Background: In 2021, leading pediatric healthcare organizations declared a national state of emergency in children's mental health in America. Anxiety disorders are among the most common mental health conditions affecting pediatric populations. The Diagnostic and Statistical Manual of Mental Disorders, 5th edition, recommends objective measurement of pediatric anxiety for evaluation of symptomatology and treatment response. The objective of this review was to summarize recommendations and resources for measuring pediatric anxiety, and to quantify and characterize utilization of outcome measures for generalized anxiety in pediatric psychiatry.
Methods: A literature review of PubMed, last searched on August 22, 2022, was conducted. Results were reviewed for use of objective rating scales for measurement of generalized anxiety by mental healthcare professionals in pediatric populations. Full text case reports and observational studies in English over the past 10 years were included. Clinical trials were excluded with the intention of focusing on real-world practice.
Results: Seventeen studies were identified for inclusion, most of which were conducted in Europe. There was minimal repetition in rating scale selection between studies. Many studies were prospective in nature, suggesting that anxiety rating scales may have been implemented for study purposes, rather than as routine practice.
Conclusions: These findings represent an essential step toward understanding how and to what extent anxiety rating scales are utilized in pediatric psychiatry and where quality improvement initiatives may be needed. The limited number of studies identified for inclusion suggests a potential need for increased utilization of objective rating scales, especially in light of the youth mental health crisis. There appears to be a lack of consensus regarding which measurement tools are most ideal. Education, training, and further research are warranted to optimize utilization of measurement-based care for generalized anxiety in pediatric psychiatry settings and to determine which scales are optimal for use in this context.
Outcome measurement, Outcome measures, Measurement-based care, Psychiatry, Mental health, Child, Adolescent, Anxiety, Generalized anxiety disorder (GAD), Rating scale
Mental health disorders remain one of the largest sources of economic burden worldwide, and the impact of the COVID-19 pandemic on child and adolescent mental health is not fully known. A systematic review estimated the economic impact of child and adolescent mental health disorders at $201 billion dollars in the United States in 2016, prior to the COVID-19 pandemic [1]; and literature cites the pandemic as a significant factor in rising anxiety rates in pediatric populations. During the pandemic, anxiety prevalence rates were estimated at between 18.9 and 23.87% in children and 15.4 and 39.9% in adolescents [2]. The toll of the pandemic contributed to a collaborative declaration by the American Academy of Pediatrics (AAP), American Academy of Child and Adolescent Psychiatry (AACAP) and Children's Hospital Association (CHA) regarding a national state of emergency in children's mental health in America [3].
If unrecognized and untreated, child and adolescent anxiety contributes to an already costly economic burden. Anxiety in the child and adolescent population is a contributor to parent absenteeism from work, student absenteeism from school, increased visits to primary care for somatic complaints, and an overall increase in utilization of healthcare services, such as emergency room and primary care visits. Untreated anxiety disorders can lead to severe mental health issues in childhood and chronic mental illness in adulthood [4,5].
Despite the increasing incidence of generalized anxiety in children and adolescents, it is unclear how frequently mental health providers (e.g., psychiatrists, social workers, nurse practitioners, physician assistants, psychologists, etc.) utilize reliable and validated tools for evaluation of generalized anxiety in pediatric populations. A well-established strategy to support clinicians in translating research into clinical practice is producing and implementing Clinical Practice Guidelines and Clinical Practice Toolkits [6,7]. This review was implemented to evaluate the need for quality improvement initiatives geared toward optimizing identification and management of generalized anxiety in pediatric psychiatry settings.
The DSM-5 is the gold standard for diagnosis of mental health conditions, including anxiety disorders, in children, adolescents, and adults in the United States [8]. Section II reviews each of the different anxiety disorders, including separation anxiety disorder, selective mutism, specific phobia, social anxiety disorder (social phobia), panic disorders (with a panic attack specifier), agoraphobia, GAD, substance/medication-induced anxiety disorder, anxiety disorder due to another medical condition, other specified anxiety disorder, and unspecified anxiety disorder [8]. APA discusses assessment measures in Section III of the DSM-5, with the recommendation that clinicians obtain baseline outcome measurements at the initial assessment and throughout treatment to monitor response [8]. The Patient-Reported Outcomes Measurement Information System (PROMIS) Emotional Distress-Anxiety-Parent Item Bank is suggested as a potential tool [8]. Objective rating scales are not utilized for stand-alone diagnosis of mental health conditions, but serve as a tool in supporting the clinician and family in screening for mental health conditions and evaluating treatment outcomes. Broad rating scales for general assessment of mental health may be used initially, followed by the use of anxiety-specific rating scales, if an anxiety diagnosis is suspected. Novel dimensional anxiety scale symptom measurement tools developed by APA for children, adolescents, and adults are not discussed in this paper as they are new and there is limited data available at this time [8].
