Angioedema, Airway obstruction, Emergency airway management, Percutaneous tracheostomy
Angioedema evaluation and management should focus on the airway initially because the main concern in the patient in angioedema is airway obstruction. Indeed, airway obstruction can occur in up to 15% of patients with angioedema [1,2]. Angioedema in the emergency department is a common presentation and the threat of asphyxiation can be fatal, therefore, prompt diagnosis and correct treatment are critical.
A woman ages 70-80 years-old with a past medical history of obesity, hypertension and dyslipidemia and outpatient therapy with amlodipine/valsartan, diltiazem, naproxen, and simvastatin. The patient was admitted to the emergency department with sudden onset tongue swelling and inability to swallow Figure 1, but no other associated complaints, no recent initiation of outpatient therapy and there was no history of drug or food allergies, upper respiratory tract infection, or recent tooth extraction. On examination, she was afebrile with normal vital signs. Soft inspiratory stridor was present, and the voice was very weak. Oral hygiene was fair, with no peritonsillar fullness or raised floor of the mouth. Other review of systems was normal. In the resuscitation bay, initial blood gas revealed hypoxia while the rest of the parameters were unremarkable.
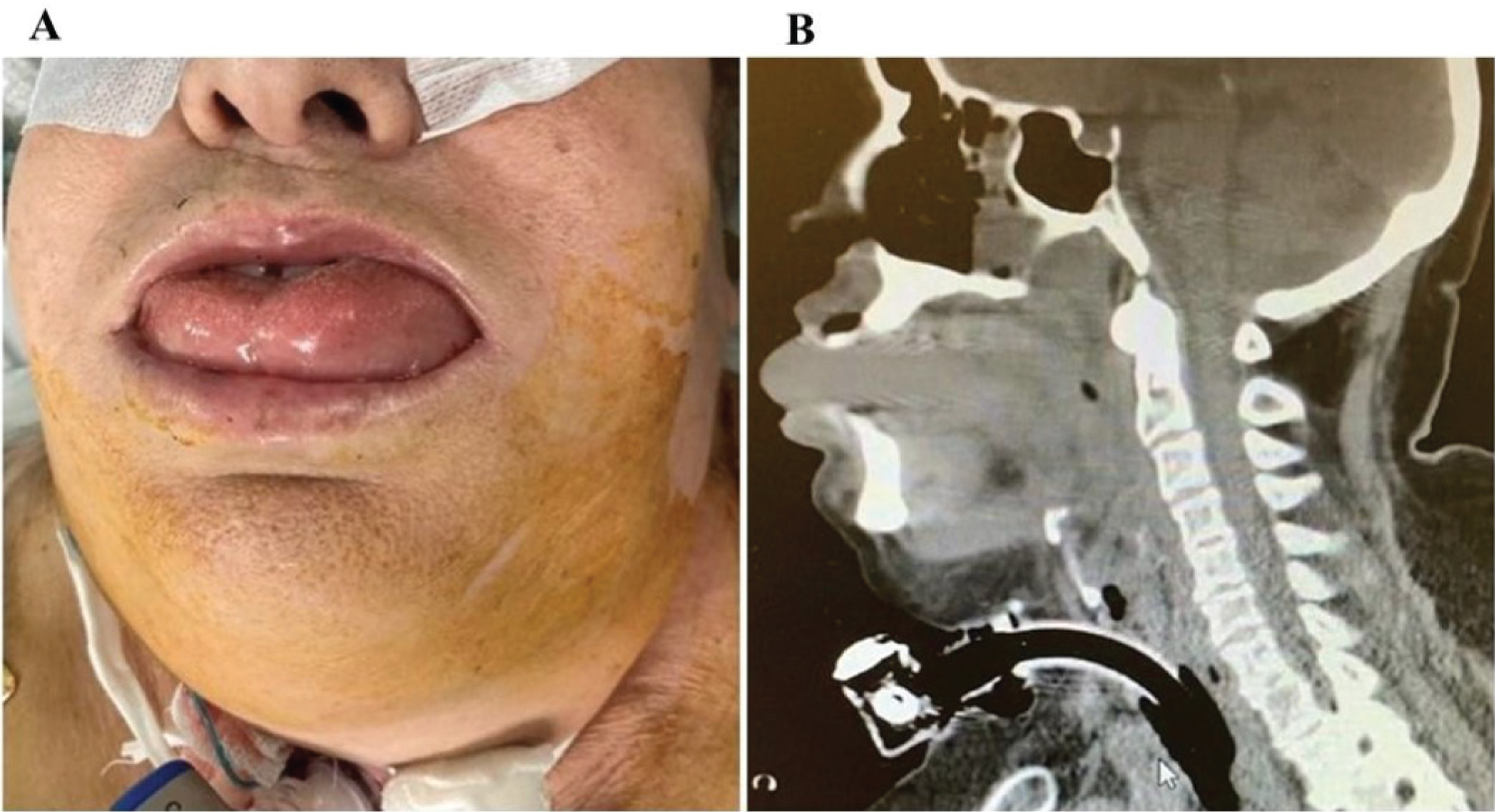 Figure 1: (A) Tongue swelling with evolution to airway obstruction; (B) CT images revealed significant oedema of all the soft parts of the nasopharynx, oropharynx, lingula and base of tongue, with complete obliteration.
