This case report highlights a unique soft tissue entrapment in an open Metatarsophalangeal joint dislocation requiring operative reduction.
Metatarsophalangeal joint dislocation, Irreducible dislocation, Posttraumatic ankylosis
Metatarsophalangeal joint (MTP) dislocations are rare and complex injuries typically resulting from high energy trauma [1]. The mechanism of injury typically involves a forceful extension of the first MTP joint, resulting in subluxation and dislocation of the metatarsal head plantar to the phalanx base [2,3]. Adequate treatment is necessary to prevent long-term functional limitations given the biomechanical role of the first MTP complex in gait [4].
Reduction may be performed open or closed, depending on the direction of dislocation and involvement of soft tissue structures [3,5]. Complications including osteoarthritis, hallux rigidus, and sesamoid pseudoarthrosis have been previously described [5].
In this article, we report a case of an irreducible dorsal open dislocation of the first MTP joint. Intraoperatively, the metatarsal head was found to have split the medial and lateral heads of the flexor hallicus brevis (FHB) tendon requiring incision of the intersesamoid ligament for reduction.
A 39-year-old female presented to the emergency department as an unhelmeted motorcycle passenger who was ejected from the motorcycle following a head-on collision with an automobile. Concurrent injuries included non-displaced C3 fracture, multiple rib fractures, right-sided pneumothorax, right internal carotid artery dissection, right knee traumatic arthrotomy, and right elbow soft tissue injury.
The patient was administered tetanus, cephalexin, and tobramycin in the emergency department. Examination revealed a first MTP dislocation with protrusion of the metatarsal head through the plantar surface of the foot (Figure 1). No motor or sensory deficits were noted. Dislocation of the first MTP joint was confirmed radiographically (Figure 2) and via computed tomography (Figure 3), which also revealed a fracture of the second metatarsal head. Multiple reduction attempts under local anesthesia were performed and failed. The decision was made to proceed to the operating room for open reduction.
