The objective of the current study was to assess the impact of sleep quality on pain sensitivity and depressive symptoms in the elderly.
In this cross-sectional analytical design study a total of 78 patients (65-85 years) with good general health status and 44 young (30-50 years) healthy volunteers were included. All subjects assessed by Pittsburg sleep quality index (PSQI), pain pressure threshold (PPT) and geriatric depression scale (GDS).
In geriatric subjects, components of PSQI were significantly higher (p < 0.05) as compared to controls, indicating bad sleep components in geriatric subjects. The PPT was significantly reduced among the geriatric patients vs. controls (p < 0.05), indicating a lower pain tolerance among the geriatric patients. Also, the elderly subjects had significantly higher depression scores than in control subjects (p < 0.05), indicating higher depression levels in geriatric group. In the geriatric group, except for the use of sleeping medication, all PSQI components and the total PSQI score showed a significant correlation with depression scores (p < 0.05), patients with higher depression levels have bad sleep quality.
Our results showed decreased sleep quality, pain sensitivity and an increased depression among elderly subjects as compared to younger individuals. These findings indicate that decreased sleep quality is associated with both increased pain sensitivity and increased rates of depression.
Aging, Sleep quality, Pain sensitivity, Depression
Assessment of health status in the elderly has become a more important research priority as a result of the global increase in the life-expectancy [1]. Sleep disturbances represent a leading problem in the elderly populations (≥ 65 years), with approximately 40% of the older individuals reporting sleep impairment and dissatisfaction from sleep quality [1-4]. Poor sleep quality may lead to day-time sleepiness, chronic fatigue, and increased risk of accidents and falls [5]. The prevalence of sleep disorders has been reported to increase after 30 years of age, followed by a plateau period and a subsequent additional peak after the 5th decade of life [1,4]. In recent years, we have witnessed a growing interest in sleep disturbances in the scientific community. Studies have shown that in addition to the natural course of ageing with a potential impact on sleep quality, a variety of other factors may also adversely affect the sleep quality, including medical and psychosocial co-morbidities as well as multi-pharmacy commonly utilized for their treatment [1].
Aging is associated with an increased likelihood of pain or discomfort in association with an increase in the occurrence of musculo-skeletal disorders [6,7]. Furthermore, structural, functional, and biochemical alterations occur in cerebral cortical receptors at all nociceptive levels as a result of aging [8]. Studies on pain sensitivity in the elderly have provided conflicting results, with some authors reporting increased pain sensitivity, in contrast with others reporting no change or a decrease [8-10]. Interestingly, in a study by Jensen, et al. only women were found to have an elevated pain sensitivity [11]. Gokoğlu, et al. [12] observed no differences in terms of pain sensitivity between elderly and younger individuals, while Pickering, et al. reported a lower pain sensitivity among male patients [13].
From a clinical viewpoint, depression represents a major psychiatric problem in the advanced age group (≥ 65 years). The high prevalence of depression in the geriatric population is a major determinant for other disorders affecting this age group [14,15]. The presence of depression has been shown to have multiple implications, such as increased healthcare expenditures, impaired physical functioning, and worsened disease prognosis [16]. Depression may also lead to musculo-skeletal disorders in individuals with pain [16-18]. In this regard, Berg, et al. showed an association between the severity of pain and depression, while several others demonstrated an increased pain perception in depressed individuals [19].
This cross-sectional analytical design study was undertaken at the outpatient unit of the department of physical therapy and rehabilitation. All patients provided written consent prior to study procedures. The study protocol was approved by the ethics committee.
A total of 78 patients (65-85) years of age with good general health status and adequate cognitive abilities who were followed up at the FTR osteoporotic outpatient unit of our hospital were included in the study. Cognitive assessments were performed using the Turkish version of the Mini Mental State Examination [21], and subjects who scored ≥ 25 points were considered eligible for the study.
Exclusion criteria included presence of hearing or comprehension difficulties, dysphasia, current use of anti-depressants or non-steroidal anti-inflammatory agents, pain as a major symptom, and gabapentin or pregabalin use.
A total of 44 otherwise healthy individuals between 30 and 50 years of age employed in our facility comprised the control group.
Sleep quality in the past month was assessed using the Pittsburgh Sleep Quality Index (PSQI), which consists of the following 7 components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Each component is scored on a 0-3 point scale, yielding a total score between 0 and 21. Higher total scores indicate poorer sleep quality. Also, a PSQI global score 5 or greater than 5 indicates poor sleep quality [22]. The validity and reliability of the Turkish version of this tool was demonstrated in 1996 by Ağargün, et al. [23], with a Cronbach alpha reliability coefficient of 0.804. A global PSQI score of 5 was found to be 89.6% sensitive and 86.5% specific for estimating sleep quality [22].
The most frequently used scale for measuring late-life depression is the geriatric depression scale (GDS). The GDS was originally developed as a 30-item questionnaire (GDS-30) in a simple yes/no response format [24]. Sheikh, et al. [25] developed a shorter 15-item form to improve the acceptability of the scale that used in our study. In the shorter form, scores above 5 represent depression with ascending severity. Scores of 0-4 are considered normal, 5-8 indicate mild depression, 9-11 moderate depression, and 12-15 indicate severe depression. The validity and reliability of the Turkish version of this tool was demonstrated in by Ertan, et al. [26].
