Introduction: Systemic air embolism (SAE) is a rare but potentially life-threatening complication of transthoracic computed tomography (CT)-guided lung biopsy [1-6], with reported incidence rates of 0.02-0.07% to 0.21-4.8% [3,5,7,8]. However, the incidence might be underestimated due to failure to diagnose this adverse event in asymptomatic patients as its early recognition is difficult [2,3,5,6,9,10]. Although SAE may be well tolerated, it can be difficult to manage and may lead to death, with a mortality incidence of 0.16% [4,7].
Case presentation: We present the case of an asymptomatic 74-year-old man who presented with systemic air embolism after transthoracic CT-guided lung biopsy was performed [1,2,4-6]. Subsequent serial thoracic CT scans demonstrated the causal relationship as well as confirmed the gradual absorption of the intravascular air, showing total resolution of this clinical situation [1,2].
Conclusions: SAE is a rare and potentially fatal complication of transthoracic CT-guided lung biopsy that may be asymptomatic [1,3,5-7]. Post-procedure CT scans allow the detection of SAE [2,3,6,7,10]. Early recognition and prompt diagnosis are difficult but crucial and eventually lifesaving, preventing significant morbidity and mortality [1,3,4,6,7].
Systemic air embolism, Lung nodule, Transthoracic computed tomography (CT) -guided lung biopsy, Complication
Pulmonary nodules are a real challenge to daily medical practice [10]. Transthoracic CT-guided lung biopsy is a resourceful and widely used tool for the definitive diagnosis of pulmonary lesions, avoiding costly and unnecessary surgeries [1,3,4,9,10].
Transthoracic CT-guided lung biopsy can lead to complications that include pneumothorax (the most common), pulmonary hemorrhage, hemothorax, hemoptysis and SAE [1,4-7]. SAE consists of a very rare and potentially fatal lung biopsy complication, with reported incidence rates of 0.02-0.07% to 0.21-4.8% that can be associated with major morbidity and mortality [3,7-11]. However, these rates could be underestimated due to failure to diagnose this adverse event in asymptomatic patients [2,3,5,6,9,10].
SAE can result from three mechanisms: An accidental puncture of the pulmonary vein by the tip of the biopsy needle that can lead to air embolism occurring during rapid inspiration when atmospheric pressure exceeds pulmonary venous pressure (PVP) that is normally low (10 cmH2O); an accidental bronchovenous fistula that occurs when the needle simultaneously transverses both a pulmonary vein and adjacent airway, and if the alveolar pressure is greater than the PVP, air can enter the pulmonary vein; and transversing the pulmonary microvasculature as air can reach the pulmonary venous circulation if it enters the pulmonary arterial system [2,3,7,8,10].
SAE can be classified as venous or arterial according to the mechanism of gas entry into the bloodstream and the location of the gas emboli [3,6,8]. Systemic arterial air embolism is more worrisome than venous one, corresponding to air entry into the pulmonary venous system, reaching the systemic circulation [6,8].
In fact, SAE can result from an incidental passage of air from the pulmonary vein to the left heart that can lead to coronary and brain infarction [1,3,4,6,7].
Initial management consists of immediate administration of 100% oxygen and placing the patient in a slight Trendelenburg position to prevent air embolization into the cerebral circulation [2-8]. Early hyperbaric oxygen chamber therapy (HBOT) can be considered the mainstay treatment of SAE [2,5-8].
We present a case of SAE after transthoracic CT-guided lung biopsy was performed in an asymptomatic patient.
A 74-year-old man with a suspicious pulmonary nodule in the upper lobe of the right lung detected in thoracic CT Figure 1A and Figure 1B, was hospitalized and submitted to a pulmonary nodule biopsy with previous negative cytology for malignant cells. His past medical history included prostate cancer diagnosed 12 years ago, with lymph node metastasis, refractory to radiotherapy, under hormone therapy for 7 years; hepatocellular carcinoma and hepatic cirrhosis, with a Child-Pugh class A - 6 points and a Model for End-Stage Liver Disease (MELD) score of 10 points.