 Figure 1: Photograph of the right foot at the time of presentation to the emergency department demonstrating open, contaminated plantar dislocation of the first metatarsal phalangeal joint. View Figure 1
Figure 1: Photograph of the right foot at the time of presentation to the emergency department demonstrating open, contaminated plantar dislocation of the first metatarsal phalangeal joint. View Figure 1
 Figure 2: AP (A) and lateral (B) of the right foot demonstrating a dorsal first MTP dislocation with medial displacement of the first metatarsal, as well as fracture of the second metatarsal head. View Figure 2
Figure 2: AP (A) and lateral (B) of the right foot demonstrating a dorsal first MTP dislocation with medial displacement of the first metatarsal, as well as fracture of the second metatarsal head. View Figure 2
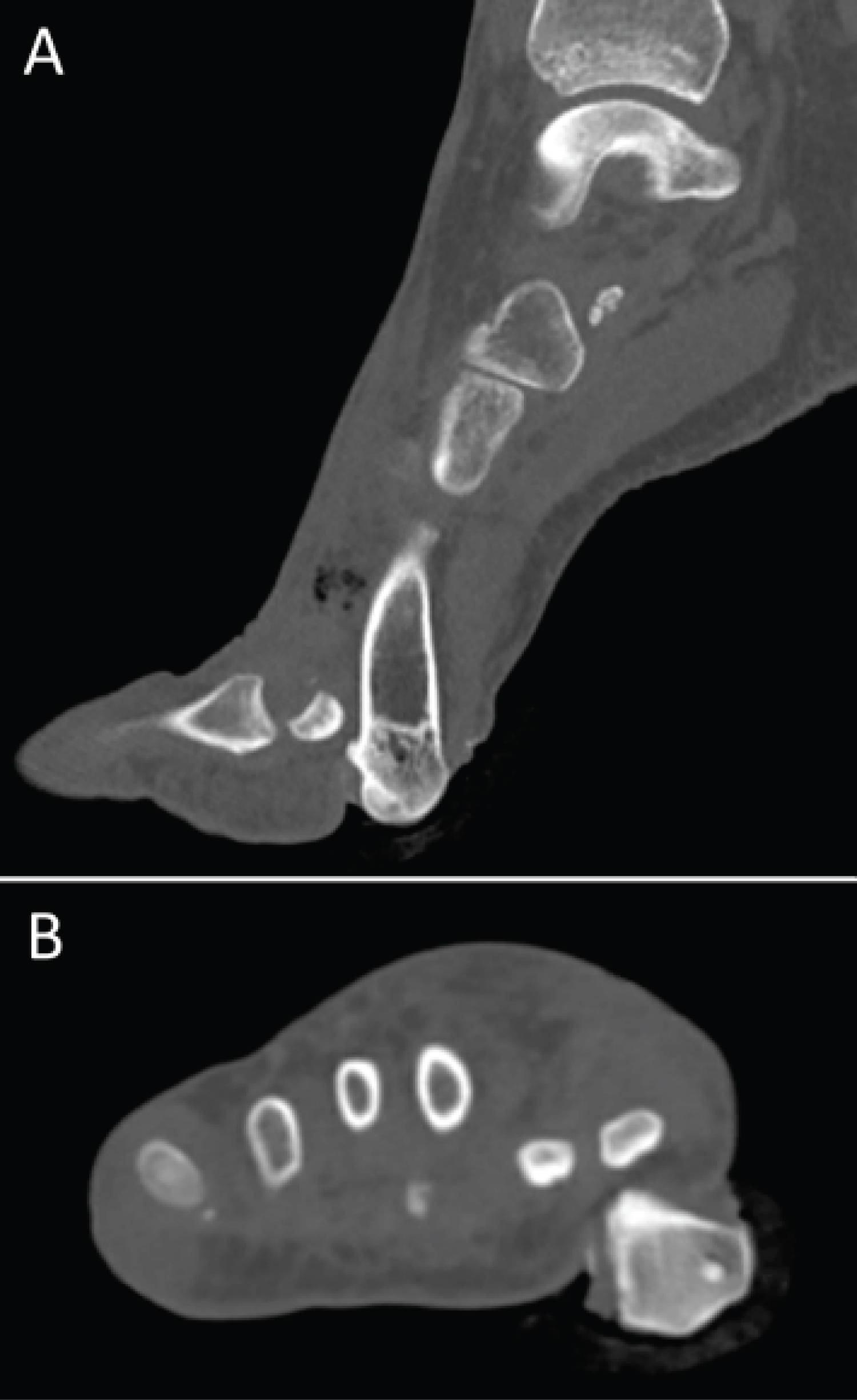 Figure 3: Sagittal (A) and Axial (B) computed tomography demonstrating the plantar first MTP dislocation. View Figure 3
Figure 3: Sagittal (A) and Axial (B) computed tomography demonstrating the plantar first MTP dislocation. View Figure 3
Intraoperatively, the plantar wound was observed to be grossly contaminated with debris. A scalpel and tenotomy scissor were used for sharp excision of devitalized and contaminated tissue. Application of axial traction did not result in reduction. The laceration was extended distally over the proximal phalanx to respect the plantar skin. The abductor hallucis was retracted dorsally, and the medial FHB tendon was observed to be acting as a noose around the metatarsal head (Figure 4). The FHB tendon was followed distally until the medial sesamoid was encountered, and the metatarsal head was found to have displaced through the medial and lateral limbs of the FHB tendon. Application of axial traction resulted in tendon tightening around the metatarsal head. The intersesamoid ligament was incised a few millimeters without full release. Reduction was obtained with axial traction and manipulation of the FHB tendons (Figure 5). Following reduction, the MTP joint was stable through range of motion. The wound was thoroughly irrigated and closed with interrupted 3-0 Nylon. Postoperatively, she was restricted to touch down weight bearing in the right lower extremity in a CAM boot and was ultimately discharged on postoperative day (POD) 10.