A pressure algometer (Baseline® Dolorimeters, New York, USA, 2015) was used for assessing pain pressure threshold (PPT). The measurements were performed at the 1st dorsal inter-osseous muscle by the same investigator under the same test conditions, room temperature and test equipment. For assessments, a 1 cm2 circular probe was used which was connected to a pressure device calibrated to Newton/cm2 as the power unit. Pressure increments at a rate of 1 N/sec was performed until the perception of the pain by the subject. The test was stopped upon the "stop" command by the subject and the value on the screen was recorded. Each measurement was performed thrice, and the average of three measurements was recorded as the PPT.
IBM SPSS 23.0 statistical software pack was used for data analysis. Study data were assessed using descriptive statistics (frequency, percent, mean, standard deviation, median, min-max). The normal distribution of the data was tested using Kolmogorov-Smirnov and Shapiro-Wilk methods (data did not show normal distribution). Between-group differences were analyzed with Mann-Whitney U test, while Spearman's rho correlation test was used for the correlations between the variables. Values with a probability (p) of less than α = 0.05 were considered significant, showing a difference between the groups, while p values greater than 0.5 was considered to signify statistical insignificance and absence of difference. The results were evaluated in a confidence interval of 95%.
Of the 78 elderly included, 87% were female and 13% were male; among the 44 control subjects, the corresponding figures were 77% and 23%, respectively, with no significant gender differences between the two groups (p = 0.156) (Table 1).
Table 1: Comparison of elderly and young control group for demographic characteristics and evaluation parameters. View Table 1
In this group of geriatric patients, the subjective sleep quality (p = 0.000), sleep latency (p = 0.000), habitual sleep efficiency (p = 0.000), sleep disturbances (p = 0.000), and daytime dysfunction (p = 0.000) components of PSQI were significantly lower as compared to controls, while no differences were found for sleep duration (p = 0.074) and use of sleeping medication (p = 0.788) (Table 1).
The PPT was significantly reduced among the geriatric patients vs. controls (p = 0.000) (Table 1).
Also, the elderly subjects had significantly higher depression scores than in control subjects (p = 0.048) (Table 1).
Of the elderly subjects, 84.6% had impaired sleep quality (PSQI ≥ 5), while the corresponding figure among controls was 45.5% (Table 2).
Table 2: Sleep quality frequency in elderly and control group. View Table 2
There were not significant correlations between total PSQI score and PPT in the elderly (p = 0.851, r = -0.022); however, there was a significant negative correlation between the "use of sleeping medication" component of PSQI and PPT (p = 0.033, r = 0.241). In control subjects, a statistically significant correlation was found between the "habitual sleep efficiency" component of PSQI and PPT (p = 0.041, r = 0.310). No significant associations between PSQI total and other components were observed (Table 3).
Table 3: Correlation of pain pressure treshold and PSQI for elderly and young control. View Table 3
In the geriatric group, except for the use of sleeping medication (p = 0.075, r = -0.203), all PSQI components (subjective sleep quality (p = 0.000, r = 0.570), sleep latency (p = 0.000, r = 0.568), sleep duration (p = 0.036, r = 0.238), habitual sleep efficiency (p = 0.036, r = 0.238), sleep disturbances (p = 0.036, r = 0.238), daytime dysfunction (p = 0.017, r = 0.270) and the total PSQI score (p = 0.000, r = 0.570) showed a significant correlation with depression scores, while in controls, a similar correlation was found between all PSQI parameters sleep latency (p = 0.000, r = 0.624), habitual sleep efficiency (p = 0.030, r = 0.328), sleep disturbances (p = 0.000, r = 0.571), use of sleeping medication (p = 0.043, r = 0.307), daytime dysfunction (p = 0.014, r = 0.367) except for subjective sleep quality (p = 0.057, r = -0.290) and sleep duration(p = 0.237, r = 0.182) as well as the total PSQI scores and depression scores (Table 4). The correlation between depression and PPT was not statistically significant (p = 0.740, r = 0.38 in the geriatric group; p = 0.348, r = 0.145, in controls) (Figure 1).
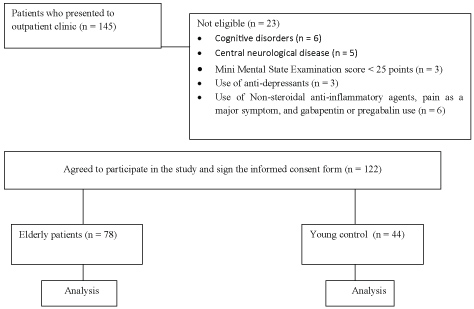 Figure 1: Flow diagram.
View Figure 1
Figure 1: Flow diagram.
