Vasoplegic shock refractory to vasopressors is associated with significant morbidity and mortality. Catecholamine driven therapies are first-line in the management of vasoplegic shock. Research regarding the use of non-catecholamine agents in the setting of refractory vasoplegic shock is lacking. Methylene blue has multiple off-labelled indications for use, but recently has been suggested to have a role in treating vasoplegic shock. Vasoplegic shock is mediated by dysregulation of nitric oxide, which is generated via nitric oxide synthase. Methylene blue inhibits endothelial nitric oxide synthase and restores vascular tone through nitric oxide upregulation. Our case describes hemodynamic improvement following administration of a one-time dose of methylene blue in the management of refractory vasoplegic shock due to primidone overdose. Within 36 hours, he was titrated off all vasopressors with clinical improvement. This case report demonstrates the possible role of single-dose methylene blue in refractory vasoplegic shock.
Critical care, Intensive care, Lactic, Resuscitation, Shock, Vasopressors, Vasoplegic shock, Vasoplegia, Primidone, Methylene blue
Vasoplegia presents as abnormally low systemic vascular resistance in the presence of profound hypotension and normal or increased cardiac output [1]. Vasoplegic shock is associated with significant morbidity and mortality. There is limited data on non-catecholamine driven therapies in the setting of vasoplegic shock. Methylene blue restores vasoregulation by targeting the nitric oxide (NO) pathway. Limited data is available on the use of methylene blue in the setting of vasoplegic shock, but several small studies suggest a possible role to improve hemodynamics.
A 71-year-old Caucasian male with a significant past medical history of autonomic dysfunction, depression, diabetes mellitus, hypertension, hyperlipidemia and obstructive uropathy presented to the emergency department secondary to altered mental status. The initial physical exam was significant for severe hypotension and bradycardia (blood pressure at arrival was 48/26 mmHg, heart rate of 40 beats per minute, mean arterial pressure (MAP) of 31. Patient was unable to provide any history secondary to altered mental status and a lack of family listed in the electronic chart. Initial laboratory data was significant for electrolyte abnormalities (potassium of 3.6 mmol/L and magnesium of 1.7 mg/dL) which were replaced. A urine toxicology screen was performed and was positive for barbiturates and tetrahydrocannabinol (THC). Pertinent initial laboratory results are listed in Table 1. A home medication list was obtained through the patient’s prescription drug fill history. Home medications included: carvedilol 3.125 mg by mouth twice daily, clopidogrel 75 mg by mouth once daily, primidone 50 mg by mouth three times daily, sertraline 50 mg by mouth once daily, glimepiride 2 mg by mouth three times daily, atorvastatin 40 mg by mouth once daily, aspirin 81 mg by mouth once daily, and gabapentin 400 mg by mouth twice daily. He had no drug allergies reported. Although altered, the patient admitted to taking 40 pills of his home primidone.
Table 1: Initial laboratory workup. View Table 1
Initial management included fluid resuscitation (2.5 liters of lactated ringers were administered, followed by lactated ringers at 83 mL/hr) and one dose of atropine 1 mg IV push with no significant improvement in hemodynamics. Norepinephrine was started at 34 mcg/min and was titrated up to 60 mcg/min within 2 hours. Epinephrine was added at 1mcg/min and vasopressin at 0.03 units/min. Vasopressors were titrated per hospital protocol to a MAP of 65. Stress-dose steroids were initiated as 50 mg every 6 hours and administered immediately. The patient’s hemodynamics continued to decline and were not responsive to high-dose vasopressors. Patient’s laboratory work up, clinical status, and inability to respond to high dose vasopressors led to the thought process of refractory vasoplegic shock secondary to primidone toxicity. The patient was administered methylene blue 90 mg (1 mg/kg) intravenously once. Figure 1 illustrates the patient’s trend in vasopressor requirements with the mentioned interventions.
