Chronic kidney disease (CKD) represents a worldwide public health problem, Mexico has a prevalence of 12.2%, of which 52,000 patients are in renal replacement therapy and 80% are treated at the Mexican Social Security Institute, it is associated with early mortality with a higher incidence after 40 years of age. The literature mentions severe metabolic acidosis, severe hyperkalemia and hyperphosphatemia, water overload and uremic syndrome as frequent causes of dialysis urgency. However, the most frequent dialysis emergency in our setting has not been studied.
To establish the most frequent cause of dialysis emergencies and to identify the precipitating factor in patients with chronic kidney disease admitted to the emergency department of Hospital General Zone (HGZ) 50, Mexico.
Analytical and retrospective study, the sample was obtained by calculating the finite sample (Murray's formula) of patients admitted to the emergency department over a period of one year, as well as descriptive statistics (measures of trend, central, ranges, frequencies, proportions, chi-square to establish associations), SPSS software was used. Results. Data were collected from 148 patients.
Severe metabolic acidosis was identified as the main cause of dialysis urgency (29.1%) and the main precipitating factor was the presence of infections at any level (33.8%).
Refractory metabolic acidosis is the main dialysis emergency in our patients, it is important to perform gasometry on admission in the ED, the main precipitating factor is the presence of infection, so initiating timely treatment and immediately requesting renal replacement therapy, as well as providing sanitary and preventive measures will have a positive impact on reducing morbidity and mortality.
Chronic kidney disease, Dialytic urgency, Treatment
CKD: Chronic Kidney Disease; HGZ: Hospital General Zone; MSSI: Mexican Social Security Institute; LASNH: Latin American Society Of Nephrology and Hypertension; AKI: Acute Kidney Injury; BUN: Blood Urea Nitrogen; PTH: Parathyroid Hormone; FGF-23: Fibroblast Growth Factor -23 (FGF-23); ABC: Airway, Breathing and Circulation
Chronic Kidney Disease is a generic term that includes a group of diseases that affect the function and structure of the kidney, evidenced by serum, urinary or imaging markers of renal damage and/or a theoretical glomerular filtration rate of less than 90 ml/min/1.73 m2 body surface area, for a period greater than or equal to 3 months, regardless of the cause [1-3].
Morbimortality figures are alarming worldwide, and it represents a serious public health problem in Mexico and the world. As it is a disorder of multifactorial origin and is strongly associated with the most prevalent chronic diseases in our population, such as diabetes and arterial hypertension, its impact on public health is reflected in the high demand for human, economic and infrastructure resources that its treatment requires [4-6].
In Mexico, the incidence is estimated at 377 cases per million inhabitants with a prevalence of 1,142, of which 52,000 patients with kidney disease receive renal replacement therapy and 80% are treated by the Mexican Social Security Institute (MSSI) [6].
The Latin American Society of Nephrology and Hypertension (SLANH) mentions that in Latin America an average of 613 patients per million inhabitants had access in 2011 to one of the treatment alternatives for the substitution of the function that their kidneys can no longer perform: Hemodialysis, peritoneal dialysis, and kidney transplantation [7].
In the last decade, risk factors have been identified that, due to their high prevalence in the population, increase the cases of chronic kidney disease; among the most important risk factors are obesity, arterial hypertension, obstructive uropathies, smoking, consumption of nephrotoxic drugs and diabetes mellitus [8-10].
With time, CKD progresses to more advanced stages, so the mainstay in the treatment and follow-up of these patients is to prevent or slow its progression by means of strategies aimed at reducing risk factors, with timely diagnosis and appropriate treatment [8].
One of the main complications of chronic kidney disease are the causes of dialytic urgency. According to Bello and Nieto, dialytic urgency is the need to perform renal replacement therapy in the shortest possible time to prevent fatal complications. The causes of dialysis urgency are:
• Pulmonary edema in the context of oliguria or anuria in patients with AKI or CKD.
• Progressive volume overload in an oligoanuric patient (usually balances greater than 10 liters).
• Severe hyperkalemia (serum potassium > 6.5 mmol/L) or with electrocardiographic changes, without response to medical management.
• Severe hypermagnesemia without response to medical management (serum magnesium > 10 mg/dl).
• Hypercalcemia refractory to medical management (serum calcium > 15 mg/dl).
• Severe hyperphosphatemia refractory to medical management (serum phosphorus > 10 mg/dl).
• Severe metabolic acidosis associated with renal failure, usually with pH < 7.15, unresponsive to medical management.
• Complications of uremia such as encephalopathy, pericarditis, pleuritis, neuropathy or bleeding.
