Background: Plantar fascia taping is a common conservative treatment method used to treat plantar fasciitis, or plantar heel pain. Clinical taping methods (e.g., Low-Dye and calcaneal) have been shown to be effective in reducing plantar heel pain, but their application is laborious and generally not self-applied. The growth of retail home-based kinesiology tape products has created an opportunity to improve the use of taping in the clinical and home settings. The purpose of this study was to evaluate the effectiveness of a novel plantar fascia kinesiology taping method in reducing plantar heel pain. We hypothesized that this taping method, called Functional Anatomic Support Taping (FAST), would reduce plantar heel pain in a manner similar to existing taping methods while being easily self-applied at home.
Methods: A total of 151 patients being treated in 3 Private podiatry clinics were recruited for the study and allocated to four different treatment groups: 1) A small baseline group was taped with Low-Dye taping (LDT, n = 10), 2) one group received the FAST method of taping (n = 54), 3) One group received a cortisone injection with the FAST method (FAST+, n =75), and 4) the last group received only a cortisone injection (CORT, n = 39). The patients returned 3 weeks later and answered a written questionnaire focusing on pain levels (100-point VAS scale) and the patients' experience on self-applying the tape at home. Pain levels were compared across three time points using a 4 × 3 mixed model ANOVA.
Results: All groups experienced a significant reduction in heel pain (p < 0.001) at both 24 hours and 2 weeks. In addition, there was a significant group x time interaction (p < 0.001), where the LDT pain scores rose slightly while all other groups dropped slightly between 24 hours and 2 weeks. At 2 weeks, the FAST+ group showed the greatest reduction (67.5%), followed by the FAST (55.1%) and CORT (54.4%) groups, with LDT the least (36.5%).
Conclusion: In this study we present a new method for taping the plantar fascia using kinesiology tape for the reduction of plantar fasciitis/heel pain. This novel tape is designed to be easily applied in the office or self-applied at home. This study shows the FAST tape is effective and reliable in diminishing plantar heel pain. The FAST method is as effective as Low-Dye Taping with the advantage that it can be self-applied.
Plantar proximal heel pain, or Plantar Fasciitis (PF), is a pathology that affects millions of men and women every year [1] PF is a condition of chronic inflammation of the origin of the plantar fascia. Diagnosis is based on clinical evaluation with the most common symptoms being pain at the plantar medial aspect of the calcaneus, and post-static dyskinesia. Onset of the pathology of PF can occur at any age but is most common in overweight persons with a sedentary lifestyle from ages 40 to 60 [2]. Even though PF is more common among the sedentary population, it can affect any individual including those with a more active lifestyle [2,3]. In fact, it is one of the most common pathologies seen in athletes with active runners comprising 76% of those affected athletes [4]. In the US, it has been reported that over 2 million patients are treated in the outpatient setting every year for acute PF [5]. Plantar heel pain is also reported to be the most common lower extremity pathology encountered by Foot and Ankle Surgeons [6-10]. Statistics show that 11-15% of adult patients seeking medical attention from a podiatric physician will present with a chief complaint of plantar proximal heel pain [11]. Some of the common treatment options used by physicians for PF include corticosteroid injections, orthotics, stretching, physical therapy, and plantar foot taping. These conservative treatment options have been shown to improve heel pain associated with PF in 90% of patients [12-14]. A few studies have reported that the most effective of these treatment options is mechanical control of foot, i.e., orthosis and taping [15,16].
One of these taping methods, called Low Dye Taping (LDT), has become a mainstay for initial treatment of plantar heel pain for many lower extremity and sports medicine providers. The LDT method for treatment of plantar fasciitis was originally described by Ralph W. Dye DSC in 1939 and has changed very little since that time [17]. Several scientific articles have evaluated Low Dye taping to understand its effect on the biomechanical function of the lower extremity and found it effective in short term symptom reduction of heel pain while awaiting long term management from other treatment options such as custom orthosis [12,18,19]. LDT reduces pain by effectively reducing overpronation, relieving tension within the plantar fascia [16,20,21]. Podolsky & Kalichman, relate that a standard LDT takes around 10 minutes to apply in order to provide immediate relief for heel pain [22], but Chen, et al. related that the process of applying LDT is inconsistent between different specialists because there is no uniform method to apply LDT [23]. However, LDT is difficult to self-apply at home because the method requires various strips of athletic tape and knowledge of the complicated application process.