Despite recommendations for objective monitoring of generalized anxiety within the DSM-5, there is a lack of strong and consistent recommendations for objective measurement of generalized anxiety by psychiatric providers in pediatric and adult treatment guidelines. In 2020, AACAP published a "Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents with Anxiety Disorders". This guideline supports the utility of standardized symptom rating scales in screening for generalized anxiety in children and adolescents, characterizing patient-specific symptomatology, and determining baseline anxiety severity to better identify symptomatic improvement throughout treatment [9]. Numerous objective rating scales for evaluation of generalized anxiety have been studied in pediatric populations (Table 1). The AACAP guidelines site the 7-item GAD Scale (GAD-7), teen/adult version; Screen for Child Anxiety Related Emotional Disorders (SCARED), parent and child versions; Spence Children's Anxiety Scale (SCAS), parent and child versions; and Preschool Anxiety Scale (PAS), parent version as examples of objective rating scales with acceptable psychometric properties in this population [9,10].
Table 1: Select tools for assessment of generalized anxiety in pediatric populations. View Table 1
While AACAP supports using symptom rating scales to obtain collateral during the diagnostic process, it is essential to note that there is poor to moderate agreement between youth and parents on symptom rating scales [9]. For internalizing disorders, such as GAD, AACAP suggests generally giving preferential weight to the youth's report, highlighting the importance of having children and adolescents complete their own rating scales, in addition to identifying parent-reported observations for additional perspective [9]. AACAP also suggests that standardized symptom rating scales could be useful for evaluating symptomatic improvement with Cognitive-Behavioral Therapy (CBT) in particular, given evidence of optimization of accurate assessment of treatment response and remission by therapists with this practice [9]. They suggest that standardized symptom rating scales should be considered in measuring response to pharmacological treatment as well, as a supplement to the clinical interview [9]. The guideline provides non-specific references to monitoring for adverse effects during the acute phase of treatment and for a resurgence of anxiety symptoms after treatment discontinuation [9].
While pediatric patients are considerably different from adults, adult treatment guidelines are sometimes applied to pediatric populations, given the greater abundance of data in the adults. There are no American Psychiatric Association (APA) clinical practice guidelines for psychiatric providers relevant to the management of generalized anxiety; however, many alternative guidelines are available to support identification and management of generalized anxiety in adults. This includes resources such as the World Federation of Biological Psychiatry (WFSBP) and Anxiety Disorder Association of Canada (ADAC) guidelines.
The WFSBP Guidelines were last updated in 2008, followed by the development of a guideline focused on primary care providers in 2012 [11,12]. The 2008 guidelines suggest that symptom rating scales, specifically the Hamilton Anxiety Scale (HAM-A), may be useful to monitor treatment effectiveness in patients with GAD [11]. Yet, they note that the Clinical Global Impression Scale (CGI) or self-reported outcome measures may be reasonable alternatives in busier practice settings [11]. The Anxiety Disorder Association of Canada (ADAC) guidelines also mention that objective scales can be utilized to monitor patient progress during anxiety disorder treatment [13]. Similar to the WFSBP guidelines, they make specific mention of the CGI scale as a viable option for use at each follow-up appointment, given its brevity, ease of use, and comprehensive nature [13]. Additionally, they note that the HAM-A is less useful in real-world practice as opposed to clinical trials [13].
For this narrative review, a literature search was conducted in PubMed in an effort to quantify and characterize utilization of objective rating scales in screening, diagnosis, and/or measurement of treatment outcomes in pediatric psychiatry patients in whom there is concern for generalized anxiety. Results were reviewed to identify utilization of pediatric anxiety rating scales over the past decade by psychiatric healthcare providers, including, but not limited to psychiatrists, advanced practice providers, pharmacists, psychologists, social workers, case managers, and therapists. The following combination of search terms was utilized within PubMed: Anxiety AND ("measurement-based care" OR "rating scale" OR scale OR tool OR instrument OR checklist OR screener). Search filters were implemented to limit results to full text case reports and observational studies published in the English language over the past 10 years in humans between 2 and 18-years-old. Studies with a mixed population of children or adolescents and adults were permitted for inclusion. There was no minimal or maximal study duration requirement. Clinical trials were excluded with the intention of focusing on evidence from real-world clinical practice.