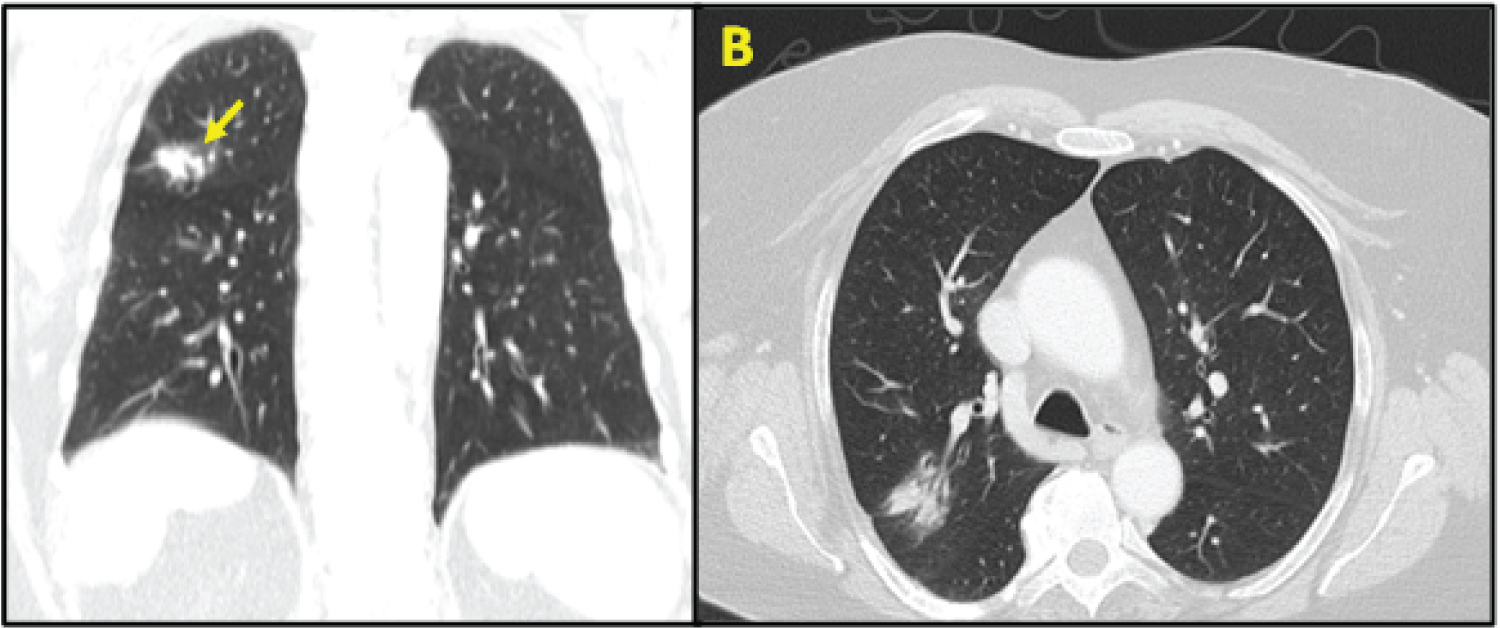 Figure 1: Prior to the procedure, CT thoracic scans was performed to establish an appropriate needle trajectory, with the nodule of interest being located on right upper lobe (yellow arrow; A - Coronal scan; B - Axial scan).
View Figure 1
Figure 1: Prior to the procedure, CT thoracic scans was performed to establish an appropriate needle trajectory, with the nodule of interest being located on right upper lobe (yellow arrow; A - Coronal scan; B - Axial scan).
View Figure 1
Given that the lung lesion on thoracic CT scan was very suggestive of malignancy cells, a new biopsy was performed after 1 month. This procedure was interrupted due to right iatrogenic pneumothorax, which was responsible for extension of hospitalization. He was discharged home after 2 days with an indication to repeat the biopsy 1 week later. Informed consent was obtained before performing the procedure. He underwent transthoracic CT-guided lung biopsy. Local anaesthetic agent was infiltrated at the skin site, followed by introduction of a coaxial biopsy system with a 20-gauge introducer needle and a 21-gauge core biopsy needle (length 16 cm; Argon Medical Devices, United States) into the upper lobe of the right lung lesion during lung biopsy, in an angulated left lateral decubitus position.
A single specimen was obtained and sent to the pathological anatomy department. The extraction procedure was performed once. Needle placement was assessed with additional CT images Figure 2. The introducer needle was then removed. The patient remained cooperative during the procedure without any coughing or deep breathing so no sedation was applied. His vital signs remained stable.