The advent of retail home-based kinesiology tape products has created an opportunity to improve the use of taping in the clinical and home settings. As these taping methods have become common, there has been a significant increase in the variety of taping methods used for common conditions such as plantar heel pain [24-27]. However, a major concern with the emergence of home-based taping is the diversity of taping methods, most of which have not undergone clinical testing. In this study we present a novel method for consistently taping the plantar foot using kinesiology tape and evaluate its effectiveness in reducing plantar heel pain. We hypothesized that this taping method would reduce plantar heel pain in a manner similar to LDT.
A novel taping method for plantar heel pain, which we termed functional anatomic support taping (FAST) was created using KT Tape brand pro-extreme tape (KT Health, American Fork Utah USA). The tape design was created by cutting large sheets of KT tape into a design that consists of a single unit of tape in the shape of the letter "t" with a wider forefoot section, two angled side strips, and a narrow section at the plantar heel (Figure 1). The final pattern was 7 cm wide at the distal end (forefoot), 5 cm wide at the proximal end (heel), and 22 cm in length. At 10 cm from the distal end (forefoot) is the central point of the "t" where the side (wings) support strips are angled at 70 degrees and are 8 cm long from the central point.
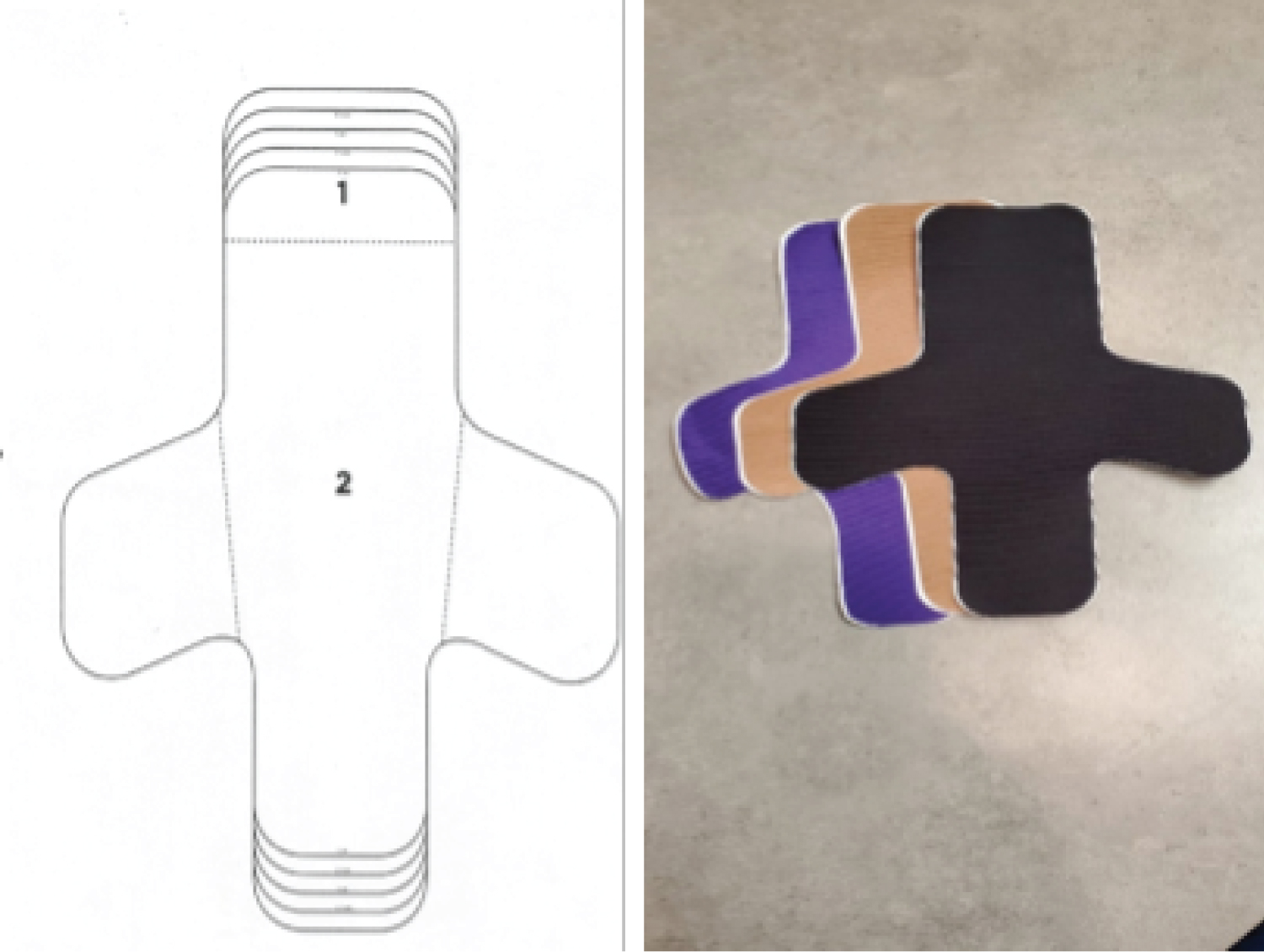 Figure 1: FAST design (1) indicates the forefoot section of the tape backing and; (2) is the main body of the tape. To help with application sequencing, perforated lines were created as tear strips (dashed lines), while guidelines were printed for cutting the tape for smaller foot sizes (curved lines at the top and bottom). View Figure 1
Figure 1: FAST design (1) indicates the forefoot section of the tape backing and; (2) is the main body of the tape. To help with application sequencing, perforated lines were created as tear strips (dashed lines), while guidelines were printed for cutting the tape for smaller foot sizes (curved lines at the top and bottom). View Figure 1
