Securing a peripheral venous line is one of the most common procedures used in hospital settings. Although this is an easier task and a routine exercise, if not done properly, it can have dire consequences. This case report revolves around a 40-year-old man admitted to a super-specialty unit of a tertiary care hospital, while removing a venous catheter, was locally examined for a retained fragment of a peripheral venous catheter when the attending nurse noticed his absent tail. The missing fragment was identified in the cephalic vein of the left arm by ultrasonography. Immediately after imaging, the patient was transferred to an emergency operating room, where the retained fragment was extracted under local anaesthesia by performing a venotomy under the supervision of a vascular surgeon.
Such routine procedures form an important part of the health care delivery system, and as such, there are no specific guidelines for the performance of these procedures. Ultimately, due to a lack of knowledge and awareness of the methodologies regarding these procedures among junior hospital staff, accidents may occur. This case is an ideal example of the factors and unavoidable circumstances leading to a peripheral venous catheter fracture and how such unfortunate events can be prevented.
Through this case, the authors tries to convey the importance of the guide needle in cannulation and how its repeated reinsertion after multiple failed cannulation attempts can lead to such consequences. And proper counselling, awareness, and education of junior hospital staff, including patients and their caretakers, about these rare but devastating consequences of such routine procedures.
Venotomy, Day care procedure, Cephalic vein, Peripheral intravenous catheter, Iatrogenic complication
Securing a peripheral venous line is the first and simplest routine task performed after admission to the hospital setting. Although it is a simpler task, it can be associated with many complications, such as swelling and inflammation around the injection site, injury to adjacent vessels and nerves, hematoma formation after puncture, extravascular infiltration (if the peripheral intravenous cannula is not properly secured), thrombophlebitis, cellulitis, and sepsis during long-term storage, and, in rare cases, embolism [1]. Peripheral intravenous catheter or cannula (PIVC) fracture is an underreported complication of peripheral intravenous (PIV) cannula insertion [2].
These life-threatening accidents related to the same procedure due to iatrogenic or unavoidable circumstances have been rarely reported [3]. And especially in the Indian scenario, there are no case reports available in this context. Through this case, the author tries to convey the importance of the guide needle piercing the catheter during cannulation after several failed attempts. including proper advice, awareness, and education about such routine procedures and how such accidents can be prevented.
A 40-year-old man admitted to the tertiary care wing of a tertiary care hospital on September 2022 was examined locally for a peripheral venous catheter that was in place when the attending nurse removed the venous catheter, noting its absent tail. As soon as she saw this, she called the resident on duty. The patient had stable vitals, but on local examination there were no signs of inflammation, and on palpation, induration was felt in the left cubital fossa.
A tourniquet was tied on the most proximal area of the same arm to prevent the broken part or the tail from reaching other important areas. A missing fragment was detected in the cephalic vein of the left arm during ultrasound. The patient was then transferred to an emergency operating theatre, where the rest of the peripheral venous catheter was removed under local anaesthesia under the supervision of a vascular surgeon. A 1.5 centimeter extracted out tail or part of the peripheral venous catheter as shown in Figure 1. It was removed after the local exploration and venotomy.
 Figure 1: A 1.5 cm long fractured fragment/tail of the venous catheter after doing local exploration and venotomy.
View Figure 1
Figure 1: A 1.5 cm long fractured fragment/tail of the venous catheter after doing local exploration and venotomy.
View Figure 1
Thereafter, the suspected local site was explored as seen in Figure 2 , the explored local site was sutured, using interrupted suturing techniques for wound closure under aseptic conditions, as shown in Figure 3 . The patient was kept under observation for 2 more days and was subsequently discharged from the hospital when the course of the hospital stay was uneventful.