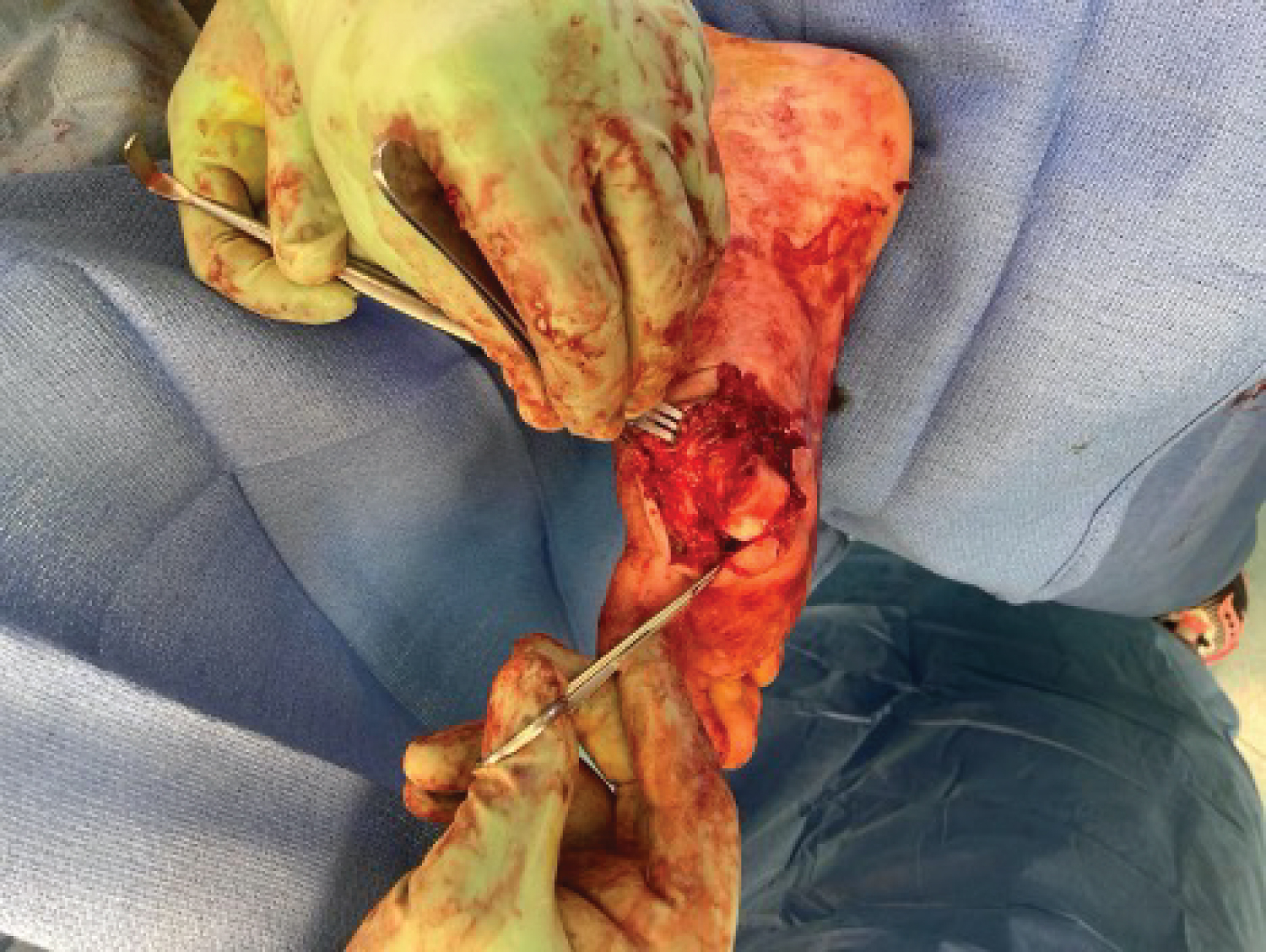 Figure 4: Intra-operative photograph demonstrating herniation of the first metatarsal through the flexor hallucis brevis muscle bellies. View Figure 4
Figure 4: Intra-operative photograph demonstrating herniation of the first metatarsal through the flexor hallucis brevis muscle bellies. View Figure 4
 Figure 5: Intra-operative fluoroscopic radiograph demonstrating concentric reduction of the first metatarsophalangeal joint and second metatarsal fracture. View Figure 5
Figure 5: Intra-operative fluoroscopic radiograph demonstrating concentric reduction of the first metatarsophalangeal joint and second metatarsal fracture. View Figure 5
The patient presented for follow-up on POD 24 with increased pain and persistent drainage from the surgical site. On exam, the incision appeared partially dehisced with surrounding necrotic tissue and scant purulent drainage. She was directly admitted and initiated on intravenous (IV) vancomycin and cefepime. She underwent irrigation and debridement with application of a negative pressure dressing on POD 25 and POD 28. The wound grew polymicrobial species, and the patient ultimately was managed with 6 weeks of cefepime and was subsequently transitioned to 6 weeks of oral levofloxacin.