The primary body of the tape is applied to the plantar foot from the forefoot to the heel. The medial side strip ends near the anterior-inferior aspect of the medial malleolus, overlying the apical insertion of the flexor retinaculum. The lateral side strip ends over the dorsal lateral foot overlying the distal segment of the extensor retinaculum. The primary length of the tape covers the plantar foot with the side wings applied at the medial arch and lateral midfoot. The tape is applied in sequence, with the forefoot section being applied first, aligning the tape along the foot's long axis. The side wings are applied last (Figure 2).
 Figure 2: Two pieces of FAST tape applied to the foot bilaterally with four angles showing where the tape is positioned on the various aspects of the foot. View Figure 2
Figure 2: Two pieces of FAST tape applied to the foot bilaterally with four angles showing where the tape is positioned on the various aspects of the foot. View Figure 2
In order to be effective, the tape was designed with M/L elasticity and longitudinal inelasticity as opposed to typical kinesiology tape strips, which only stretch along their length. By using a static tape from heel to toe, the tape reduces strain or stretching deformation along the plantar fascia, while M/L elasticity allows the side strip along the medial arch to provide dynamic/elastic support to the medial arch in parallel with the pull of the PT tendon.
Clinical testing was performed by 3 Podiatric physicians in 2 separate clinical offices. From January 2019 to December 2020, patients seen in the office of Canyon Foot and Ankle in Spanish Fork, Utah, USA diagnosed with plantar fasciitis were invited to participate in this study. In addition, patients diagnosed with plantar fasciitis from May 2019 to December 2019 at the Foot Care Center, in, Billings, Montana, USA, were also invited to participate. Patients were diagnosed with PF based on clinical symptoms consisting of: pain located at the plantar medial heel during weight bearing, pain on palpation at the plantar medial aspect of the heel, post-static dyskinesia, duration of pain, and pain level. Exclusion criteria included patients with more than one diagnosis or a secondary lower extremity pathology at presentation, patients with a positive Tinnel's sign, or history of tarsal tunnel.