View Figure 1
Figure 1: (A) Tongue swelling with evolution to airway obstruction; (B) CT images revealed significant oedema of all the soft parts of the nasopharynx, oropharynx, lingula and base of tongue, with complete obliteration.
View Figure 1
During the admission, she was medicated with targeted therapy due to suspicion of anaphylaxis, with no improvement and progressive worsening of the tongue swelling and inspiratory stridor with evolution to airway obstruction, despite hemodynamic stability and no neurological dysfunction. Approached by intensive care medicine with a decision for endotracheal intubation due to the obstructed airway. Algorithm for difficult airway management was performed and airway equipment available. Thus, after manual ventilation using a bag valve-mask to preparation for tracheal intubation and optimize oxygenation status it was decide upon proceeding with rapid sequence intubation medications (fentanyl, propofol and rocuronium) and approach of the airway with videolaryngoscopy, showing exuberant oedema of the glottis, without visualization of cords, with an unsuccessful attempt at endotracheal intubation. Following a rescue oxygenation with a supraglottic airway device was attempted (laryngeal mask airway) which allowed ventilation with high resistance by a manual ventilation but, able to effectively oxygenate the patient. In this emergency setting it was decided an achieving front-of-neck access with performed a percutaneous tracheostomy under sedation with ketamine and propofol. The procedure was successful and adequately oxygenate and ventilate the patient.
Subsequently, a cervical contrast CT images revealed significant oedema of all the soft parts of the nasopharynx, oropharynx, lingula and base of tongue, tonsillar regions, and retropharyngeal region with complete obliteration of the air column due to a volumetric increase of the soft tissues at this level Figure 1, which was difficult to characterize, but without evidence of abscesses or tumor masses.
Discussion with otolaryngology and maxillofacial surgery without indication for other immediate measures. Patient was admitted to intensive care unit with a presumptive diagnosis of sudden angioedema of etiology under study. Patient presented favorable evolution during the ICU stay, showing significant regression of the angioedema at 48 hours Figure 2, which allowed the withdrawal of sedation and ventilatory support with remove of tracheotomy four days after the hospital admission. Due to inconclusive diagnosis at the discharge, patient keeps followed-up in immunologist consultation.
