Introduction: Foot healthcare studies reports a high fraction of population possesses footwear related ill-fitting. These feet related ill-fits may vary with difference in nationality and ethnic groups. The aim of this study was to examine and establish the current feet size and shape of a population of children in the Zlin region of the Czech Republic.
Methods: A total of four hundred and sixty-nine children within the age range of 6-15 years participated in the investigation. Using a 3D scanning device based on foot-shoe interaction, size and shape measurements of the foot (length and width) were collected. To this, short questionnaires were completed by the participants to rate their age, sex, height and weight followed by pairing with the foot size data measurements of length and width of the left and right legs.
Results: Nine quantitative parameters related to the fit were identified and examined: Age, height, weight as well as others including the length and width of both left and right foot. Overall, the linear statistical model depicted p < 0.05 for the measured length and width of the left and right foot. Following the established results from the represented population size of 54.5% girls and 42.6% boys, it was observed that the average width and length of the both feet were approximately equal to 8.40 and 21.35 cm, respectively. However, it was observed that the foot length showed greater standard deviation than the width. In addition, the size difference between the male and female children examined in terms of length indicated a linear equation with an added constant of 0.34 cm for the males.
Conclusions: This study reflects the foot health of Zlin region children and how factors of foot size and shape affect this issue. Based on gender variation, results obtained provide valuable insight about foot size difference in childhood for healthy foot development.
Footwear, Foot fit, 3D scanning, Measurement, Size
3D: Three-Dimensional; R2: Correlation Coefficient; C.I.: Confidence Interval; SD: Standard Deviation; N: number of participants; SE: Standard Error
Foot health is a vital issue significantly dependent on healthy and functional footwear during childhood. But nowadays, it is usually ignored for the sake of fashion. Therefore, the importance of shoes to fit has been one of the leading discussions in the footwear industry [1-4]. Parameters such as shape, size and design of footwear has proven to greatly influence foot development, function and foot health [5-8]. According to current studies, approximately 30% of the global adult population depict different foot pathology or pain [9,10], with some of these defects associated with neglected foot healthcare during childhood which over the years has developed into malformations leading to reduction in mobility, decrease in leg strength, increase fall risk and decrease in body stability [11-13]. Amongst all, studies show that the main source of these foot pathologies relates to ill-fitting [14].
The foot is influence by several factors from different health areas including development, biomechanical and clinical. However, it is highly important to understand foot-shoe interaction, materials used in the manufacture of the shoe, and the functioning of the footwear industry [1,3,4,8]. In addition, it is worth mentioning that the effects on foot health are a gradual process with primarily long-term perspectives [4,5,7]. Notwithstanding, the development of the foot plays a key role primarily in childhood, where footwear influences most of the structural development and foot functions [2,3,15,16]. For example, the development of the foot arches (longitudinal arch length, arch height and navicular arch) occurs during the first decade of life and the morphology of a child’s foot in the future may be impacted by improper changes in these arches [17]. This may lead to gait pathologies caused by deformity and pain especially during the usage of footwears.
Over the centuries, the use of footwear has proven to play important roles both during childhood and adults’ life cycle and has been related to several diseases including metabolic disorders, inflammatory arthritis, neurodegenerative disorders, balance control, etc. [13]. Furthermore, available evidence shows that foot structure development in children and teenagers may be effected by anatomical structures, different growth patterns and abnormal variation of plantar pressure [18-20]. Another factor that may greatly influence foot development relates to fashion designs [21,22]. For example, in the western countries footwear have proven not to be use only as functional materials, but represents personal identity and plays a vital role in the society [10]. In most cases, styling and fit do not always correspond with foot health related issues which cause foot pain and may lead to development of foot deformity [22,23]. This suggests that to maintain good foot health, the use of any shoes must fit someone socially, fashionably and also functionally [13,24]. Furthermore, this shows that correct shoe fitting plays an important role in foot pathology and this aspect is highly necessary to identify the current size and shape distribution of a given population [10,23]. Since the difference in nationality and ethnic groups may also influence the shape and size of the foot [25]. For example, a comparison study performed between German and Australian children showed that the German children had larger and flatter feet to that of children from Australia [26]. Another similar supporting study evaluated the importance of prevention and foot care by investigating between appropriate footwear and foot-shoe interaction to reduce foot pain and illnesses [13].