This study was designed around the need to treat each patient with best clinical practices; thus, a full controlled, randomized trial was outside the scope of this work. Instead, patients were divided into four treatment groups based on symptom severity and associated research team preferred treatment protocols. Each participating provider was asked to continue routine treatment protocols for patients diagnosed with plantar fasciitis using the FAST method in place of their typical Low Dye taping. The groups were: 1) Patients who received a cortisone injection and were taped with the FAST method (FAST+); 2) Patients who were treated with the FAST method only (FAST); 3) Patients receiving only a cortisone injection (CORT); 4) Patients receiving Low Dye taping (LDT). According to office protocols, patients with a pain level of 8-10/10 (on a self-determined visual analog pain scale) were treated with a cortisone injection and FAST. Patients with a pain level of 6-7/10 were treated with cortisone injection and patients with a pain level below 6/10 were treated with FAST. In order to create a small control group, 10 patients were selected at random during the first 3 months of the study to receive LDT.
Prior to clinical testing each physician was educated on how to apply the FAST method to the patient's foot. Each physician was able to demonstrate consistent application of the tape to insure consistency. In order to ensure further consistency, the specific method for Low Dye taping was discussed in detail and agreed upon among the physicians (Figure 3).
 Figure 3: Low Dye taping applied to the foot using 1-inch strips of white sports tape. The first strip of tape is applied with no tension circumferentially around the forefoot just at the metatarsal heads. The next piece of tape is applied along the glabrous junction starting at the 5th metatarsal and ending at the 1st metatarsal. 3-4 strips of tape are applied in a similar fashion with each strip overlapping the more distal strip by a half-inch each and ending with the last strip applied just distal to the ankle joint. View Figure 3
Figure 3: Low Dye taping applied to the foot using 1-inch strips of white sports tape. The first strip of tape is applied with no tension circumferentially around the forefoot just at the metatarsal heads. The next piece of tape is applied along the glabrous junction starting at the 5th metatarsal and ending at the 1st metatarsal. 3-4 strips of tape are applied in a similar fashion with each strip overlapping the more distal strip by a half-inch each and ending with the last strip applied just distal to the ankle joint. View Figure 3
Each patient in the CORT and FAST+ groups received a cortisone injection. The cortisone injections were given under sterile conditions and each patient was given a plantar heel injection from a medial approach at the level of the glabrous junction. Each cortisone injection consisted of a 2-cc total injection of 1 cc of 0.5% Marcaine plain and 0.5 cc of Kenalog 40 and 0.5 cc of Dexamethasone Phosphate 10 mg/mL.
Each patient in the FAST and FAST+ groups received a packet containing a welcome letter, clearly worded taping instructions, and 4 additional units of the FAST method tape for home application. The first unit of FAST method tape was applied by the clinician while educating the patient on how to apply the remaining 4 units at home, every 3-5 days. Each patient was instructed to use the tape for 2 weeks total. A simply worded questionnaire was taken by the patients in all 4 treatment groups at a 3 week follow up appointment. The questionnaire included basic demographics questions including name, date, age, height, and weight. The questionnaire then asked about the patient's pain level at the time of the appointment, 24 hours later and after 2 weeks of taping. Pain related questions utilized a 100-point visual analog pain scale (VAS). Lastly, four Likert scale questions (see Table 1 in results) were used to evaluate each participants' experience using their assigned treatment method. Likert scale questions were on a scale of 1-5 with 1 indicating an answer of strongly disagree and a 5 indicating a response of strongly agree.
Table 1: The 4 different Likert Questions on the 3 week follow up questionnaire and the mean values of the responses from the 4 treatment groups using the scale of 1-5: 1-Strongly disagree, 2-Somewhat disagree, 3- Neutral, 4-Somewhat agree, 5-Strongly agree. In the CORT group the final Likert question was removed from the questionnaire, as it was not relevant. View Table 1
Pain scores were compared among the four groups and across the three measurement times using a 4 × 3 mixed model ANOVA (α = 0.05). Holme post-hoc tests were used for pairwise comparisons when significant main effects were found. Likert question answers were evaluated only descriptively to add context to the pain results and treatment comparisons.