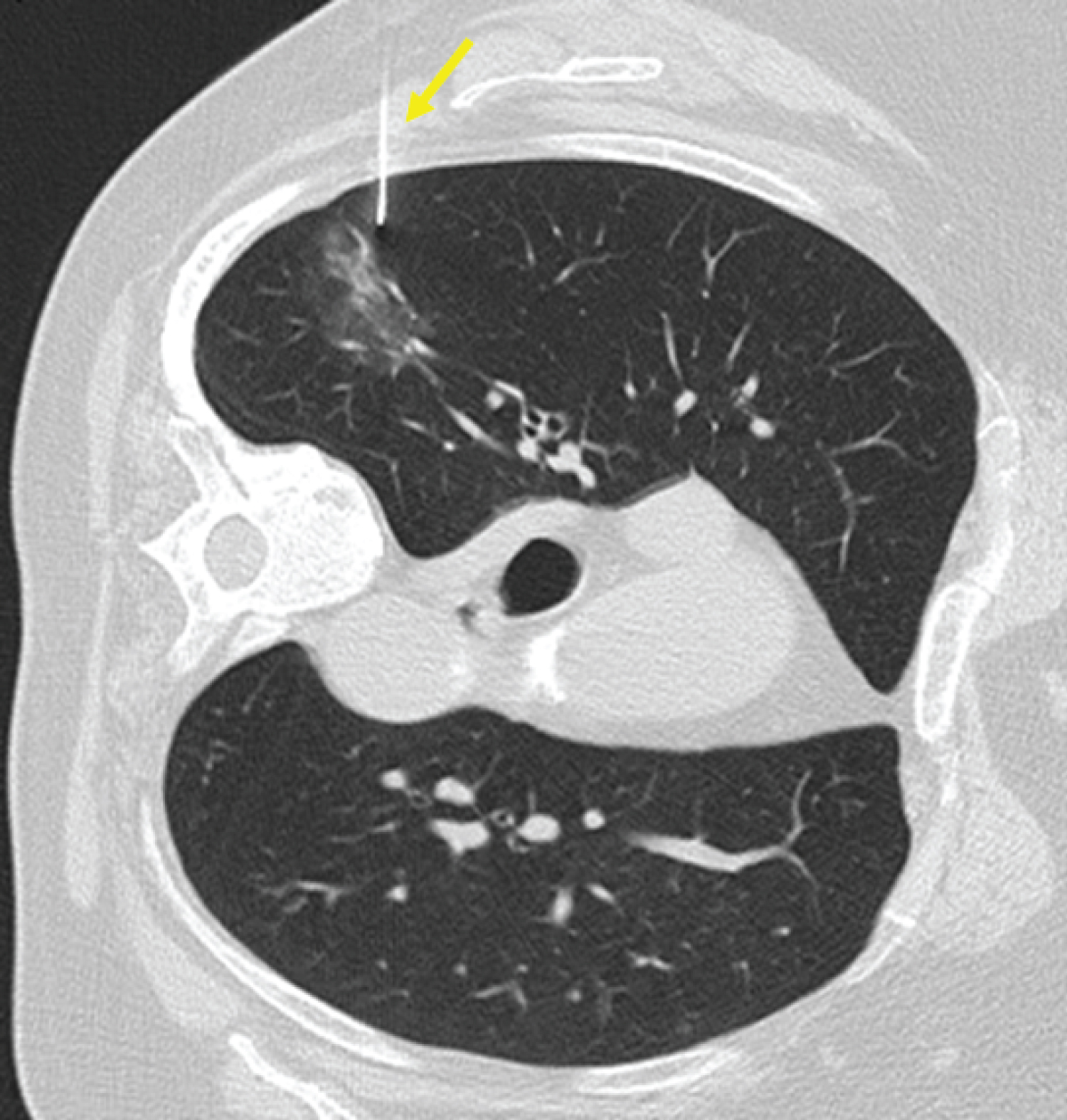 Figure 2: Axial thoracic CT scan showing the co-axial 20-gauge needle of a core biopsy instrument insertion through the nodule (yellow arrow).
View Figure 2
Figure 2: Axial thoracic CT scan showing the co-axial 20-gauge needle of a core biopsy instrument insertion through the nodule (yellow arrow).