• Progressive severe uremia refractory to management, usually with blood urea nitrogen (BUN) > 100 mg/dl.
• Severe poisoning by dialyzable substance.
• Symptomatic severe acute dysnatremia (sodium > 160 mmol/L or < 120 mmol/L).
• Severe hyperthermia refractory to management (T ≥ 41 ℃).
• Severe hyperammonemia in patients with acute liver failure [10].
Factors that precipitate the patient being in a dialytic emergency are the following: failure to attend dialysis treatment, failure to initiate dialysis when it was necessary, and skipping peritoneal dialysis sessions [11]. The mortality of patients in dialysis emergencies, even if renal replacement therapy is performed, is 20% in the hospital setting and reaches 50% in the intensive care unit [12]. Within the treatment of dialytic emergencies, there are immediate indications to perform dialytic therapy such as: hyperkalemia with ventricular arrhythmias or heart block; severe metabolic acidosis associated with renal failure that does not respond to management (pH < 7.15); uremic complications such as encephalopathy, pericarditis, and uremic bleeding; severe poisoning by dialyzable substances; and pulmonary edema of renal origin in a patient who is oligoanuric and not intubated [13].
Severe hyperkalemia is defined by a serum potassium > 6.5 mmol/l, it is a potentially fatal condition and represents a medical emergency, it is the most common electrolyte disturbance in patients with chronic kidney disease, the main clinical manifestations are fatigue, muscle weakness and cardiac arrhythmias, the latter significantly increasing the risk of sudden death. Treatment includes membrane stabilizers with calcium salts, either calcium gluconate or calcium chloride. Another strategy is sodium bicarbonate, which causes transcellular redistribution of potassium by stimulating transmembrane H/K exchange, Na/H exchange, sodium bicarbonate cotransport and Na/K ATPase; however, it is not a first-line strategy. Additionally, intravenous administration of loop diuretics combined with thiazides or similar, can be considered in patients with hyperkalemia and hypervolemia. Finally, oral or rectal administration of ion exchange resins together with sorbitol can be performed with the aim of increasing potassium elimination in the distal colon [14].
Acute nephrogenic pulmonary edema is a dialysis emergency because it is a complication due to the presence of fluid in the interstitial and alveolar space in greater quantity than physiological, if it is not controlled it produces multiorgan failure, a process called "organ croos-talk". It causes acute respiratory failure, due to abnormality in the ventilation-perfusion relationship that causes deterioration in gas exchange and pulmonary mechanics. This clinical condition appears when the amount of water increases to double the normal amount, requiring immediate treatment with oxygen, diuretics, and sometimes advanced airway management, as well as emergency dialysis to improve the survival of these patients [15].
Patients with renal disease, with glomerular filtration rate < 60 ml/min, have abnormalities in mineral and bone metabolism, such as elevated parathyroid hormone (PTH), increased fibroblast growth factor-23 (FGF-23), increased fractional excretion of phosphorus, no elevation of urine phosphorus 24 hours and decreased calcitriol. This association increases all-cause mortality, even with normal blood phosphorus levels, and is due to increased valvular and vascular calcifications, which increase the risk of a cardiovascular event. Treatment of hyperphosphatemia is based on low-phosphorus diet, phosphorus binders such as calcium carbonate, calcium acetate, sevelamer, lanthanum and aluminum as well as emergency dialysis [16].
The prevalence of metabolic acidosis is 15%, however, its prevalence increases with worsening renal function; one study described a prevalence of 37% in patients with a glomerular filtration rate of less than 30 ml/min. Reduced glomerular filtration rate is the most important risk factor. Metabolic acidosis is defined as a serum tCO2 < 22 mEq, a pH less than 6.8 is incompatible with life and this exponentially increases the mortality of these patients, so severe drug-resistant metabolic acidosis is considered a dialytic emergency [17]. Moioli, et al. as well as Kinoshita, et al. published that urgent renal replacement therapy is effective in the control of severe metabolic acidosis, there are drugs that can decrease acidemia such as pyruvate, bicarbonate, tromethamine, spermidine and pharmacological inhibition of NHE-1; however, the use of these drugs have adverse effects [18].