200 participants were recruited through an initial office visit and treatment. A total of 151 participants continued through follow up and study completion (102 females and 49 males, Table 2). There were 49 people who did not complete the study and were excluded from the patient total and statistical analysis. Most of these were excluded due to not returning for their 3 week follow up appointment at the office or not continuing with the FAST taping method as instructed. Three patients discontinued the taping due to allergic dermatitis. All three were treated with hydrocortisone 1% topical cream and the dermatitis resolved without further treatment.
Table 2: Patient demographics among the 4 groups with N representing the number of feet treated versus number of subjects in parenthesis and the group's mean ± standard deviation age, height, and mass. View Table 2
For pain scores (Table 3 and Figure 4), significant main effects were found for time (p < 0.001) and group × time interactions (p < 0.001), but not for group (p = 0.08). Pairwise comparisons showed time differences between baseline and 24 hours (p < 0.001) as well as between baseline and 2 weeks (p < 0.001), but not between 24 hours and 2 weeks (p = 0.253). However, the main effect group × time interaction was visible when comparing LDT to the other three groups, as mean LDT pain scores rose slightly while all other groups dropped slightly.
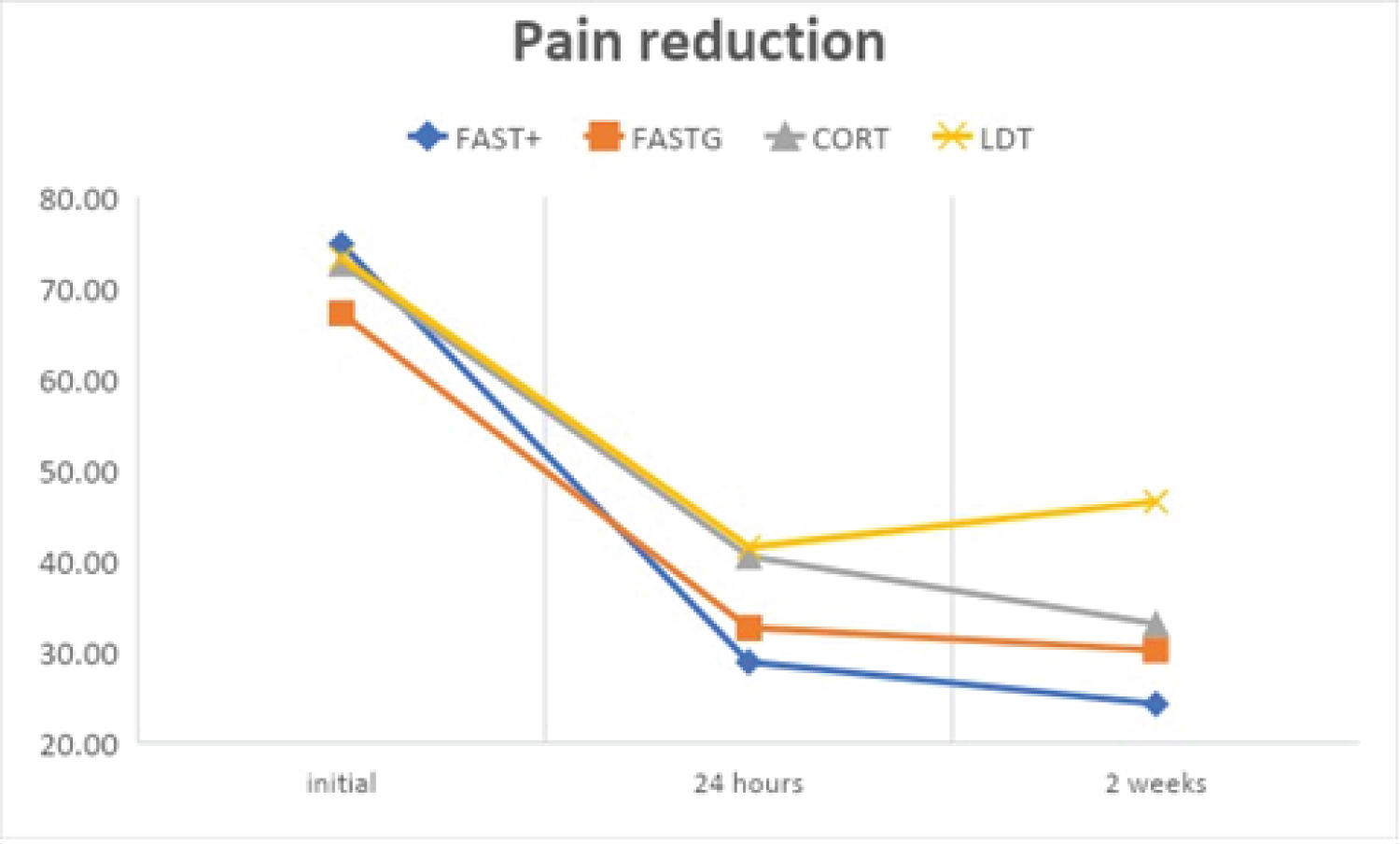 Figure 4: The change in the average pain level as self-reported by the subjects using the Visual Analog scale of 1-100 among the 4 different groups over the total time period of the study. The 3 different values were recorded by the subject from the follow up questionnaire during the 3 week follow up visit. View Figure 4
Figure 4: The change in the average pain level as self-reported by the subjects using the Visual Analog scale of 1-100 among the 4 different groups over the total time period of the study. The 3 different values were recorded by the subject from the follow up questionnaire during the 3 week follow up visit. View Figure 4