View Figure 2
After the procedure, he presented 1 episode of hemoptoic sputum. A CT scan was performed immediately after procedure, in left lateral decubitus position, which detected the presence of air embolism in the left superior pulmonary veins, left atrium, aorta, and right kidney (Figure 3 and Figure 4 (A-D)); as well as a small pneumothorax and alveolar hemorrhage adjacent to the biopsied nodule (Figure 5).
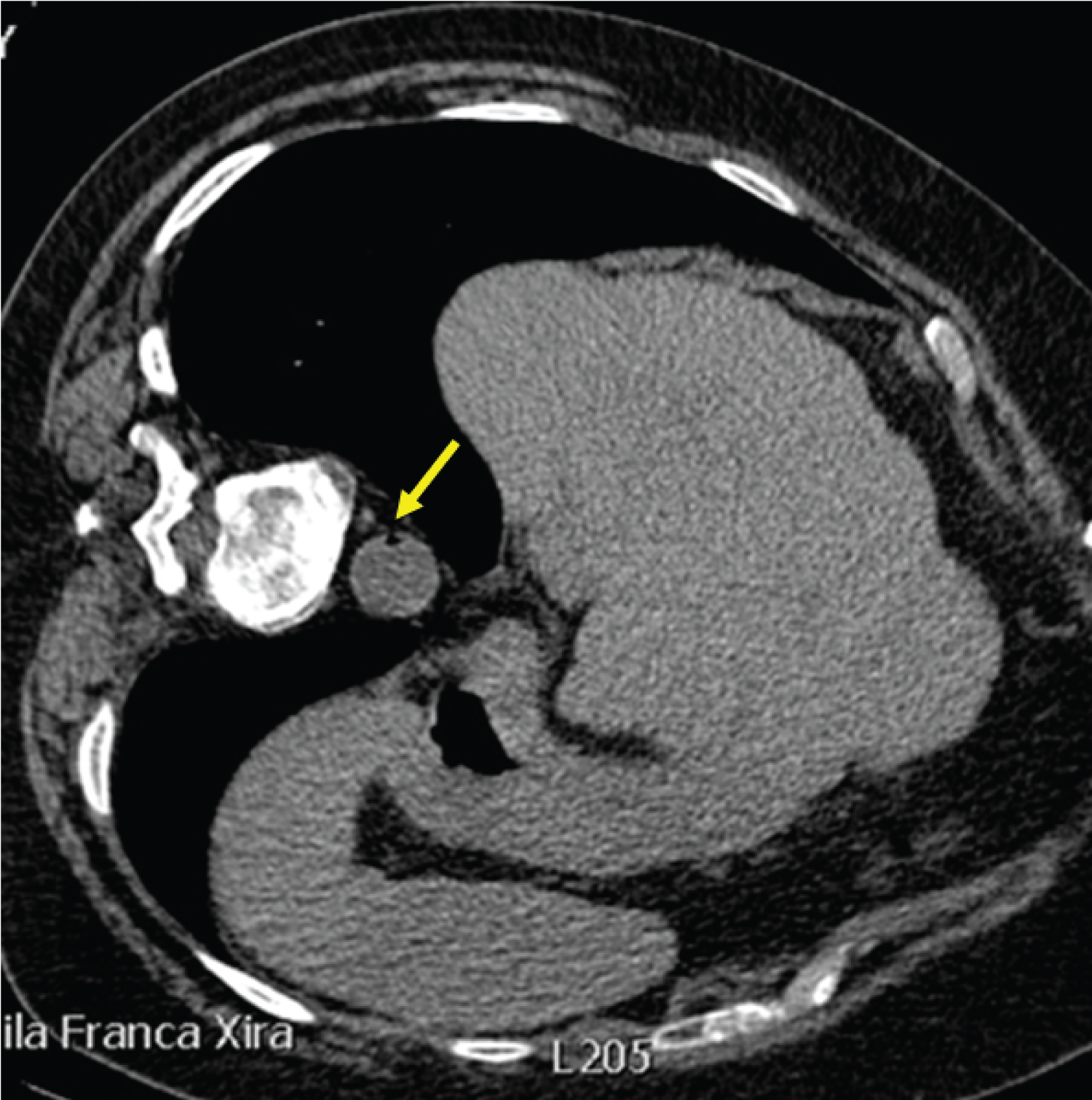 Figure 3: Axial CT scan showing an air embolus within the aorta, after biopsy (yellow arrow).