A single reviewer screened each record and each report retrieved, and collected data from each report that was included. Studies were excluded during the screening process if rating scales were administered outside of inpatient and outpatient psychiatry or by another discipline, other than psychiatry. Web-based questionnaires were considered indicative of a non-psychiatry setting. Studies solely in patients under the age of 2 or adults, defined as 18 years of age or older, were excluded, as were studies in women, men, caregivers, college and university students, peripartum populations, and mothers, terms which were considered an indicator of a predominantly adult population. Studies of alternative forms of anxiety, such as state anxiety, social anxiety, and separation anxiety, were not included, nor were hypothetical patient cases or studies using avatars. Studies that were sought for retrieval were reviewed for use of objective rating scales for the evaluation of generalized anxiety by psychiatric providers and/or within a psychiatry setting. Attempts were made to contact authors for missing details (Table 2).
Table 2: Use of objective rating scales for measurement of generalized anxiety in pediatric psychiatry. View Table 2
The search, last conducted on August 22, 2022, yielded 329 results (Figure 1). After screening article titles and abstracts, 202 articles were excluded. One hundred and twenty-seven articles were sought for retrieval and of the 123 articles retrieved, 106 further articles were excluded. The majority of studies that were excluded were conducted in a non-psychiatric setting or adult population. In three studies in which age or treatment settings were unclear, attempts to contact authors for missing details were unsuccessful.
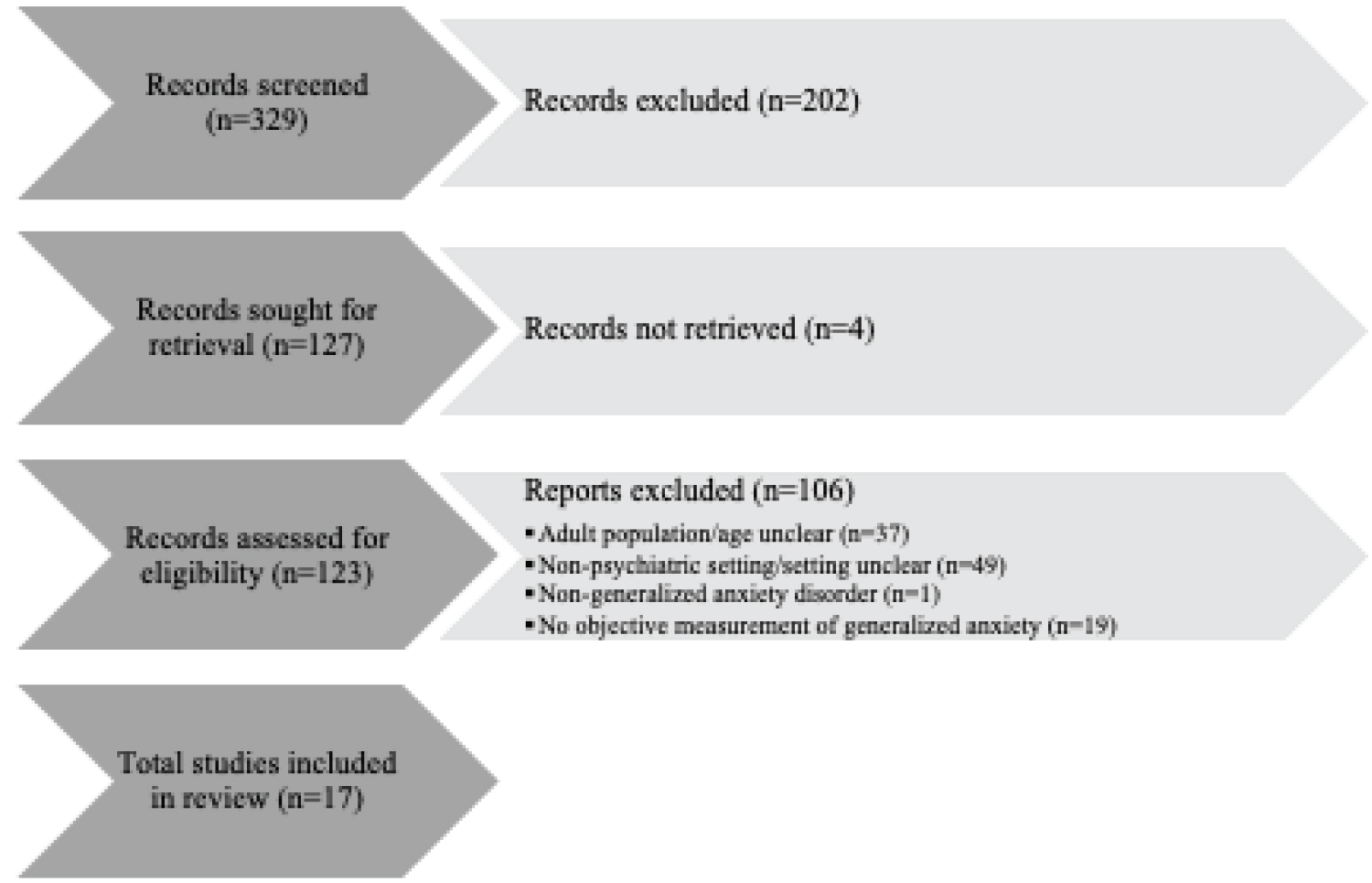 Figure 1: Flow diagram of study identification, screening, and evaluation.