Table 3: The averaged pain value plus or minus the standard deviation among the 4 groups at the 3 different times as self-reported on the follow up questionnaire using the Visual Analog pain scale of 1-100. View Table 3
Mean Likert scores ranged from 3.2 to 4.6 (Table 1). The LDT group reported the lowest mean scores in all areas, while CORT, FAST, and FAST+ scores were fairly similar across questions. Of note, the FAST group had the highest scores on question 2 and 4, while CORT had the highest score on question 3.
In this study we described a new taping technique for plantar heel pain using kinesiology tape (FAST). Our hypothesis that this taping method would reduce plantar heel pain in a manner similar to LDT was supported by our pain results. All four groups exhibited reduction in pain, with some subtle differences among the groups. Unsurprisingly, the FAST+ group had the greatest reduction in pain across the 2-week period (67.5% reduction in pain), since it combined two treatments. Interestingly, the percentage of pain reduction was similar in the FAST group (55.1%) to the CORT group (54.4%). We originally expected the CORT group to have a higher reduction in pain compared to all taping methods based on previous research [28,29]. The pain reduction in the FAST group may be comparable in this study in part because the baseline pain level was slightly lower. In addition, the FAST group may have had a higher perceived reduction of pain due to the feeling that they had more control over this treatment method. For instance, studies on pain management have shown that patient-controlled pain management results in similar pain reduction when compared to provider control, but with less medication [30,31]. The LDT and FAST taping groups had similar reductions in pain at 24 hours; however, in the LDT group pain rose slightly between 24 hours and 2 weeks, while the FAST group dropped slightly. While some of this discrepancy may be influenced by the low LDT subject numbers and study methodology, compliance could also be a factor. In our study, LDT was only applied at the baseline visit and patients were advised to leave the tape on for up to a week. For the FAST group, the patients re-applied the tape every 3-5 days.