View Figure 3
Figure 3: Axial CT scan showing an air embolus within the aorta, after biopsy (yellow arrow).
View Figure 3
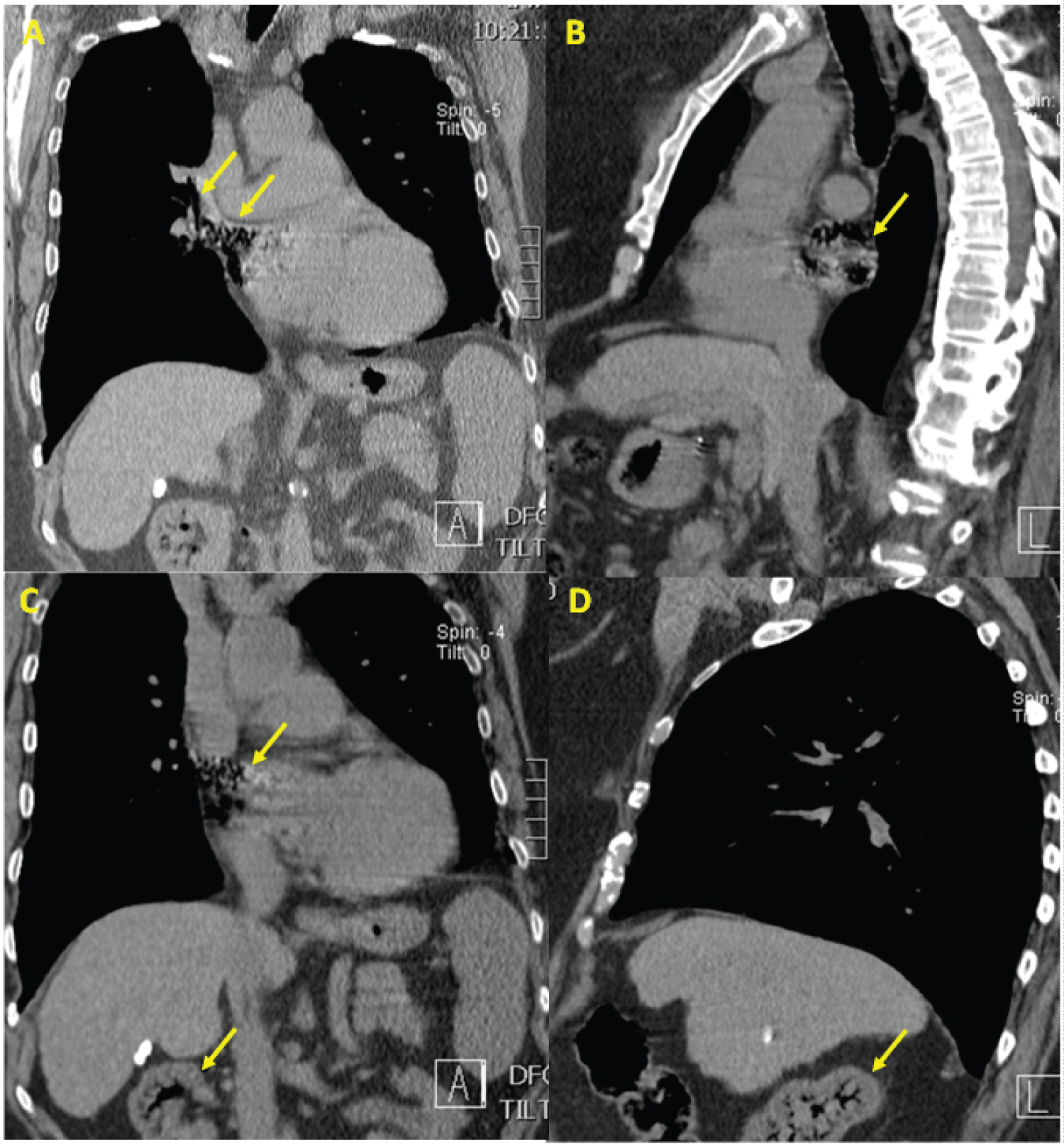 Figure 4: Series of CT scans demonstrating the movement of the air emboli. Immediate post-procedure tomography scans demonstrating free air in one of the left superior pulmonary veins and left atrium (A - coronal scan); left atrium (B - sagittal scan); left atrium and right kidney (C - coronal scan) and the arterial vasculature of the right kidney (D - sagittal scan), evidenced by yellow arrows.