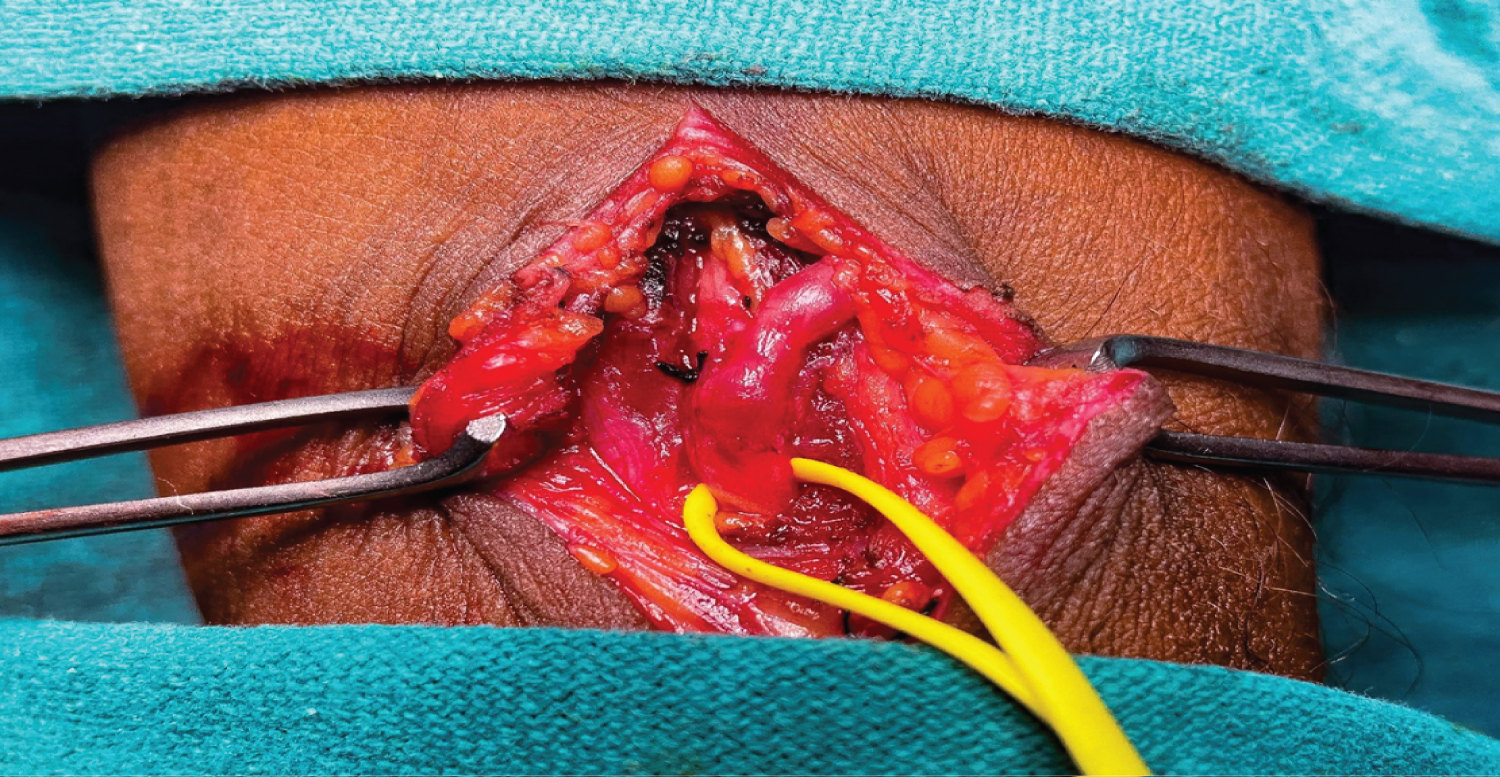 Figure 2: An intraoperative picture showing exploration of the local site i.e., the cephalic vein where the fractured segment of the catheter was retained.
View Figure 2
Figure 2: An intraoperative picture showing exploration of the local site i.e., the cephalic vein where the fractured segment of the catheter was retained.
View Figure 2
 Figure 3: Suturing of the local incision site is done after the extraction and removal of the fractured catheter tail or fragment in situ.
View Figure 3
Figure 3: Suturing of the local incision site is done after the extraction and removal of the fractured catheter tail or fragment in situ.
View Figure 3
Such routine procedures form an important part of the health care delivery system, and as such, there are no specific guidelines regarding these procedures. Due to a lack of knowledge of the methodologies regarding these procedures among junior hospital staff, such accidents may occur during cannula placement or removal [4]. Other associated causes may include poor cannulation techniques by novices performing such procedures without supervision, poor-quality cannula and catheters, repeated insertion of the guide needle after repeated unsuccessful attempts, or a cannula that has not been replaced for a long time in chronically ill patients [5].
Realising that multiple unsuccessful attempts using the same cannula are to be very strongly discouraged, such procedures should be performed under the supervision of senior hospital staff, and, in an emergency, if junior hospital staff are unable to secure the peripheral device line or if they notice such inconsistencies in the size of the cannula when removing it, the help of the experts should be taken, as seen in this case. This case emphasises safer cannulation practises by clinicians and adequate patient counselling about the rare consequences of such routine procedures.
Initially, the same patient had to undergo an X-ray, then ultrasonography, and then local exploration and venotomy in the operating room, which increased the hospital length of stay and hence costs. Conversely, if the same broken fragment remained somewhere else in the body, the same patient would undergo a much more expensive CT scan and emergency surgery, which, in rare cases, could include a thoracotomy.
The primary cause of venous catheter fracture is repeated reinsertion of the guidewire during multiple failed attempts to secure a peripheral line, which punctures the tip of the catheter and goes unnoticed. Such practices should be very seriously discouraged, and a new catheter should be used if the tail of the catheter is punctured before it is inserted into a blood vessel. Other causes may include prolonged catheter insertion, and in such circumstances, the IV catheter should be changed regularly to avoid these life-threatening consequences. To avoid such accidents, multiple attempts at cannulation should be discouraged, and both patients and junior hospital staff should be well aware of the devastating consequences of such routine and not-so-simple procedures.
Taking this case into account, such accidents, whether iatrogenic or caused by other unavoidable circumstances, lead to additional costs and prolonged hospital stays that are easily avoidable. It is very important to adhere to the strict protocols and methodologies used in these daily routine procedures, as inefficiency or carelessness in performing such procedures, unsupervised can have devastating consequences for the patient. However, the occurrence of this or other treatment errors is unavoidable. Therefore, in addition to recommending safety points in the implementation of procedures, medical personnel should be trained to report cases immediately without fear of punishment and blame from superiors in case of incidents like this, so that the following dangerous consequences are avoided and the lives of patients are not endangered.
All the authors are grateful to the patient and his family members for their cooperation. Dr. Aditya Sharma is the primary and corresponding author of this article who drafted this manuscript. Dr. Rajeshwar Yadav and Dr. Swati Pathak read, edited, and made substantial contributions to the conception, design of the work, and the acquisition, analysis, and interpretation of data for the work and approved the final manuscript for publication. And the primary author hereby submits this manuscript under their supervision.
Consent was obtained or waived by all participants in this study.
In compliance with the ICMJE uniform disclosure form, all authors declare the following:
Payment/services info : All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships : All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships : All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.