There are several potential benefits of the FAST tape design, particularly when compared to LDT. LDT has been shown to be effective for reducing plantar heel pain by amounts similar to that in our study [18,29]. For instance, Landorf, et al. exhibited an ANCOVA adjusted improvement of 31.7 points on a VAS scale, comparable to our 32.1 initial improvement relative to baseline. However, its application is complicated and generally needs to be performed in the clinic. FAST simplifies the application by having only one strip of pre-cut tape that can be applied by the patient at home. In addition, we estimated application time to be under 1 minute, while LDT can take 3-5 minutes. FAST application time was estimated during preclinical testing, where 50 applications were performed and timed. Three clinicians and two medical assistants applied the FAST method 10 times each and the average time for self-application was 46 seconds for each unit of tape. The speed and simplicity of the FAST method may improve patient compliance and satisfaction in comparison to LDT or other taping methods.
Another consideration is the unique tape elastic properties. Kinesiology tape has traditionally been applied in longitudinally elastic strips. In the FAST tape design, we reversed this, choosing lateral elasticity with longitudinal inelasticity. We think that these tape properties may increase performance when compared to both LDT and kinesiology taping methods. While LDT beneficially reduces strain in the fascia, its inelasticity may also immobilize the transverse arch and overly reduce foot function. In contrast, longitudinally elastic kinesiology tape may alter proprioception and pain receptors but is unlikely to affect mechanics [24-27,32]. In addition, we feel that having a tape that is static in length makes it useful for a new type of anatomic function that will be suitable for many other body regions where bracing and supportive reinforcement are useful. For instance, we have used this tape for isolated clinical testing of mild Achilles tendonitis, and for support of lateral ankle ligament laxity with strong positive feedback from those patients. Additional research is needed to confirm these benefits.
The Likert scale questions were used primarily as a feedback tool relating to the design of the FAST taping. These questions are not clinically valid but do add some value to understanding the patient's perception of each treatment. The lower scores for the LDT group across all questions suggest lower overall satisfaction with this taping method compared to the other treatment options. It is interesting t note that the FAST group reported the highest scores on question 2. This could be due to the simplicity of use of the new taping method or to the patient attributing all improvement to a single self-administered treatment (e.g., "I would use the treatment again..."). Similarly, the higher score in the CORT group for question 3 might be due to the reliance on a medical professional for treatment (e.g., "I would recommend my doctor use this treatment..."). In question 4, we attempted to relate taping to orthoses use, which the patients may or may not have had much experience with. It is interesting that the FAST group had slightly higher scores here than FAST+. This could be due to chance, or perhaps due to the difficulty separating the effects of the tape from the cortisone in this combined treatment.
The most prominent limitation in this study is the lack of a control group that was either left untreated or treated with sham taping. Because this study was integrated into clinical practice, an untreated group was not desirable, since previous research has shown that plantar heel pain does not resolve if left untreated [18,29]. For example, Landorf, et al. showed a reduction in pain with LDT but an increase in pain in a non-treatment group [18]. Thus, although a clear limitation, positive results from each group suggest effective pain reduction that is likely beyond a placebo effect. Two related limitations involve the non-randomized group selections and the small LDT group. Both decisions were also made in the context of routine treatment. Treatment group selections were based on clinical treatment guidelines as previously presented. A larger LDT group may have been helpful, however, positive results were seen even with our small LDT group. A larger multi-site randomized control trial study design would be ideal to fully compare taping methods. Finally, our main measure of effectiveness is a subjective pain scale. While this is a common method to study treatment effects when pain is the main symptom, future studies should incorporate more objective outcome tools [29]. For example, instrumented gait analysis may provide measures of the mechanical effects of taping on walking or running movements.
Overall, the FAST method diminished pain associated with Plantar Fasciitis that was comparable to or exceeded other treatment options. It has the added benefit of being substantially easier to apply and wear for both the patient and provider. In addition, we believe that, unlike many taping methods, the FAST method increases patient efficacy and treatment duration by allowing the patient to administer treatment at home. Further analysis with a randomized control trial study will help to better understand the function of the FAST method in comparison with LDT and other treatment options for conservative treatment of plantar heel pain. This new taping method has the potential to considerably improve patient care in and out of the clinical setting.
The specific tape design used in this study is under patent pending status (application 17/006,551) with the potential for commercialization by the primary author.