View Figure 4
Figure 4: Series of CT scans demonstrating the movement of the air emboli. Immediate post-procedure tomography scans demonstrating free air in one of the left superior pulmonary veins and left atrium (A - coronal scan); left atrium (B - sagittal scan); left atrium and right kidney (C - coronal scan) and the arterial vasculature of the right kidney (D - sagittal scan), evidenced by yellow arrows.
View Figure 4
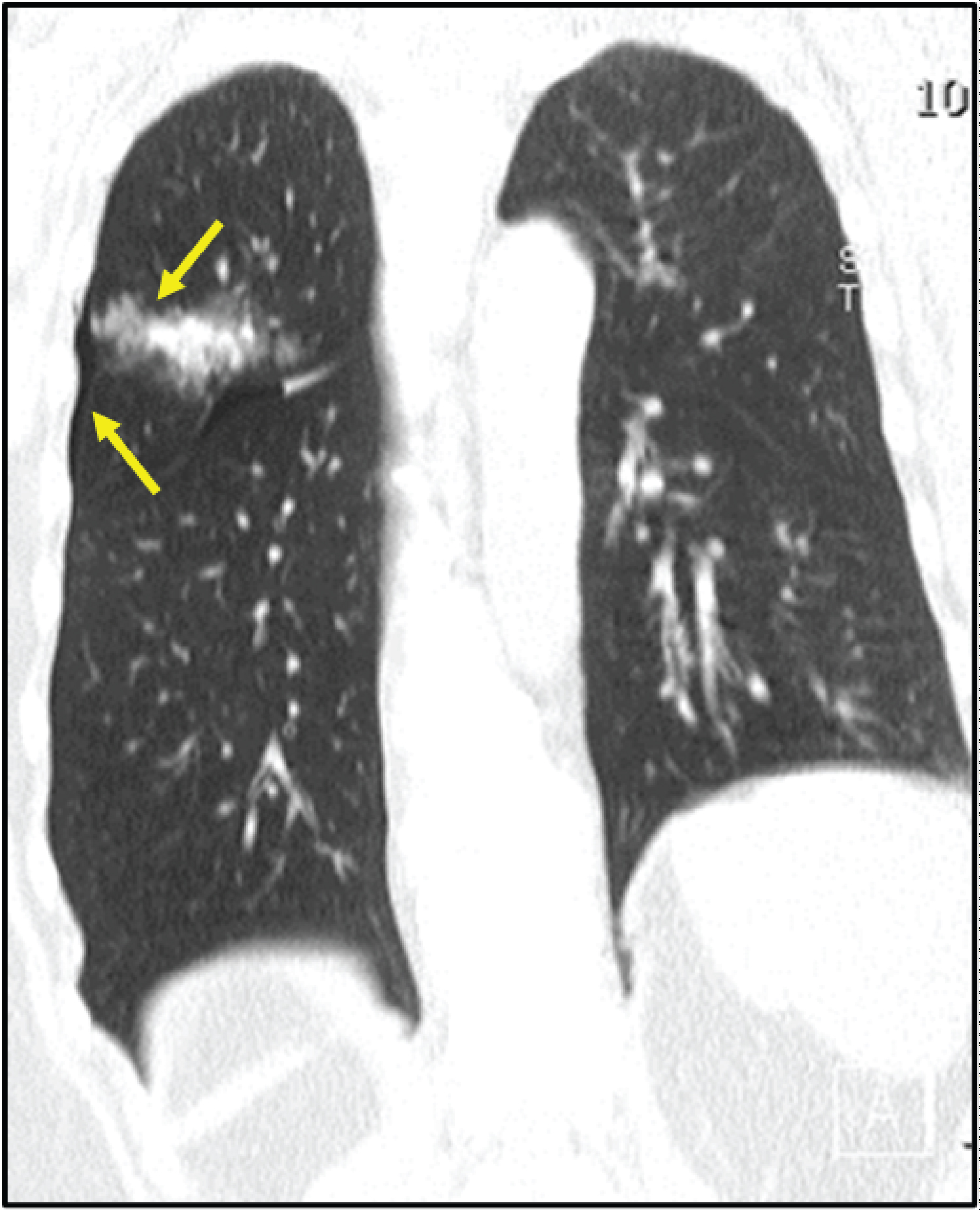 Figure 5: Postprocedural coronal CT scan showing a smaller pneumothorax and an alveolar hemorrhage adjacent to the biopsied nodule (yellow arrows).