View Figure 1
Table 4: Correlation of depression and PSQI for elderly and young control. View Table 4
Our results showed a significant reduction in sleep quality in the elderly study subjects in comparison with the control group consisting of younger individuals (i.e. those between 30 and 50 years of age). The age-related decline in sleep quality is generally thought to be associated with the alterations in neuronal sleep circuits. A slowing down in the activity of the central nervous system has been observed in the elderly individuals that results from the decrease in the levels of the endogenous neuropeptide orexins A and B, which are also referred to as hypocretin 1 and 2, respectively [27]. This decline in endogenous neuropeptides leads to a reduction in the total sleep duration, and even worse, to poor sleep quality [27-29]. Also, aging has an impact on several brain areas such as the cortex, hypothalamus, and the brainstem structure locus coeruleus. Again, consequent to such alterations, the ability to maintain a consistent circadian rhythm is impaired with aging, which is also associated with a decrease in cortisol and melatonin release. Furthermore, the reduced retinal sensitivity to light in the elderly further complicates the circadian disturbance. In line with these findings, a previous study reported that more than 80% of the elderly individuals had impaired sleep quality [30]. Malakouti, et al. [31] examined a total of 400 individuals over 60 years of age residing in a nursing home and found poor sleep quality in 82.6% of these individuals. Consistent with these reports, 84.6% of our study subjects had impaired sleep quality.
In our study; among our elderly individuals, the PPT was significantly lower than that among younger subjects. Also, the PSQI component "use of sleep medication" showed a significant correlation with the PPT. More than 70% of the elderly have been reported to suffer from chronic pain interfering with daily activities of living [32-34]. The reported prevalence of impaired sleep quality among subjects with chronic pain is in the range of 50 to 58% [35]. Both sleep disturbance and chronic pain represent a significant public health problem associated with significant functional and social impacts among the elderly [1]. An investigation into the effects of aging on pain sensitivity is not only important for describing the age-related differences, but also for delineating the underlying mechanisms for such differences. Until now, published data on such mechanisms has been scarce and indicate certain age-related alterations in the functions of peripheral A-delta fibers as well as disruption in the endogenous pain inhibition systems [37]. Ischemia and pressure stimulation have been shown to increase the pain sensitivity among elderly through activation of deep tissue nociception [38]. Edwards, et al. [39] found no difference between geriatric subjects and younger individuals in terms of the PPT measurements performed at the trapezius and masseter muscles. Donat, et al. [40] performed PPT measurements in the second and fifth digits, again observing no difference between younger and older patients. Mesci, et al. [41] examined the results of PPT measurements in older and younger individuals with chronic low back pain at the 1st dorsal interosseous, deltoid, and tibia sites, and reported no age-related differences. In contrast, Pickering, et al. [13] reported lower PPT in geriatric male patients. In another study, Lautenbacher, et al. [42] measured the PPT at the volar site of the left middle finger, and found lower threshold values for the elderly individuals. PPT measurements were performed by Cole, et al. [43] in the forearm, indicating lower threshold values among the elderly compared to younger individuals. In the current study, pain pressure threshold measurements were performed in the 1st dorsal interosseous muscle and lower threshold values were detected for the geriatric patients.
According to the results of our study, depression in the geriatric population is significantly higher than in the younger population (30-50 years). There was a significant negative correlation between sleep quality and depression. On the other hand, PPT and depression had no significant associations. Depression is a common disorder in the elderly population representing a significant health problem [44]. Our geriatric patients similarly had higher rates of depression than in younger subjects. The relationship between sleep disorders and depressive symptoms is complex, mutual, and not very well understood [44,45]. In a study examining the association between depressive symptoms and sleep disturbances in a group of elderly men, a strong link between sleep impairment and depressive symptomatology was observed [46]. Again, in another report, a negative association between sleep quality and depression was found, consistent with our observations [47].
Published data suggests that poor sleep quality is related with increased likelihood of depression in geriatric patients with chronic painful disorders, akin to the observations in patients with fibromyalgia [20]. Bair, et al. [48] showed an association between the severity of pain and depression, and Ohayon, et al. [49] reported increased severity and duration of depression as well as an increased likelihood of experiencing certain depressive symptoms in subjects with chronic pain. In another report, Smalbrugge, et al. [50] showed a correlation between anxiety and depression, and suggested the presence of a relationship between depression and pain severity. Baker, et al. [51] also demonstrated a direct and significant association between pain and depressive symptoms. On the other hand, Liffe, et al. [52] found no link between pain frequency and depression. In our study, the PPT was not significantly associated with depression.
A major limitation of our study is its limited sample size. Our results showed decreased sleep quality and pain sensitivity and an increased occurrence of depression among elderly subjects as compared to younger individuals. The results of our study also shown the association between ‘use of sleeping medication' and pain sensitivity in elderly. And these findings indicate that decreased sleep quality is associated with increased rates of depression. As a result of the increase in global life expectancy, studies are warranted to target these disorders that significantly and adversely affect the quality of life in the geriatric populations.
None.
We declare that they have no conflict of interest.
Informed consent was obtained from all individual participants included in the study.
Ethical approvement was obtained from instituional research committee and with the 1964 Helsinki declaration and comparable ethical standards.