Recently, most research studies have proven to focus on four areas (practicalities, personal, purpose, and pressure factors) which are important for shoe fitting and widely incorporated during production in footwear industries [27]. However, the fit of shoes is defined by varying parametric factors including length, girth, width, and the height of toe box and shape [7,28]. But amongst all, the length has proven to be one of the most significant parameters especially in children and considering several studies, the deduced results show that at least half of all children wear shoes of inadequate length [23,30]. In so doing, this might lead to malformations and deviation of the big toe during future development causing poor foot health and mobility at adult age. In this study, the main purpose was to examine the variation of foot size and shape based on length and width in a children population of Zlin of the Czech Republic and establishing its importance between foot-shoe interaction. In addition, the objective of this study was to create a database of foot size range of adolescent children in the Zlin region for the purpose of science and research.
The study was designed with the aim to evaluate the foot size of a sample of children in length and width with relation to age, height and weight. Following the interpretive sampling and selection criteria of the geographical location, the research was performed as part of a public event in the Zlin Region, Czech Republic. The randomized sample included a study population made up of 462 participants between the age of 6-15 years. The study was carried out for 3 days and the research involved the participants filling anonymous questionnaires, where the following data were required; gender, age, height, weight and region of origin. Based on elimination of extreme data values enters and incorrectly filled questionnaires, the final study sample was composed of 252 girls (54.50%) and 197 boys (42.60%).
A measuring scanning device was developed by researchers from Tomas Bata University in Zlin under a project from the Technology Agency of the Czech Republic (TACR). The measuring device consisted of four 3D scanning units that scanned the foot at 90° following an in-plane mesh deformation measurement. In brief, the respondent stands comfortably on the mat with both feet and we performed measurements simultaneously for the left and right foot. For an accurate foot size measurement, three points (foot length, foot width and height of the instep) are to be evaluated as major factors in terms of shape classification of the foot. Three-point cloud measurements were obtained from each scanning unit and then linked to the final object by the developed algorithm. The error between cloud measurement of the real measured foot size and the linked algorithm was less than 5 mm. A total time of approximately 30 seconds was used in measuring a single object. Prior to each measurement, the device was calibrated using a developed calibration algorithm. The calibration was performed using a calibration cube of known dimensions followed by data collection. To depict a scenario of real measurements, the data acquisition procedure was always the same in the following:
1. The respondent was asked to fill in an anonymous questionnaire with a generated random measurement number.
2. The respondent was asked to pull off his/her shoes and stand in socks on a measuring pad on which the position marks were located. If the respondent had no socks, he/she was provided nylon socks.
3. The subject was asked to stand still and relaxed on the mat for about 30 seconds.
The research questions were answered in the form of quantitative research followed by measurement on a scanning device. The validity of the study was based on the possibility of measuring a large number of respondents in a relatively short period of time. The questionnaire data were paired with the measured foot size values from the 3D scanning measurements such as the length and width of the left leg, the length and width of the right leg, and the diameters over the length and width of both legs. In addition, respondents were asked about their foot health status, but the vast majority of respondents were unwilling to disclose this information. For this reason, we did not include this item in the statistical evaluation of the sample of data.
The collected answers to the research questions and paired to the 3D scan measurements of length and width fit were solved using statistical hypothesis testing and standard tests such as paired t-test, Wilcoxon test and linear model with dummy variables. For presumptive analysis, a 95% confidence interval was examined and the experimental p-value compared with a less than 0.05 significant level. We believe that the above-mentioned statistical approach is relevant and effective for answering research questions, in particular through the mass processing of large amounts of digitized information. In addition, the data were checked using descriptive statistics methods for extreme values such as boxplot, skewness and spikes estimates. All values outside the calculated range were considered outliers [31]. Data items with extreme values and incorrectly filled in questionnaire were removed from the analysis filtering to 462 respondents. Statistical analyses were carried out using SPSS® Statistics Version 3.6.1.
Table 1 presents the descriptive statistics calculated from the collected quantitative data. However, the weight and height data are incomplete due to respondents' ignorance of these values.
Table 1: Description of quantitative items of the analysed samples. View Table 1
Based on the descriptive statistics analyses, the average length of the left and right feet was approximately equal to 21.35 ± 2.08 cm. But it should be noted that in this age period the foot is in development and as such is very indicative. On the other hand, the average foot width was determined to around 8.4 cm and following the deduce results it could be noted that the foot lengths showed greater standard deviation than the foot widths. This observation can be attributed to the fact that during the development of the foot, the length of the foot gradually changes more than its width. According to further deduced results, the median length of both feet was approximately the same determined as 21.30 cm and 21.25 cm. The skewness and kurtosis values suggested that the increase in foot length might be attributed to normal distribution. However, this do not apply to the foot width (Figure 1).
