The accessory soleus muscle is a rare anatomical variant that usually occurs in adolescents or young adults. And it may manifest as an exertional ankle pain and swelling or as an asymptomatic posteromedial mass. However sometimes it may be mistaken as a soft tissue tumor at the ankle. The purpose of this study is to heighten awareness about the existence of accessory soleus muscle in a swelling at the posteromedial aspect of the ankle and to reduce the failure to recognize this muscle in MRI.
Accessory soleus muscle, Congenital anatomical variant, MRI diagnosis, Ankle
The accessory soleus muscle is a rare congenital anatomic variant, whose incidence is estimated to occur in 0.7% to 5.5% of the general population [1-3]. Clinically, if the muscle belly is large, the accessory soleus muscle may appear as a soft tissue prominence posterior to the medial malleolus. It will become pain and swelling in the posteromedial aspect of the leg with activity. Sometimes it can be misdiagnosed to other diseases, such as lipoma, ganglion, hemangioma, sarcoma and synovioma [1,2]. Radiological investigations include plain radiographs, US, CT and MRI [4-7]. However, MRI has characteristic diagnostic value to this disease [3,5]. A male patient who is 25-years-old with an accessory soleus muscle that demonstrated with MRI is reported.
A 25-year-old man presented with a posteromedial mass in the left ankle over one month. The patient described the mass becoming painful after significant physical activity. And there was no special medical history to this area. Physical examination revealed a tender soft-tissue mass and swelling of the left posterior-medial ankle located just anterior to the Achilles tendon. The patient was suggested to be performed by MRI to exclude a soft-tissue tumor.
The MRI examination was performed using a 1.5-T MRI unit Signa Advantage Horizon; GE Medical Systems, Milwaukee, WI, USA. The T1 weighted coronal sequences showed the mass originating from the ventral portion of the normal soleus muscle and inserting to the medial surface of the calcaneus independently of Achilles tendon (Figure 1). Compared with the normal side, the affected side showed a homogeneous soft tissue mass located posteromedial to the flexor hallucis longus tendon and anteromedial to the Achilles tendon in all sequences (Figure 2, Figure 3 and Figure 4). It showed iso intense signal on all sequences (Figure 2, Figure 3 and Figure 4). And the pre-Achilles' fat pad was compressed by this muscle mass. The T1-weighted sequences showed a thin rim of adipose tissue within the fascial plane around the mass (Figure 1).
 Figure 1: The T1 weighted sagittal sequence shows the mass (arrow) originating from the ventral portion of the normal soleus muscle and inserting to the medial surface of the calcaneus independently of Achilles tendon. View Figure 1
Figure 1: The T1 weighted sagittal sequence shows the mass (arrow) originating from the ventral portion of the normal soleus muscle and inserting to the medial surface of the calcaneus independently of Achilles tendon. View Figure 1
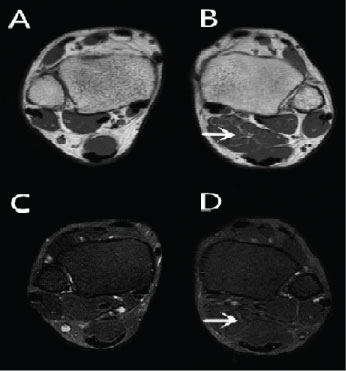 Figure 2: (B) Spin echo T1 weighted and (D) fast spin echo T2 weighted fat-suppressed axial images sequences shows that the accessory soleus muscle (arrow) had the same signal with adjacent muscles on all sequences. The A and C show the opposite side that is normal. View Figure 2
Figure 2: (B) Spin echo T1 weighted and (D) fast spin echo T2 weighted fat-suppressed axial images sequences shows that the accessory soleus muscle (arrow) had the same signal with adjacent muscles on all sequences. The A and C show the opposite side that is normal. View Figure 2
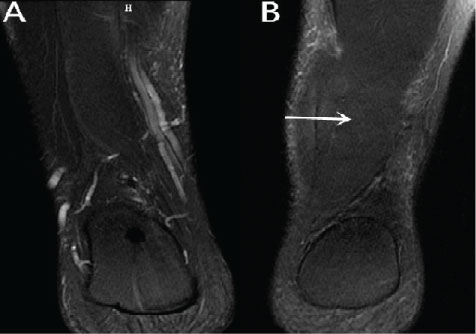 Figure 3: Fast spin echo T2 weighted fat-suppressed coronal images sequences show the differences between the both sides. View Figure 3
Figure 3: Fast spin echo T2 weighted fat-suppressed coronal images sequences show the differences between the both sides. View Figure 3
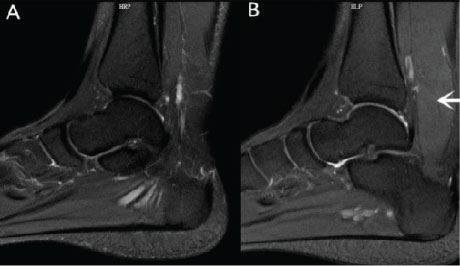 Figure 4: Fast spin echo T2 weighted fat-suppressed sagittal images show the differences between the both sides. View Figure 4
Figure 4: Fast spin echo T2 weighted fat-suppressed sagittal images show the differences between the both sides. View Figure 4
From the above imaging appearance soft tissue tumor was excluded with accurate diagnosis of accessory soleus muscle. The patient was avoided from unnecessary treatment. The patient's painful symptoms had been relieved by freeing from heavy activities.
