Isolated acute anterior tibial (AT) tendon rupture is rare and can be missed, resulting in significant functional deformity of the affected limb. Early surgical treatment can improve functional patient outcomes, familiarity with patient presentation, including a history of ankle pain and swelling after hyper-plantar flexion and signs of a palpable dell and weak dorsiflexory strength at the ankle, and prompt confirmation with MRI are crucial. Here we report a patient who had an isolated acute AT tendon rupture that was surgically repaired with tenodesis and graft augmentation just 10 days post injury and had full restoration of power to the AT tendon by 15 weeks.
Anterior tibial tendon rupture, Tendinopathy, Tenodesis, Suture anchor
Isolated, closed anterior tibial (AT) tendon ruptures are rare. The typical patient is an elderly individual without a history of acute, traumatic injury. However in some instances, patients may recall a precipitating event prior to rupture, such as a popping sensation and development of acute swelling and pain, such as described in this case report [1,2]. This mechanism is more common in younger patients with a high activity level or following trauma [3]. The common sequelae of AT tendon ruptures include foot drop, flatfoot, and Achilles tendon contracture [1]. With a rupture of the AT tendon, up to 80% of dorsiflexory power at the ankle is eliminated [4]. The lack of dorsiflexion from the AT tendon may also lead to the recruitment of extensor hallucis longus and extensor digitorum longus tendons, which compensate with extensor substitution, resulting in deformities such as claw toes and hammertoes [1].
Management of AT ruptures relies on early diagnosis through clinical findings, including anterior ankle pain and swelling, palpation of fixed soft tissue mass representing the tendon contracture, and marked decrease in dorsiflexory power at the ankle. Imaging modalities like ultrasonography and MRI are helpful to identify incomplete tears and ruptures. Ultimately, the decision between conservative versus surgical treatment must be considered based on a combination of factors, including the length of tendon deficit, age of the patient, presence of comorbidities, functional status, and chronicity of the injury [3]. It is generally accepted that operative treatment is preferred for patients who are good surgical candidates and want to maintain a high functional level [5]. On the other hand, functionally low-demand patients with advanced age may benefit from conservative treatment with ankle-foot orthosis (AFO) and physical therapy [1,3].
A 60-year-old male presented with complaints of pain and swelling to the anterior aspect of his left ankle, one day after attempting to stand up from a kneeling position on the ground. After his foot was forced into hyper-plantarflexion, he heard an audible snap and then experienced acute pain. Immediately after the injury, he was able to bear weight on his left lower extremity, but could not walk more than a few steps, and had weakness of the left lower leg and ankle. The patient denied use of local or systemic corticosteroids, and fluoroquinolone antibiotics, such as ciprofloxacin, which are medications associated with tendon tears. There was also no history or evidence for diabetes mellitus, hyperlipidemia, hyperparathyroidism, or renal disease.
Clinical examination demonstrated tenderness to palpation at the anterior ankle, dorsum of foot, and distal third of the leg. There was a palpable dell located at the anterior ankle joint which followed the course of the AT tendon 4 cm distally to the dorsum of the foot and matched the consistency of the tendon. There was no palpable soft tissue mass or swelling proximal to the ankle. There were areas of patchy ecchymosis overlying the medial plantar aspect of the foot. Motor strength was graded 0/5 for the AT tendon and 4/5 for the extensor digitorum longus and extensor hallucis longus tendons. The patient demonstrated an antalgic, steppage gait. There were no extension contractures of the digits. There were no neurologic or vascular deficits.
The patient had a 3 Telsa MRI of his ankle 3 days after the injury. The MRI demonstrated marked thickening, presumably due to the presence of hemorrhagic products, and extensive partial thickness tearing of the distal AT tendon (Figure 1). Specifically, there was complete rupture of the fibers of the AT tendon inserting onto the base of the first metatarsal approximately 2 cm proximal to their insertion, and extensive partial thickness tear of the fibers inserting onto the medial cuneiform, approximately 3.5 cm proximal to their insertion.