View Figure 1
Figure 1: Flow diagram of study identification, screening, and evaluation.
View Figure 1
A total of 17 studies were included (Table 1), a handful of which had were in older adolescents or included a predominance of adults. The majority of studies that were included utilized diverse rating scales for the measurement of generalized anxiety, indicating a lack of consensus as to which objective rating scales may be most ideal for evaluation of generalized anxiety in the pediatric psychiatry population. The HAM-A, GAD-7, RCADS, and SCARED were most commonly utilized, with each scale administered in two different study populations. None of the studies that were included utilized the PROMIS. The majority of studies were conducted in Europe, and only four United States-based studies met criteria for inclusion. Most studies were prospective in nature, lending the question as to whether or not anxiety rating scales were implemented for the purpose of the study, rather than as a routine standard of care.
There is a national state of emergency in children's mental health in America, warranting closer evaluation of pediatric patients for mental health conditions, including anxiety. This narrative review identified a limited number of studies using objective rating scales for assessment of generalized anxiety in pediatric psychiatry practices, suggesting a potential need for improvement in utilization of measurement-based care in this population. The wide variety of rating scales utilized in the studies that were included suggests a lack of consensus regarding which tools are most ideal and a need for further research in this area. Traditionally, mental health screening and outcome measurement tools have been discredited due to poor psychometric properties. Poor positive predictive value and lack of adaption for specific age groups are potential barriers to uptake. Lack of consistency between recommendations within the DSM-5 and commonly utilized pediatric and adult anxiety treatment guidelines may cause confusion among providers regarding which tools to utilize. The availability of a number of different tools for measurement of generalized anxiety in pediatrics could also lead to indecision and a subsequent reduction in utilization by healthcare providers.
Another critical issue centers around reimbursement of time for completion of objective rating scales in clinical practice. A new Current Procedural Terminology (CPT) behavioral code of 99417 was added in 2021 enabling clinicians to bill for additional patient time in fifteen minutes increments [3]. Consultation with professional certified billing consultants may be useful for mental healthcare providers, given that billing and coding differences exist between private insurance, Medicaid, and Medicare.
Additional clinical research and naturalistic studies on utilization of objective rating scales for measurement of generalized anxiety are needed to support screening, diagnosis, and management of anxiety in the pediatric psychiatry setting. Objective measurement may facilitate early detection of generalized anxiety, which is essential, given the current youth mental health crisis, as well as the fact that disorders, such as anxiety, that develop in early life increase the risk for additional psychiatric conditions in adulthood [1]. Knowledge deficits in insurance reimbursement for use of objective rating scales require education and training of mental health professionals to incentivize incorporation of these tools into clinical practice. Incorporation of rating scales into Clinical Care Pathways [14,15] may facilitate utilization. Lengthier scales may also be available in alternative "short versions", knowledge of which could assist in promoting objective measurement of anxiety in busy clinical practices. In line with the recommendations within the DSM-5, mental health professionals are encouraged to consider incorporating objective measurement tools into their clinical practices.
Brittany Finocchio is an employee of Takeda Pharmaceuticals U.S.A., Inc. Wanda Hilliard has no conflicts of interest to declare. The views expressed are those of the authors and do not necessarily reflect the views of Takeda Pharmaceuticals U.S.A., Inc or Texas Tech University Health Science Center.
• What's known
○ Anxiety disorders have been cited as one of the most common mental health conditions affecting pediatric populations, and objective measurement of symptomatology and treatment response is recommended by the Diagnostic and Statistical Manual of Mental Disorders, 5th edition.
• What's new
○ In 2021, leading organizations in pediatric healthcare came together to declare a national state of emergency in children's mental health in america.
• What's relevant
○ Knowledge deficits in insurance reimbursement for use of objective rating scales require education and training of mental health professionals to incentivize incorporation of these tools into clinical practice.
○ Further research is needed to best elucidate which rating scales are most ideal for baseline and ongoing assessment of generalized anxiety in children and adolescents.