A syndrome characterized by delirium in patients with untreated or inadequately treated renal disease; however, the toxins causing uremia to have not been definitively identified. Brain amino acid metabolism may be impaired in such cases, leading to an imbalance between inhibitory and excitatory neurotransmitters and the accumulation of false neurotransmitters categorized as intermediate molecules. The risk of developing uremic encephalopathy appears to be elevated in anuria patients on peritoneal dialysis. Inflammatory mediators and oxidative stress as well as uremic solutes are thought to contribute to the pathogenesis of central nervous system disorders in patients with impaired renal function. Within the electroencephalogram manifestations the most common with prominent slow waves, θ intermittent frontal rhythmic activity is also frequent. Uremic encephalopathy is reversed with dialysis, hemodialysis, or combined therapy, however, prior to entry to such therapy, it is required to maintain airway, breathing and circulation (ABC) until basal alertness is recovered after the hemodialysis session. In anuric patients on peritoneal dialysis treatment require hemodialysis, combined therapy is a good option in these patients and is the only way to reverse encephalopathy in this type of patients described in the literature [19].
Analytical and retrospective study, the sample was obtained by calculating the finite sample (Murray's formula) of patients admitted to the emergency department of the hospital general de zone 50, San Luis Potosi, Mexico, over a period of one year (240 patients) as well as descriptive statistics (measures of trend, central, ranges, frequencies, proportions, chi-square to establish associations), SPSS software was used.
Murray's formula:
Where:
-n = is the size of the population sample to be obtained.
-N = is the size of the total population (240 patients in one year).
-σ = Represents the standard deviation of the population (50%)
-Z = is the value obtained using confidence levels (95%)
-e = Represents the acceptable limit of sampling error (5%)
-p = Probability of success (50%). Therefore, the sample size to be obtained is 148 patients.
We included 148 patients admitted to the emergency department of the Hospital General de Zone 50 in San Luis Potosi, Mexico, of which 55 were women and 93 men, corresponding to 37.16% and 62.84% respectively (Graph 1), the average age was 53.7 years with an age range from 17 years to 94 years (Table 1 shows the measures of central tendency).
 Graph 1: Frequency of sex.
View Graph 1
Graph 1: Frequency of sex.
View Graph 1
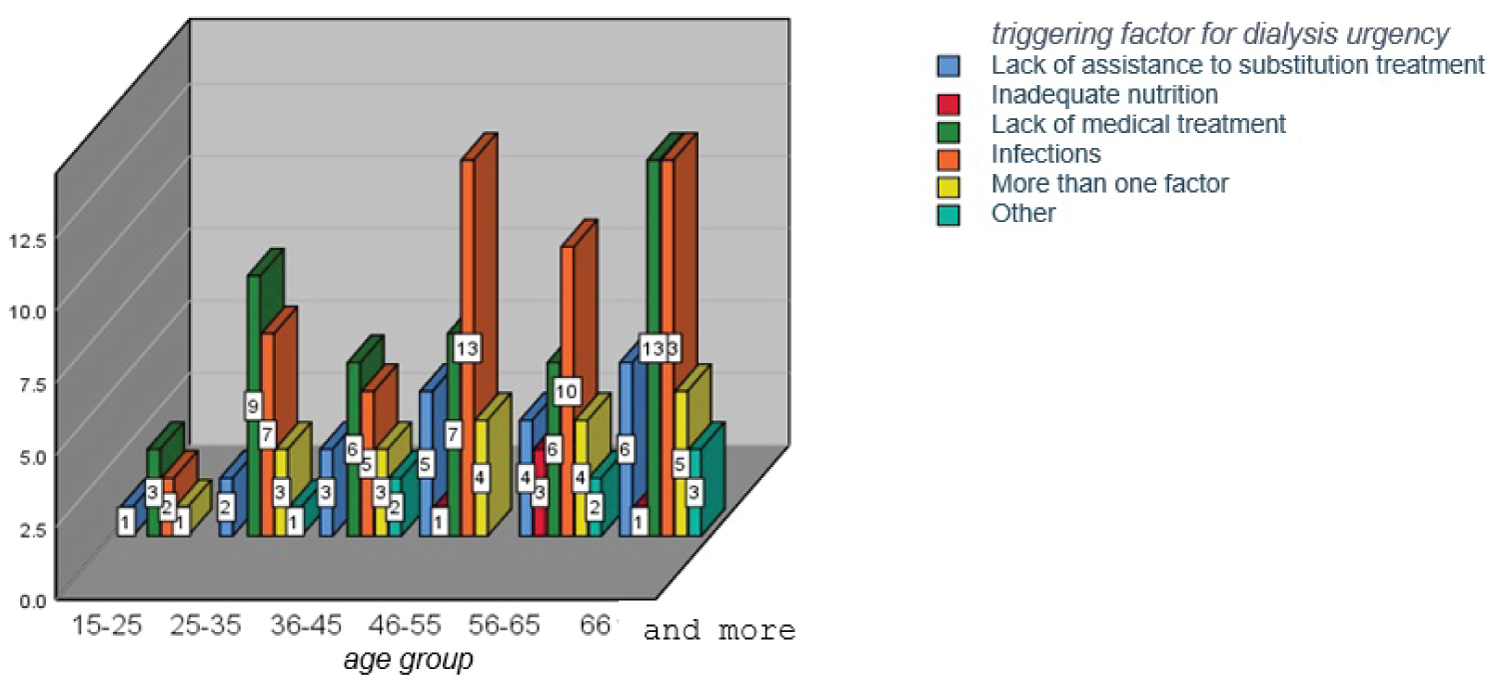 Graph 2: Triggering factor for dialysis urgency and age group.