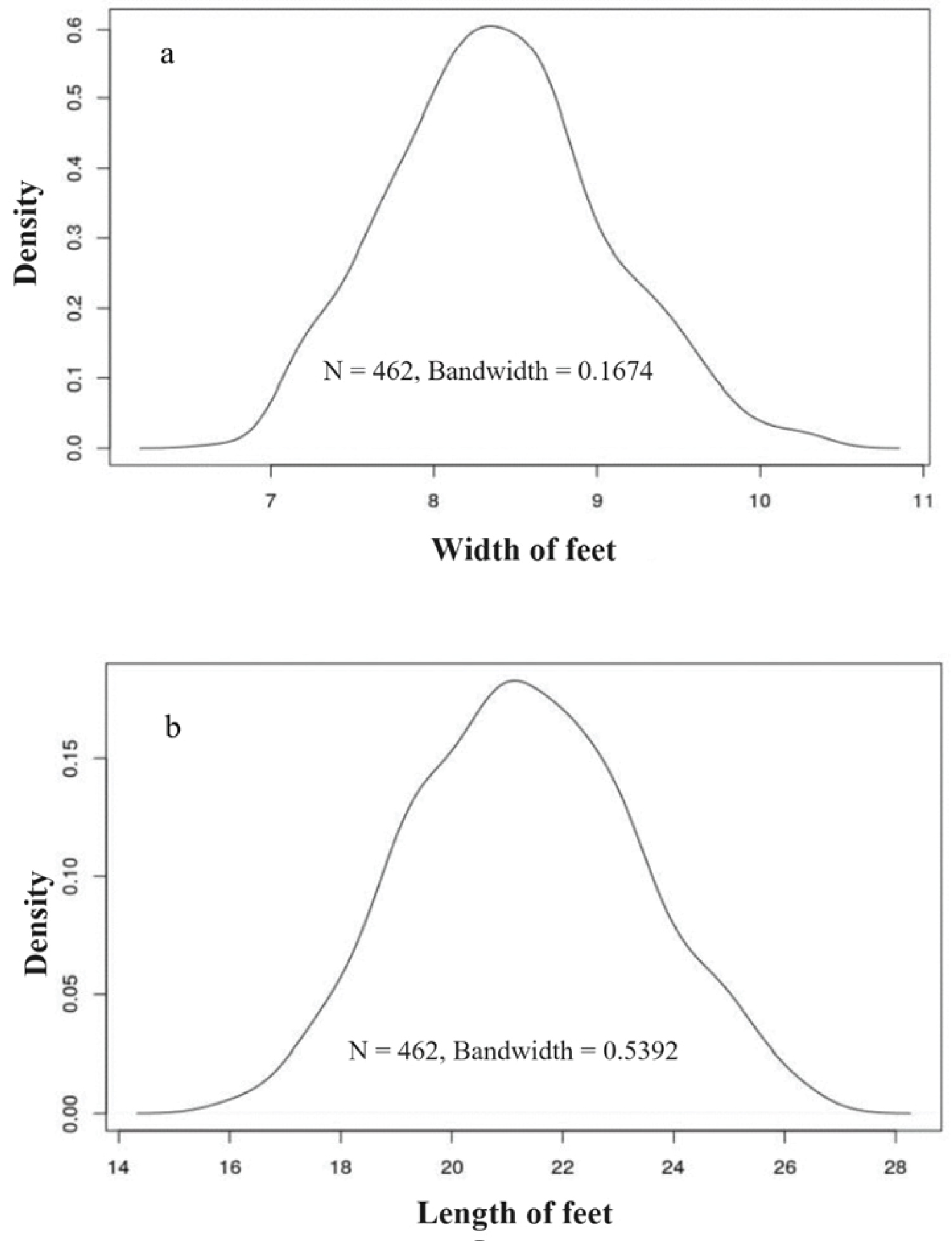 Figure 1: The graphs shows kernel density estimation for (a) Foot width and (b) Foot length of the studied population.
View Figure 1
Figure 1: The graphs shows kernel density estimation for (a) Foot width and (b) Foot length of the studied population.