View Figure 5
Figure 5: Postprocedural coronal CT scan showing a smaller pneumothorax and an alveolar hemorrhage adjacent to the biopsied nodule (yellow arrows).
View Figure 5
The patient did not have any symptoms suggestive of stroke, myocardial infarction, altered state of consciousness or arrythmia. He was positioned in Trendelenburg and right lateral decubitus and 100% oxygen via a non-rebreather mask was administered. Electrocardiogram showed no ST-segment elevation.
So he was transferred to the Intensive Care Unit (ICU) for clinical surveillance and patient close monitoring.
At ICU, he remained asymptomatic. He did not develop neurologic deficits, so no CT of the brain was performed, and he denied chills, chest and abdominal pain. He had no fever. He presented a mild tachypnea (20-25 cycles per minute), with a peripheral oxygen saturation of 100%. Chest examination revealed decreased breath sounds in the right hemithorax. He was hemodynamically stable.
Arterial blood gas analysis showed respiratory alkalosis and hypoxemia (arterial oxygen partial pressure- PaO2/fractional inspired oxygen - FiO2 ratio 170). Laboratory tests showed only a known thrombocytopenia (117,000/uL); troponin I and CK-MB levels as well as coagulation tests were normal.
Regarding the treatment, the patient maintained the 100% O2 supply and bed rest, preferably in the right lateral decubitus and in the Trendelenburg positions, with progressive improvement of hypoxemia.
Follow-up CT 24 hours after the procedures revealed total resolution of pneumothorax and SAE.
The patient was discharged to the ward 48 hours after ICU admission and left the hospital on day 6 in a stable condition, without any sequelae related to the SAE.
The nodule was diagnosed with adenocarcinoma with morphology compatible with primitive lung neoplasia.
We present a case of asymptomatic SAE, a very rare and potentially life-threatening transthoracic CT-guided lung biopsy complication that requires prompt diagnosis and effective emergency treatment in some cases [1,3,4,6,7,9].
Some factors contribute to increase the risk of SAE, including coughing during the procedure, positive pressure ventilation, chronic obstructive pulmonary disease, smaller lesions, procedures performed for a cystic or cavitary lesion, ground-glass nodules, the coexistence of vasculitis, inflammation, coagulopathy, friable lung tissue and prone position [1,4-8]. In fact, all conditions that increase the pressure gradient between the airway and pulmonary vein will contribute to increase the risk of air embolism [4,6,8,10].
In turn, some risk factors related to biopsy technique are lesion location (above the level of the left atrium), needle positioning/size, and sampling method - fine-needle aspiration versus core needle biopsy [1,6-8]. In our case, a core needle biopsy was performed. Concerning the technique per se, particularly the co-axial one, it can contribute to increase the SAE risk because it can be responsible by direct passage of air from the needle to a pulmonary venous when the patient breaths or coughs while the needle hub is open to the air [2,7,12]. In fact, the co-axial technique can lead to an increase in complications rates (38.8%), comparing to fine needle biopsy one (24%), according to the literature [5].
Thoracic CT scan should be performed during the procedure to determine an appropriate needle trajectory and the patient alerted to cease full inspiration when directed [7,11].
In our case, post-biopsy CT scans showed the relationship between SAE and transthoracic biopsy. Post-procedural CT scan allows early detection of SAE. Actually, even a small volume of air within the coronary and cerebrovascular system can lead to severe symptoms and complications owing to the vulnerability of these systems to hypoxia [1,2,3,7,8]. The volume of air required to cause end-organ injury and fatality is much less in cases of systemic arterial air embolism [2,7,8]. The patients with systemic arterial air embolism typically present with cardiovascular or neurological sequelae depending on end-artery obstruction [3,8,10].
In our patient, these diagnoses were excluded as he did not develop neurologic deficits, electrocardiogram showed no ST-segment elevation and serial troponin I and CK-MB levels were normal.