View Graph 2
Graph 2: Triggering factor for dialysis urgency and age group.
View Graph 2
Table 1: Measures of central tendency of age. View Table 1
The most frequent cause of dialysis urgency in this study group was metabolic acidosis with a total of 43 patients (29.1%), followed by hyperkalemia with a total of 37 patients (25%), acute pulmonary edema with 25 patients (16.9%), uremic encephalopathy in 24 patients (16.2%) and the least frequent cause was hyperphosphatemia in 4 patients (2.7%), 15 patients presented more than one cause, corresponding to 10.1% of the total (Table 2).
Table 2: Frequency of dialysis emergencies. View Table 2
It was identified that the main factor that triggered dialysis urgency was the presence of infections in a total of 50 patients, which corresponds to 33.8% (Table 3), followed by the lack of medical treatment in 44 patients (29.7%), lack of attendance to substitutive treatment in 21 patients (14.2%), more than one factor was present in 20 patients (13.5%), other factors in 8 patients (5.4%) and 5 patients reported inadequate nutrition (3.4%).
Table 3: Factor that triggered the dialysis urgency. View Table 3
It was found that from 46 years of age onwards, the main factor that triggered dialysis urgency was infections (Table 4) and in the age group of 66 years and older, lack of medical treatment was added as the main associated cofactor (Graph 2). The association between age and the triggering factor was not significant, with a p = 0.965 (Table 5).
Table 4: Cross table age by groups and factors that triggered the urgency. View Table 4
Table 5: Chi-square tests for triggering factor of dialysis urgency and age group. View Table 5
It was identified that the main factor that triggers dialysis urgency was presented mostly in the male sex (Table 6), however, this association is not significant, finding a p = 0.655 (Table 7).
Table 6: Cross table SEX and factor that triggered the urgency. View Table 6
Table 7: Chi-square tests for sex and triggering factor for dialysis urgency. View Table 7
Regarding the association of gender with the type of dialysis emergency, no difference was found in the presence of the main emergency with male and female gender (Table 8), finding a non-significant association p = 0.294 (Table 9).
Table 8: Cross table of sex and type of dialysis emergency. View Table 8
Table 9: Chi-square test, sex and type of dialysis urgency. View Table 9
When observing the age with the type of dialysis urgency, it was identified that the age group of 46 to 55 years is more frequently associated with metabolic acidosis, finding a significant association p = 0.040 (Table 10).
Table 10: Chi-square test for age by groups and type of dialysis urgency. View Table 10
The main objective of this research protocol is to establish the most frequent cause of dialysis emergency and the main factor that precipitates it in patients with chronic kidney disease who come to the emergency department of the Hospital General de zone 50, in San Luis Potosi, Mexico. Chronic kidney disease affects 10% of the world population and 12.2% of the Mexican population. One of the most feared complications is that these patients are in dialysis emergency because mortality is 20% in the hospital setting and 50% in the intensive care unit, even if renal replacement treatment is performed. Therefore, it is important to know the most frequent cause and the main precipitating factor to offer the patient educational and preventive strategies, as well as early medical treatment in the emergency department. In our population, severe metabolic acidosis refractory to medical treatment was identified as the main cause of dialysis urgency, occurring in 29.1% and the main precipitating factor was the presence of infections at any level in 33.8%. RUIZ-MEJIA R, et al. (2017) conducted a retrospective cross-sectional descriptive study in Mexico City, entitled "treatment of hyperkalemia in patients with chronic kidney disease on dialysis therapy" in which he analyzed review and treatment articles, selected from PubMed Central, EBSCO, Medlineplus, SciELO and found that worldwide hyperkalemia has a prevalence of 42 to 50% in patients with chronic kidney disease , so it has positioned itself as the main cause of dialysis emergency and the main factor that precipitates it is the presence of infections [20]. Álvarez-Rodríguez E, et al. (2022) published an article resulting from the work of a group of experts representing three scientific societies involved in the management of hyperkalemia: the Spanish Society of Emergency Medicine (SEMES), the Spanish Society of Nephrology (SEN) and the Spanish Society of Cardiology (SEC) in which they refer that hyperkalemia has a frequency of 28% to 50% in patients with chronic kidney disease [21]. Gómez de la Torre-Del Carpio, Andrea, et al. (2018) conducted a retrospective cohort study in Lima, Peru entitled "Early mortality in patients with chronic kidney disease who started emergency haemodialysis in a Peruvian population: incidence and risk factors." In which they included 557 patients and identified that 59.6% entered emergency hemodialysis session due to mainly respiratory and urinary infections [22].