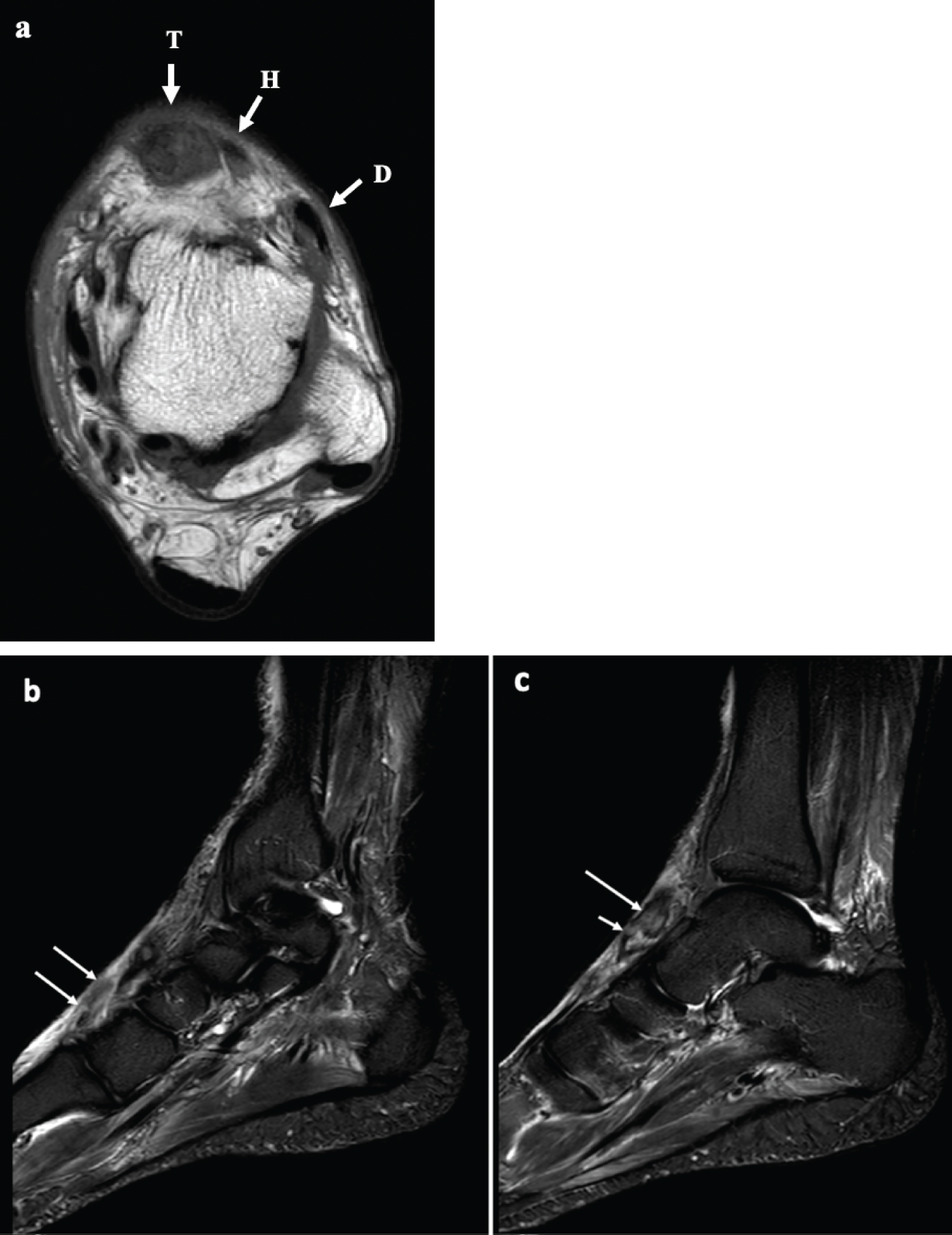 Figure 1: (A) Axial T1 image of the left ankle demonstrates a markedly enlarged, thickened and heterogeneous anterior tibial tendon (T). For comparison, the adjacent intact extensor hallucis tendon (H) and the more laterally located extensor digitorum tendon (D) are normal in size and appear black; (B) The Sagittal STIR images of the ankle demonstrate complete rupture of the fibers of the anterior tibial tendon inserting onto the base of the first metatarsal, approximately 2 cm from their insertion, with only the distal 2 cm of the tendon fibers visualized (arrows), and discontinuous from the more proximal fibers; (C) More proximally, there is extensive partial thickness tearing of the fibers inserting onto the medial cuneiform, with only a few superficial fibers seen intact (short arrow). The adjacent tendon fibers proximal to the site of the partial thickness tear is thickened and contains intrasubstance signal abnormality (long arrow). View Figure 1
Figure 1: (A) Axial T1 image of the left ankle demonstrates a markedly enlarged, thickened and heterogeneous anterior tibial tendon (T). For comparison, the adjacent intact extensor hallucis tendon (H) and the more laterally located extensor digitorum tendon (D) are normal in size and appear black; (B) The Sagittal STIR images of the ankle demonstrate complete rupture of the fibers of the anterior tibial tendon inserting onto the base of the first metatarsal, approximately 2 cm from their insertion, with only the distal 2 cm of the tendon fibers visualized (arrows), and discontinuous from the more proximal fibers; (C) More proximally, there is extensive partial thickness tearing of the fibers inserting onto the medial cuneiform, with only a few superficial fibers seen intact (short arrow). The adjacent tendon fibers proximal to the site of the partial thickness tear is thickened and contains intrasubstance signal abnormality (long arrow). View Figure 1
The patient underwent a successful primary repair of the anterior tibial tendon 10 days after his injury, including tenodesis with bioresorbable Sonic Anchor and augmentation with Graft Jacket. Intraoperative findings included complete rupture of the tendon approximately 2 cm from the base of the first metatarsal, with fraying of the split ends and remnant hematoma at the proximal end (Figure 2). Following operative repair, the patient was able to achieve full restoration of power to the anterior tibial tendon at 15 weeks post-operatively.