She was followed in the outpatient setting for a prolonged wound healing course. Negative pressure wound therapy with a portable wound vacuum was used for one month following her last irrigation and debridement, and then wet to dry dressing changes were used through postoperative week 8. To protect the wound, the patient was made heel weightbearing until postoperative month four, when weightbearing in a stiff-soled shoe was initiated. At postoperative month seven, the incision was well-healed (Figure 6) and the patient had returned to her baseline function wearing normal shoes. The MTP joint was stable with interphalangeal motion limited to 15 degrees. Radiographs demonstrated progression to posttraumatic ankylosis (Figure 7).
 Figure 6: Photograph eight months postoperatively demonstrating the well-healed surgical site after negative pressure therapy followed by local wound care and healing by secondary intention. View Figure 6
Figure 6: Photograph eight months postoperatively demonstrating the well-healed surgical site after negative pressure therapy followed by local wound care and healing by secondary intention. View Figure 6
 Figure 7: Dorsoplantar (A) and lateral (B) radiographs of the foot eight months after injury demonstrating severe posttraumatic arthritis and essentially ankylosis of the first metatarsophalangeal joint. Posttraumatic changes of the second metatarsal head are evident. View Figure 7
Figure 7: Dorsoplantar (A) and lateral (B) radiographs of the foot eight months after injury demonstrating severe posttraumatic arthritis and essentially ankylosis of the first metatarsophalangeal joint. Posttraumatic changes of the second metatarsal head are evident. View Figure 7
This case highlights a unique soft tissue entrapment in an open MTP dislocation requiring operative reduction. In our particular patient, multiple reduction attempts were performed prior to surgery because the patient was initially deemed too unstable for surgery. At the time of surgery, the joint was explored through the traumatic plantar wound and ultimately required partial incision of the intersesamoid ligament for reduction.
Closed reduction amenability depends on the injury morphology. Zrig, et al. recently revised the classification system for first MTP dislocation [5]. Type I classifications describe dorsal dislocations. Types IA and IC are amenable to closed reduction due to non-dislocation of the sesamoidal complex; in Type IA the intersesamoid ligament is intact while in Type IC the intersesamoid ligament is torn or avulsed. In contrast, Type IB requires open reduction, and involves an intact intersesamoid ligament with a dislocated sesamoidal complex over the metatarsal neck. While the present case approximates a Type IB dislocation, to the authors' knowledge, tethering of the FHB about the metatarsal head has not been previously described. However, a similar mechanism has been described for the metacarpophalangeal joint, in which the metacarpal head can become ensnared within soft tissues and tendons.
In addition to structural entrapment, this case highlights the potential for post-operative wound breakdown in an open first MTP dislocation. The wound was closed primarily in this case, however, the initial soft tissue injury resulted in wound dehiscence and later infection that considerably prolonged this patient's recovery. Early recognition of the probability of wound complications may allow for more prompt treatment and management of patient expectations.
Although this patient's postoperative course was complicated by wound dehiscence and joint infection, the joint was adequately stabilized after closed reduction and she ultimately was able to return to preoperative activity level. We present this case to raise awareness of irreducible MTP dislocations with interposed flexor hallicus brevis tendon.
No disclosure information is applicable.
Each other lister contributed equally and critically to this manuscript.