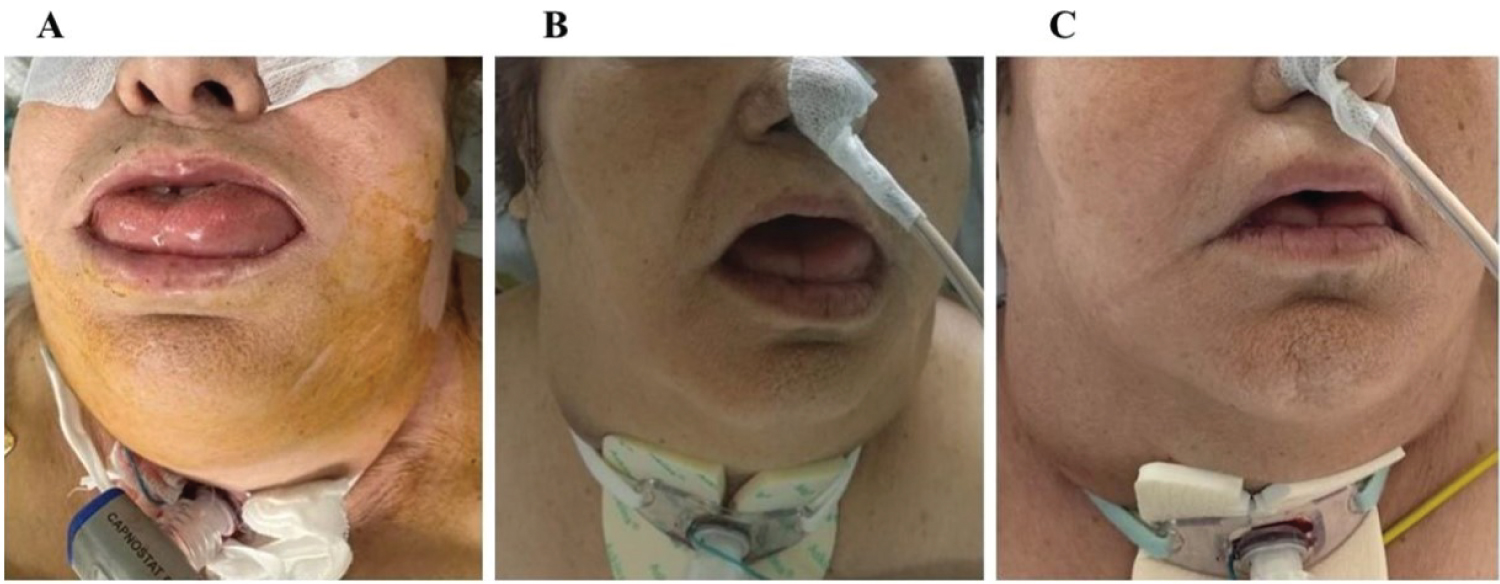 Figure 2: (A) Day one; (B) Twenty-four hours later tongue edema appears in regression; (C) Forty-eight hours later tongue edema resolution.
View Figure 2
Figure 2: (A) Day one; (B) Twenty-four hours later tongue edema appears in regression; (C) Forty-eight hours later tongue edema resolution.
View Figure 2
Angioedema is defined as the abrupt onset of swelling of the lips, tongue, posterior pharynx, and most dangerously the larynx [3]. Angioedema may occur in isolation, accompanied by urticaria, or as a component of anaphylaxis [3,4]. The underlying pathophysiology is mediated by several mechanisms, including histamine and bradykinin and influences the clinical presentation and treatment recommendations. Generally, may be diagnosed based on a suggestive history and physical findings [5]. It develops within minutes to hours and resolves in hours to days [3,5]. Usually, routine laboratories are normal in many cases of angioedema [4].
Around 10% of cases it can be life-threatening when severe angioedema of the larynx, upper airway, or tongue results in airway obstruction [4]. In this case it is necessary a rapid assessment of airway patency and respiratory status to identify those who need emergency airway management [6]. About predicting difficulty of endotracheal intubation in critically ill adults it can be used the MACOCHA score [7]. It is the only tool has been validated and consists of seven independent predictors in three domains (Mallampati score III/IV, Obstructive sleep apnoea syndrome, reduced mobility of cervical spine, limited mouth opening, coma, severe hypoxia, nonanesthesiologist) [6-8]. A MACOCHA score ≥ 3 predicts difficult intubation in the critically ill (the score ranges from 0 - anticipated easy to 12 - anticipated very difficult) [7,8]. Thus, airway protection must be given over a comprehensive diagnostic evaluation and if an emergent definitive airway is required, literature suggests a high rate of cricothyrotomy or tracheostomy (up to 50% of cases) [9-11]. Patients in whom an emergent tracheostomy is indicated include patients with acute upper airway obstruction who failed intubation with an endotracheal tube or in whom an endotracheal tube cannot be placed (eg, angioedema, anaphylaxis, hematoma, retropharyngeal abscess, malignant or benign tumors, or foreign body that cannot be removed) [10,11]. Although it can be argued that emergency cricothyrotomy should be performed in this population, emergency tracheostomy is an alternative in the hands of an experienced operator [11].
Given the life-threatening potential of patients presenting with angioedema, each emergency department should have an established protocol or algorithm and training staff to recognize, differentiate, and manage angioedema to ensure appropriate asses and security the patients airway.
All the authors made a substantial contribution to the manuscript.
The authors have no potential conflicts to disclose.