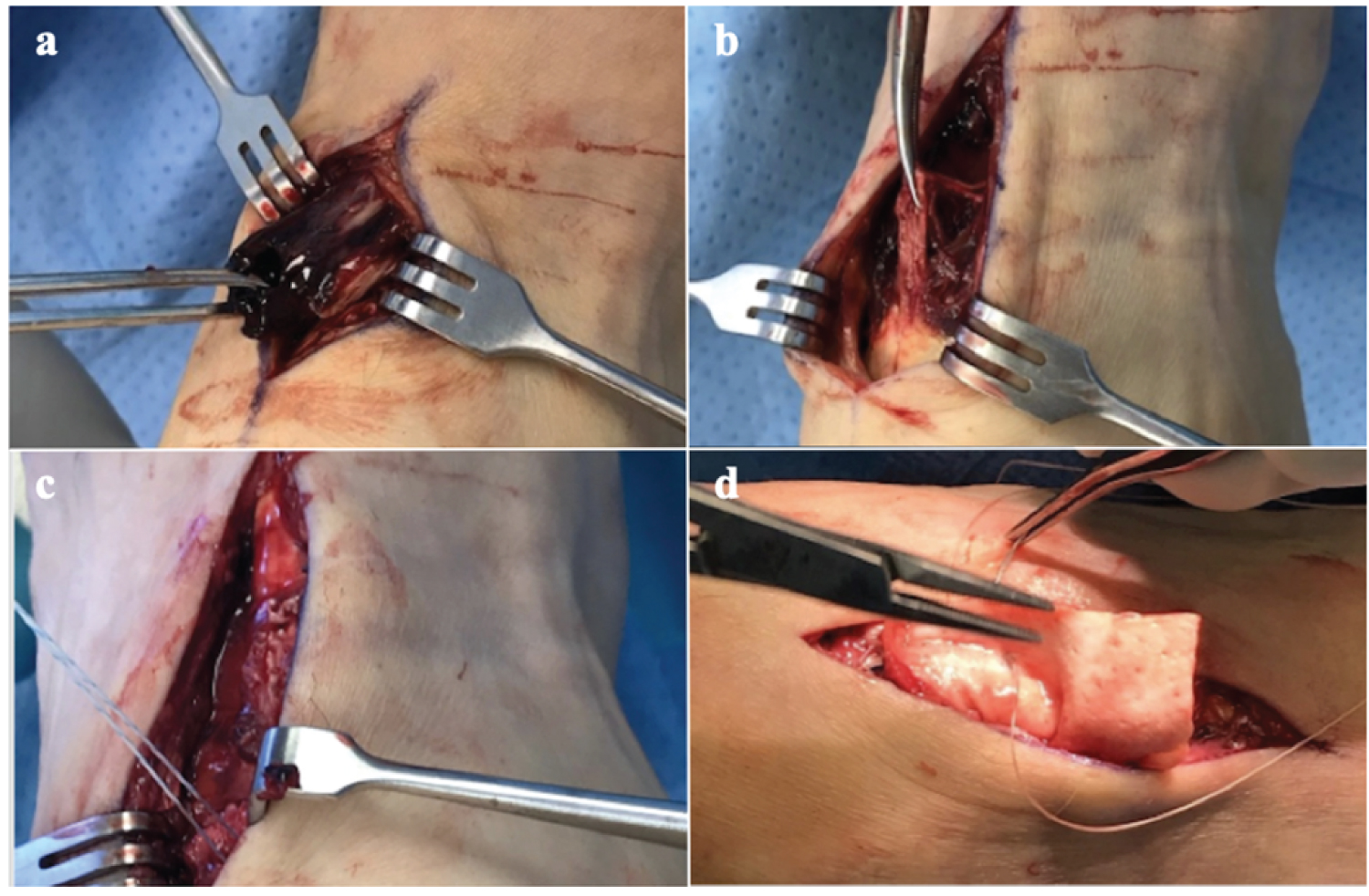 Figure 2: Operative identification of hematoma (a) and rupture of the AT tendon (b), followed by debridement and surgical repair using modified Krackow technique and tenodesis with Sonic Anchors (c) and augmentation with Graft Jacket (d). View Figure 2
Figure 2: Operative identification of hematoma (a) and rupture of the AT tendon (b), followed by debridement and surgical repair using modified Krackow technique and tenodesis with Sonic Anchors (c) and augmentation with Graft Jacket (d). View Figure 2
Anterior tibial tendon ruptures are rare and often a missed diagnosis. There have been only a few cases and series reported in literature. In one series, the average time from injury to diagnosis of an anterior tibial tendon rupture was 71 days [5]. This case report demonstrates the clinical presentation, imaging and physical exam findings that lead to the diagnosis of an AT tendon rupture in one patient.
The most common presentation is closed spontaneous rupture occurring in males in the 6th or 7th decade of life [6-8]. Ouzounian and Anderson have identified two patterns of ruptures in their series of 12 patients with anterior tibial tendon ruptures based on clinical presentation. The first presentation is atraumatic, occurring in low-functioning elderly adults, who present with several months of minor gait disturbance. The second presentation is acute traumatic, occurring in patients with a higher functional level, who experience a short period of acute pain and seek medical attention sooner [9]. In a systematic review of 155 cases, Tickner, et al. identified that acute traumatic rupture accounted for only 20% of cases [8].
The mechanism of action is most commonly supination of the foot and abrupt plantarflexion against resistance [2-4].
Conditions that have been associated with spontaneous rupture include diabetes mellitus, inflammatory arthritis, SLE, hyperparathyroidism, local or systemic steroid therapy, rheumatoid arthritis, psoriasis, and deposition of gout tophi [2,3,5,7,9-11]. Anagnostakos, et al. reported a case of a AT tendon rupture in a 71-year-old female who had been treated with cortisone injection 4 months prior and developed increased slapping of the foot and swelling with no antecedent trauma [2].