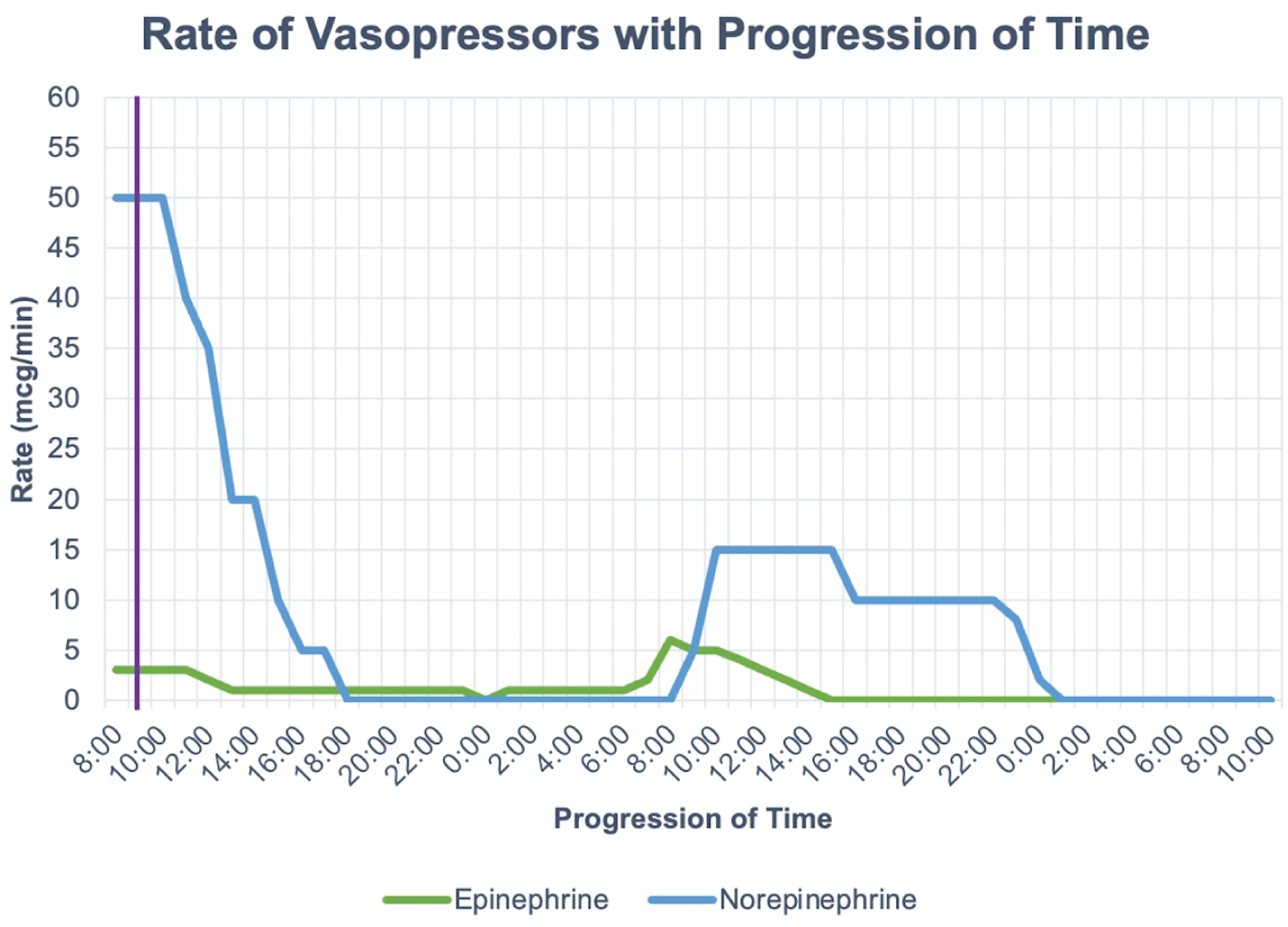 Figure 1: A graph of the rate of vasopressors (epinephrine and norepinephrine) with progression of time. The purple line depicts the time methylene blue was administered.
View Figure 1
Figure 1: A graph of the rate of vasopressors (epinephrine and norepinephrine) with progression of time. The purple line depicts the time methylene blue was administered.
View Figure 1
After administration of methylene blue, the patient’s hemodynamics improved. Vasopressor requirement decreased dramatically after administration, and all vasopressors were titrated off within 36 hours. The patient was transferred out of the ICU and discharged.
Vasoplegia presents as abnormally low systemic vascular resistance in the presence of profound hypotension and normal or increased cardiac output [1]. Causes for vasoplegia include, but are not limited to sepsis, cardiac and non-cardiac surgery, and drug intoxication. Vasoplegic shock is described as vasoplegia with evidence of tissue hypoperfusion. The presence of elevated lactate correlates with poor prognosis [2].
Catecholamines are considered first-line therapy in shock, with most data supporting use in septic shock. High doses of vasopressors can result in increased myocardial demand, dysrhythmias, and peripheral and organ ischemia. Adjunctive therapeutic options to reduce vasopressor requirements in shock include vasopressin, corticosteroids, midodrine, methylene blue, and angiotensin II [3]. Vasopressin and corticosteroids have a more evidence-based role in guidelines for the management of shock. Other agents such as methylene blue may also be considered in patients with increased vasopressor demand, although data regarding its place in therapy is limited. Larger studies are necessary to evaluate.
