that High Flow Nasal Cannula is recognized by World Health Organization for the treatment of patients with respiratory failure caused by COVID-19. However, the use of airborne isolation was recommended because the system can theoretically increase the risk of viral spread through aerosol generation [10]. Other studies concentrated on personal protected equipment PPE during caring for COVID-19 patients, Careful planning developing processes to ensure that PPE is readily available, simulations and training of staff are crucial to ensure the safety of patients and healthcare workers, they recommended that hospitals must modify their airway management and PPE guidelines based on feedback from clinicians on the ground and improved understanding of the transmissibility of the virus [16].
Pre-pandemic, simulation training courses on pediatric airway showed its efficacy. S Alyousef, et al. demonstrated that, the pediatric airway management simulation course at CRESENT, KFMC is effective in improving the knowledge and practical skills of pediatric residents. Although the greatest improvement is noted among junior residents, learners from different residency levels have comparable knowledge and practical skills at the end of the course [17].
Comparing pre-pandemic difficult airway guidelines with the recent COVID-19 guidelines, and then valuing, and understanding of these differences and modifications had led to greater adherence to the new COVID-19 guidelines mainly related to minimizing aerosol contamination and protecting healthcare workers [18]. Our study share similar outcome with Di Pan, et al. which stated, healthcare simulation training for Covid-19 patients, not only helped carry our institution through the peak of patient surge during the pandemic, but left us with lasting improvements in the function of our organization and crisis resource management [19]. Via Abatzis, et al. healthcare simulation training has many opportunities for reinforcement and refinement of the critical skills, mainly gaining feedback that led to protocol refinement. We were able to decrease unnecessary risk from learning "on-the-fly", in a clinical setting that has demonstrated high-risk for nosocomial transmission. This is helping to keep team members healthy and ready to care for our sickest, and most vulnerable patients [20]. So for these reasons we decided to transmit the guideline on airway management for confirmed/suspected Covid-19 pediatric patients, which was created in our institute KFMC into simulation training courses to be run into in-situ simulation for multidisciplinary team, then when in situ area was converted into Covid-19 care area we agreed to video tape this course and add it as QR barcode to the guideline to be readily and easily accessed by any healthcare provider in the KFMC institute. 85% of responders indicate that, simulation training either hands-on or video demonstration had helped them in Airway management for confirmed/suspected COVID-19 while 14% indicate it partially helped.
The novel coronavirus disease 2019 can be transmitted to clinicians involved in their care, particularly during aerosol-generating procedures such as, Positive pressure ventilation, endotracheal intubation and extubation. Several precautions should be taken during the care to these patients, one of the best way is either in person simulation training or videotape these courses and adding it as QR barcode to the guideline of Pediatric airway management for confirmed/ suspected Covid-19, make it readily and easily accessed by healthcare providers and are crucial for involved health care providers for safe and best care.
We recommend to apply virtual or in person simulation training to clinical medical guideline and add it as QR barcode to the guideline.
All the authors confirm that there are no conflict of interest and nothing to disclose.