The clinical findings associated with AT ruptures include a palpable defect or proximal tendon stump along the course of the AT tendon and acute pain and swelling over the anterior side of the ankle [2,5,9]. Patients may experience chronic pain over the medial side of the foot. Gait disturbances may occur from dorsiflexion and inversion weakness, resulting in slapping of the foot, steppage gait or toe dragging [2,5,9]. In order to compensate for the weak dorsiflexion of the ankle, the extensor hallucis longus and extensor digitorum longus are recruited, which results in hyperextension of the toes [10].
Sammarco, et al. summarize their clinical findings in a series of 22 patients that was diagnostic for AT ruptures as a classic triad: 1) Pseudotumor of the ruptured tendon, 2) Loss of the normal contour of the tendon, 3) And weak dorsiflexion of the ankle accompanied by hyperextension of all the toes [10].
Radiographs may be used to exclude osseus pathology, but have low utility in the diagnosis of AT ruptures. Ultrasound may confirm tendon tear, but reliability varies with the experience of the examiner [2]. MRI remains the mainstay of imaging modalities to evaluate the extent of tendon tear (partial vs. complete), the precise location of the tear, and the length of tendon deficit or retracted stump ends, and should be obtained as soon as possible [2]. MRI can be particularly useful for surgical planning, such as when the peroneus tertius or plantaris tendons must be identified and harvested as a graft for the reconstruction of the AT [10].
Isolated anterior tibial tendon ruptures are rare and are often a missed diagnosis that presents late to the surgeon, which can make repair difficult. Prompt recognition of the key clinical findings associated with AT tears both in acute and chronic cases and prompt surgical repair, as in this case, can improve functional outcomes for the patient.
The authors have no conflicts of interest to declare and have received no financial support for the work.