Nitric oxide (NO) is a critical factor for vascular function and increased vasodilation through multiple pathways. In shock, including vasoplegic shock, increased NO causes systemic vasodilation. NO is primarily generated from L-arginine primarily by endothelial nitric oxide synthase, which is mostly present in endothelial tissues, but also in platelets and cardiac myocytes. NO then diffuses into vascular smooth muscle cells to induce vasodilation. Nitric oxide increases cGMP which inhibits calcium into cells, leading to muscle relation. Hormonal and mechanical factors, such as inflammatory cytokines, bradykinin, and thrombin, increase NO production and vasodilation by activating endothelial NO. NO also activates ATP-sensitive potassium channels, leading to hyperpolarization and inhibited vasoconstriction [4].
Methylene blue (MB) has a labelled indication for acquired methemoglobinemia, in which it facilitates the conversion of methemoglobin to haemoglobin. There are reports of off-label use in life-threatening conditions such as septic shock, anaphylactic shock, drug-induced shock, and vasoplegia after cardiac surgery, in which MB improves hemodynamics and decreases vasopressor requirements [5-10]. Medications involved in cases of drug-induced shock include amlodipine, atenolol, and valsartan. Although most cases in which it was administered in non-septic shock are case reports and case studies, methylene blue has demonstrated positive patient outcomes in terms of mortality and vasopressor requirement. A recent randomized control trial demonstrated early adjunctive methylene blue in patients with septic shock reduced time to vasopressor discontinuation and increased vasopressor free days at 28 days [11]. To our knowledge, there are no reports of using methylene blue in the setting of vasoplegic shock secondary primidone overdose.
MB is an inhibitor of nitric oxide synthase and guanylate cyclase and restores systemic vasoregulation through direct nitric oxide upregulation [6]. The proposed mechanism of action involves inhibiting epithelial NO synthase to reduce vasodilation and improve hemodynamics and reduce vasopressor requirements [12]. After administering intravenous fluids and vasopressor therapies, targeting the nitric oxide pathway may be a reasonable alternative to avoid post-shock complications. When given intravenously, MB has an onset of action of 30-60 minutes, with a terminal half-life of 5-6 hours. Studies have evaluated prolonged infusion of MB due to its short duration of action [7,13,14]. In cases of vasodilatory shock, literature supports administering MB as a bolus 1-2 mg/kg over 10-20 minutes [5,12,15].
The side effect profile of MB is dose-related, and adverse effects are rarely present in one-time doses under 2 mg/kg. The most common adverse effect of MB is blue/green discoloration of urine. It is contraindicated in patients with glucose-6-phosphate dehydrogenase deficiency due to hemolytic anemia and is pregnancy category X rating. MB should be avoided in patients taking any drug with serotonergic activity such as selective serotonin reuptake inhibitors due to the risk of serotonin syndrome. MB reduces renal blood flow and should be used in caution in patients with renal failure [6].
Our patient presented in vasoplegic shock secondary to primidone overdose. Primidone is a first-generation barbiturate type antiepileptic medication used most to treat partial and generalized seizures. Primidone is a unique medication in that it undergoes metabolism into two active metabolites, phenobarbital and phenylethylmalonamide. Both primidone and its active metabolites are thought to have antiepileptic properties. Its exact mechanism of action is unknown, but it is thought to bind centrally with voltage-gated sodium channels and inhibits the monotonous firing of action potentials as well as activate gamma-aminobutyric acid receptor complex causing hyperpolarization within neurons. A primidone overdose presents with signs of severe CNS depression which can include altered mental status, hypotension leading to shock, cyanosis, respiratory depression, and coma. Morbidity and mortality of a primidone overdose are high if untreated. Supportive treatment is the only course of action for a primidone overdose, there is no reversal agent or antidote. In severe overdoses, the patient may need respiratory support such as mechanical ventilation as well as hemodynamic support such as fluid boluses and vasopressors. Tactics to remove the primidone from the body such as activated charcoal, urine alkalinization, diuretics and hemodialysis are often deployed [16-19].
Our patient required extensive hemodynamic support including fluid boluses, vasopressors, and corticosteroids secondary to a primidone overdose. A one-time dose of methylene blue was administered within 12 hours of vasopressor initiation in efforts to decrease his vasopressor requirement. There is a lack of data on non-catecholamine therapies for vasoplegic shock, especially in the setting of primidone overdose. This case describes hemodynamic improvement after administration of a one-time dose of methylene blue in refractory vasoplegic shock secondary to primidone toxicity.
Vasoplegic shock not responsive to high-dose vasopressors is associated with high mortality. There is a lack of literature on the use of non-catecholamine therapies, such as methylene blue, in vasoplegic shock. We describe a case of vasoplegic shock secondary to primidone toxicity, in which vasopressor requirements dramatically decreased following a one-time dose of methylene blue, and the patient was later discharged to home. More studies are needed to evaluate methylene’s blue place in therapy when treating patients with vasoplegic shock.
We would like to thank the patient who entrusted us to be part of his case and permitted us to share his case.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Our institution does not require ethical approval for reporting individual cases or case series.
Written informed consent was obtained from the patient for his anonymized information to be published in this article.