View Figure 1
From these graphs it is possible to deduce the normal distribution of the file. For this reason, a Shapiro-Wilk test was applied to verify the normality of the foot length and width distribution based on the left foot length (W = 0.9954, p-value = 0.1910), right foot length (W = 0.9963, p-value = 0.3688), left foot width (W = 0.9893, p-value = 0.0019) and the width of the right foot (W = 0.9909, p-value = 0.0059). Following the obtained Shapiro-Wilk test results, the foot length was divided in the set using a normal p-value distribution of > 0.05 for foot widths below the p-value of 0.05. Thus, the foot width was not divided according to the normal distribution. For this reason, different parametric tests for the foot length and non-parametric tests for foot width were used. A standard paired t-test was subsequently applied to answer question 2 whether the left and right feet differ significantly from each other. The Paired t-test compared the difference in the means of data length left and length right yields and mean the difference of 0.05 (CI-95% = [-0.06; 0.15]; p-value = 0.3880). Considering we do not have enough evidence to reject the null hypothesis that the mean of the deviations equals 0, we assumed that there is no statistically significant difference between the length of the left and right foot. If this difference exists then the mean value will be around 0.05 cm. For the width of the foot, a non-parametric test implemented to compare the mean value followed by application of the Wilcoxon test. As such, the Wilcoxon signed rank test with continuity correction compared the location shift for width left and width right data yields determined with p-value of < 0.001. Given the p-value was < 0.05 confirmed we have enough evidence to reject the null hypothesis of the same median. Therefore, we will assume that the width of the left and right foot differs significantly. The difference in median was approximately 0.1 cm. However, given the magnitude of this difference and the nature of the study, the value was termed critical and thus not considered.
To answer the 3rd question, we based on the fact that the foot develops with age and thus it was not possible to do a standard t-test for 2 groups. Therefore, we used a linear regression following the equation 1, given gender was applied as the dummy variable.
Where, Length both is the average length of the foot (one subject), i relates to the identification number of the subject, β0 is the intercept, β1 is the slope, Age is the subject's age i, and β2 is the respondent's sex dummy variable and ei is the error term.
As can be observed in Table 2, all determined coefficients were statistically significant. Overall, the model depicted to be also statistically significant with F (2,446) = 255.40 and p-value < 0.05. However, R2 on the second model was lower than the default value with 0.6, but this model explains 53.40% variability. The intercept could not be interpreted as none of the analysed groups were of zero-years-old. If we increase the age value by one year, the foot length will increase by 0.72 cm. But in the case of males, an addition of 0.34 cm was observed.
Table 2: Calculated values of the different parameters for the linear model. View Table 2
To the best of our knowledge, this is the first study to estimate the foot size and shape of community-dwelling children in this region of the Czech Republic. This is a descriptive cross-sectional study of foot size and shape in relation to footwear worn by a consecutive convenience sample of children who are community-dwelling. This provides a detailed description of the size and shape of the foot in terms of length and width for these children in relation to common potential footwear characteristic problems in this group. It may not be generalised to all community-dwelling children but may be relevant in future clinical assessment and treatment settings. In addition, the sample size of 462 participants is relatively small, leading to a narrow CI of 95% around the estimate proportion of foot sizes. We did not measure the shoe dimension of the participants; thus, we are unable to determine the interaction between the foot morphology and the footwear.
Foot size assessment based on length and width in terms of fitting is crucial and should be considered with great scrutiny when relating to foot health during childhood since it may result in future developments of malformations. As such, the need to design children’s footwear based on 3D scanning technology following different foot morphologies with required allowances in age, foot height, length and width is vital to reach better foot health. Considering the holistic thought that ‘fit’ agrees with foot health, we believe that it is important to perform educational programs for parents and footwear manufacturers on the awareness of the situation for better public foot health. Exploring the foot size and shape within this age range of 6-15 years, will help improve interaction between users and practitioners thereby contributing to better foot health in children. Also, this idea should be further explored by other inclusive studies on varying populations and age groups.
The authors would like to acknowledge the financial support provided by The Technology Agency of the Czech Republic (TACR) project No: TJ1000142.
Conceptualization, methodology and investigation, P.B., T.U.; formal analysis and data curation, Z.B., M.C., J.B.; writing-original draft preparation, P.B., T.U.; writing-review and editing, F.A.N., J.P., T.S. All authors have read and approved the final version of the manuscript.
All data analysed during this study are included in this published article.
Prior to the execution of the project, which primarily concerns human subject personal data processing, the study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee for Research of Tomas Bata University in Zlin (Czech Republic).
Informed consent was obtained from parent or legal tutor for children involved in the study. Written informed consent has been obtained from the parent or legal tutor to publish this paper.
The data presented in this study are available on request from the corresponding author.
The authors declare no conflict of interest.
Footwear Research Centre, University Institute, Tomas Bata University in Zlin, Nad Ovcirnou IV, 3685, Zlin, Czech Republic.