Hatzantoniset, et al. [8] demonstrated the prevalence of the accessory soleus muscle in cadaveric specimens was 0.7-5.5%, which was equivalent to the 3% prevalence of the accessory soleus muscle in imaging patients. The males were more likely to possess the unilateral accessory soleus muscle while the females possess the bilateral accessory soleus muscle. The overall prevalence of the accessory soleus muscle by gender has been found to be 2.4% in males and 2.1% in females [8]. Although there have been several clinical cases of symptomatic pain associated with the accessory soleus muscle, most individuals area symptomatic and it is an incidental finding during routine investigation [8].
The attachment sites of the accessory soleus muscle can be mainly concluded into five types in previous studies [8-10]. They include: 1-insertion along the tendon of Achilles, 2-fleshy insertion to the upper surface of the calcaneus, 3-tendinous insertion to the upper surface of the calcaneus, 4-fleshy insertion to the medial surface of the calcaneus, 5-tendinous insertion to the medial surface of the calcaneus (Figure 5). The present case shows that the insertion of the accessory soleus muscle is on the medial surface of the calcaneus along the tendon of Achilles and the root of the accessory soleus muscle is the ventral portion of the normal soleus muscle.
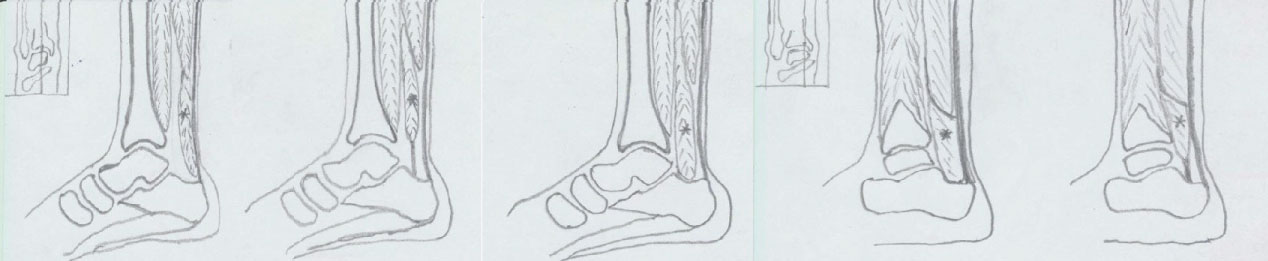 Figure 5: I: Insertion along the tendon of Achilles; II: Fleshy insertion to the upper surface of the calcaneus; III: Tendinous insertion to the upper surface of the calcaneus; IV: Fleshy insertion to the medial surface of the calcaneus; V: Tendinous insertion to the medial surface of the calcaneus. View Figure 5
Figure 5: I: Insertion along the tendon of Achilles; II: Fleshy insertion to the upper surface of the calcaneus; III: Tendinous insertion to the upper surface of the calcaneus; IV: Fleshy insertion to the medial surface of the calcaneus; V: Tendinous insertion to the medial surface of the calcaneus. View Figure 5
Although the presence of an accessory soleus muscle is not uncommon, patients are rarely symptomatic [11]. The accessory soleus muscle always manifests as a soft tissue mass in the posteromedial region of the ankle. However, it is also responsible for some congenital club foots [12-15]. And the symptomatic accessory soleus muscle always has a painful swelling in the posteromedial region of the ankle [1]. Pain in symptomatic patients is mainly due to an ischemic blood supply, compression of the tibial nerve by the accessory soleus muscle, excessive pressure on the nerve innervating the accessory soleus muscle, or a localized compartment syndrome [1,16].
The accessory soleus muscle can be diagnosed by many methods. From the beginning it usually diagnosed by surgical exploration. The plain x-ray shows that the Kager's triangle is replaced by soft tissue mass. Ultrasonography can also demonstrate the extra normal muscle echotexture [7]. Computed tomography can show the exact location of the accessory soleus muscle but can hardly differentiate this variant from other soft tissues masses. MRI can lead to definite diagnosis because of the ability to discriminate the signal between normal muscle tissue and tumorous masses [7,17]. Furthermore, MRI can clearly define the sites of origin and insertion of the accessory soleus muscle. Currently MRI is the most effective noninvasive method for a definitive diagnosis of the accessory soleus muscle.
Based on the advantages of MRI, it is more likely to differentiate the accessory soleus muscle from other soft tissue tumors in the posteromedial aspect of the ankle includes lipoma, ganglion, hemangioma, sarcoma and synovioma. The key to the differentiation from other lesions is the findings of MRI signal characteristics that are consistent with normal muscle, the main trunk of the mass and the typical anatomic location [2]. MRI scanning of the contra lateral ankle can help radiologists to get the correct diagnosis.
The therapeutic indication is based on the presence or severity of the symptoms. For asymptomatic patients, it is not necessary to treat. For the patients with moderate symptoms, conservative treatment can be proposed. However, it is essential for severe patients to perform surgical treatment [10].
In conclusion, the accessory soleus muscle is a congenital anatomic variation rather than soft tissue tumors. In fact, the characteristic appearance on MRI allows a confident diagnosis without the need to resort to biopsy. This case would alert radiologists to understand the lesion at this special location, and alert them to distinguish it from other soft tissue tumors. Combining with the imaging features and clinical presentation, the unnecessary damage to the patients can be avoided.