The results of our study differ with the publication of Ruiz-Mejia R, et al. (2017) and Alvarez-Rodriguez E, et al. (2022) since hyperkalemia as a dialysis emergency in our population comes in second place, presenting in 25% of patient's vs. 29. 1% with refractory metabolic acidosis, and this difference is mainly due to the fact that serum potassium levels can be decreased with medical treatment either by redistribution or elimination, apart from the fact that serum potassium levels are independent of presenting fatal electrocardiographic translation and this can be prevented by the administration of membrane stabilizers, In our hospital, since we have a large number of patients and the hemodialysis machines are saturated, patients with severe hyperkalemia are first stabilized with medical treatment before going on to urgent renal replacement therapy, as opposed to metabolic acidosis, where medical treatment is limited and has more adverse effects. The results of Gómez de la Torre-Del Carpio Andrea, et al. (2018) support the results of this research protocol, since the main factor precipitating dialysis urgency is the presence of infections, although the percentages vary 59.6% vs. 33.8% in our study, as expected, it can be said that in general this factor is the main factor and this is because it includes the presence of any type of infection, whether pulmonary, urinary, gastrointestinal, sepsis and angioaccess as main ones. In our study, there was no significant association of gender with the main dialysis emergency (p = 0.294). However, it was identified that there is a significant association (p = 0.040) with age, since the age group in which this complication occurs more frequently is from 46 to 55-years-old. Caravaca-Fontán Fernando, et al. (2020) conducted a retrospective study of longitudinal observation in a cohort with the title "Successful correction of metabolic acidosis is difficult to achieve in chronic kidney disease" which included 969 patients with chronic kidney disease and 55% presented metabolic acidosis of which 52.3% were men and the age of greatest presentation was from 51 to 79 years [23].
We did not find a significant association between gender and the main dialysis emergency in our study (p = 0.29), so we agree with Caravaca-Fontán, Fernando, et al. (2020) that there is no significant difference in the presence of this complication in men and women, so strategic and educational measures should be taken in all patients regardless of gender, however we do differ with the association of age and metabolic acidosis, since in our study this association was significant (p = 0.04) was more frequent in patients from 46 years of age, and in the study by Caravaca-Fontán, Fernando, et al. (2020) it was more frequent from 51 years of age, this is mainly due to the fact that renal function decreases each year and affects a higher percentage of older patients, with a significant association between age and the main cause of dialysis urgency.
One of the difficulties in carrying out this study is that it is retrospective, since on occasions the blood gas registry was not found, which limited the real report of acid-base alterations, which is why they were not included in this study. Another limitation is the questioning of non-pathological factors such as diet or amount of fluid intake in 24 hours, triggering the dialysis emergency, since they are not specified in the record, and could go unnoticed in this study. NEW PERSPECTIVES A prospective study considering dialysis urgency and triggering factors could broaden our knowledge on these issues. By finding infections as a predisposing factor for dialysis urgency, we could propose a study describing the most frequent sites of infection, as well as the pathological agent and bacterial resistance.
Knowing that refractory metabolic acidosis is the main dialysis emergency in our patients, it is important in the emergency department to perform blood gas analysis in all these patients to quickly identify this emergency and request timely renal replacement therapy to have a positive impact on the morbidity and mortality of these patients. The main factor that precipitates dialysis urgency is the presence of infection, so initiating timely treatment, as well as sanitary and preventive measures in all patients will have a positive impact on reducing the presence of infection. Since there is a significant association with a specific age group, it is necessary to provide educational and preventive strategies with greater emphasis on this age group (46 to 55 years).
To God, my parents, my son Albert Karim and my teachers.
The authors declare that they have no competing interest.
Alberto Ruiz Mondragon coordinated the working group. Karen Janeth Marroquin Morales and Alberto Ruiz Mondragon contributed to the literature analysis, update and revision of the article, and the approval of the final version.