In our daily practice, a post-biopsy CT scan is performed routinely in all patients submitted to transthoracic CT-guided lung biopsy to exclude complications. In this case, after 24 hours, we evaluated the coronary arteries in the delayed post-procedure CT scan images to ensure SAE total resolution.
Regarding to underestimated incidence due to failure to diagnose SAE in asymptomatic patients, Freund, et al. reported that the incidence of radiologically proven SAE (3.8%) was superior to the incidence of clinically apparent SAE (0.49%) [1,2,5,10]. The incidence of post-biopsy SAE might be probably higher than is estimated [2,3,9,10]. Consequently, a control CT scan that include the biopsied lung region, the heart and great vessels should be performed in order to search for intravascular and intracardiac air, allowing increasing the detection of asymptomatic cases [1,2,5,7,10]. Besides, it is important to ensure a close monitoring of the patients that suffer this complication given the occurrence of delayed manifestations [4,6,10].
In our case, a rapid and significative volume of air was introduced into the pulmonary vein and consequently in left atrium and right kidney. The patient remained asymptomatic with an effective cardiac output, assuring hemodynamic stability.
It is very important to maintain an asymptomatic patient with SAE in the lateral decubitus, to prevent the passage of air to vital organs, until the air is absorbed [1,6,8]. Indeed, this position prevents air bubbles from entering the systemic circulation, keeping the left ventricular outflow tract in a nondependent position away from the aorta and trapping air in the left ventricle. This way, it prevents the passage of air into the brain or other important vasculature [3,10]. Even if neurological signs are already present, this position is mandatory to avoid more air reaching the cerebral circulation [3,4,6,8,10].
Clinicians should be familiar with the courses of the airway and the adjacent vasculature in high-risk patients in order to increase the safety of this procedure [4,7].
The ideal management of air embolism includes stopping the procedure, readying cardiopulmonary resuscitation procedures, placing the patient in the Trendelenburg position followed by a lateral decubitus position, supplying oxygen at 100% and, if possible, applying HBOT within 4-6 hours [3,4,7,9,10]. Oxygen administration will allow not only to treat hypoxia but also to eliminate the gas as it establishes a diffusion gradient that favors the regress of gas from the bubbles [4,6,8].
The Trendelenburg position and HBOT correspond to first-line treatments for SAE located within the coronary and cerebral vasculature [3,6,7].
According to various authors, all patients should be placed in Trendelenburg position immediately followed by a right or left lateral decubitus position according to localization of air embolism bubble seen on CT. So if the patient presents a venous air embolism, he should be positioned in left lateral decubitus or Trendelenburg position. In turn, if the patient presents an arterial air embolism, it is recommended to keep the patient in Trendelenburg position with right lateral decubitus [8,13].
Early HBOT is the only effective treatment available for arterial air embolism cases, promoting nitrogen reabsorption in the air bubbles, dissolving them, improving oxygenation in the ischemic tissue (Henry's law); reducing the dimensions of the gas bubbles (Boyle's law) and decreasing permeability of the blood-brain barrier, thereby preventing cerebral oedema [2,3,5,6,8,10]. The optimal time window for initiation of HBOT after SAE occurrence is not clear but, in some series, rapid application of HBOT within 4 hours was effective in all patients [8].
Additionally to SAE, our patient also presented an untreated small pneumothorax, which is an absolute contraindication to HBOT applying due to the potential risk into tension pneumothorax, influencing SAE management [8]. However, the treatment provided was sufficient to ensure total resolution of clinical situation.
As there is no standard protocol for managing asymptomatic patients, in our institution a thoracic CT scan is performed after the procedure to evaluate possible complications and the patients remain in observation.
SAE is a very rare and potentially life-threatening transthoracic CT-guided lung biopsy complication that requires a high index of suspicion, prompt diagnosis and effective emergency treatment to prevent morbidity and mortality [3,7,8,10,11].
All clinicians should be aware of the lung biopsy techniques that can contribute to minimize the risk of air embolism as well as immediate clinical manoeuvres that could contribute to stabilize the patient and reduce morbidity and mortality prior to definitive treatment [3,5,8,10].
Future research must be carried out to clarify SAE-related risk factors and to establish appropriate patient risk stratification when selecting management strategies.
Filipe Patrocínio, MEng that provided writing assistance and proofreading the article.