Angioleiomyomas are benign soft-tissue tumors that are relatively rare and often occur in the extremities. This tumor has a predilection for middle-aged females. The true etiology is still largerly unkown. Clinical and radiological examinations are frequently nonspecific and ambiguous, as a result, they are rarely diagnosed preoperatively.
Simple excision and histopathology are the gold standard for the diagnosis.
The purpose of this case study presentation is to emphasize the importance of including angioleiomyoma in the differential diagnosis of foot and ankle soft-tissue masses.
Angioleiomyomas or Vascular angioleiomyomas are smooth muscle tumors that emerge from the tunica media of the subcutaneous blood vessels [1,2]. Angioleiomyomas are a type of leiomyoma that are assumed to be benign and have mesenchymal origins [3]. They may grow all over the body, but they usually affect the lower extremities and are relatively uncommon.
They are slow-growing masses that can be asymptomatic; as a result, their preoperative diagnosis is relatively rare [1-4]. This emphasizes how critical it is to further characterize the clinical diagnosis and management of angioleiomyomas in order to raise awareness of this pathology as a potential differential diagnosis for lower extremity soft tissue tumor [4].
A 47-years-old female presented with a chief complaint of a painful lesion on the anterior lateral side of her left ankle. The mass had been present for 2 years, and it progressively became larger in size. The mass was creating radiating pain up her leg with shoeing discomfort. Her medical history and general physical health were unremarkable.
Upon physical examination, a mobile, 2 cm dome-shaped and solid subcutaneous nodular mass was found. No transillumination was evident through the mass.
X-rays did not show any bone abnormalities (Figure 1).
 Figure 1: Foot X-Ray without ankle anomalies. View Figure 1
Figure 1: Foot X-Ray without ankle anomalies. View Figure 1
Ultrasounds results shows well-limited superficial ovoid subcutaneous nodule of the external side of the left ankle without septa or intralesional necrosis, hypervascularized by colour Doppler, evoking in first place a schwannoma (Figure 2 and Figure 3).
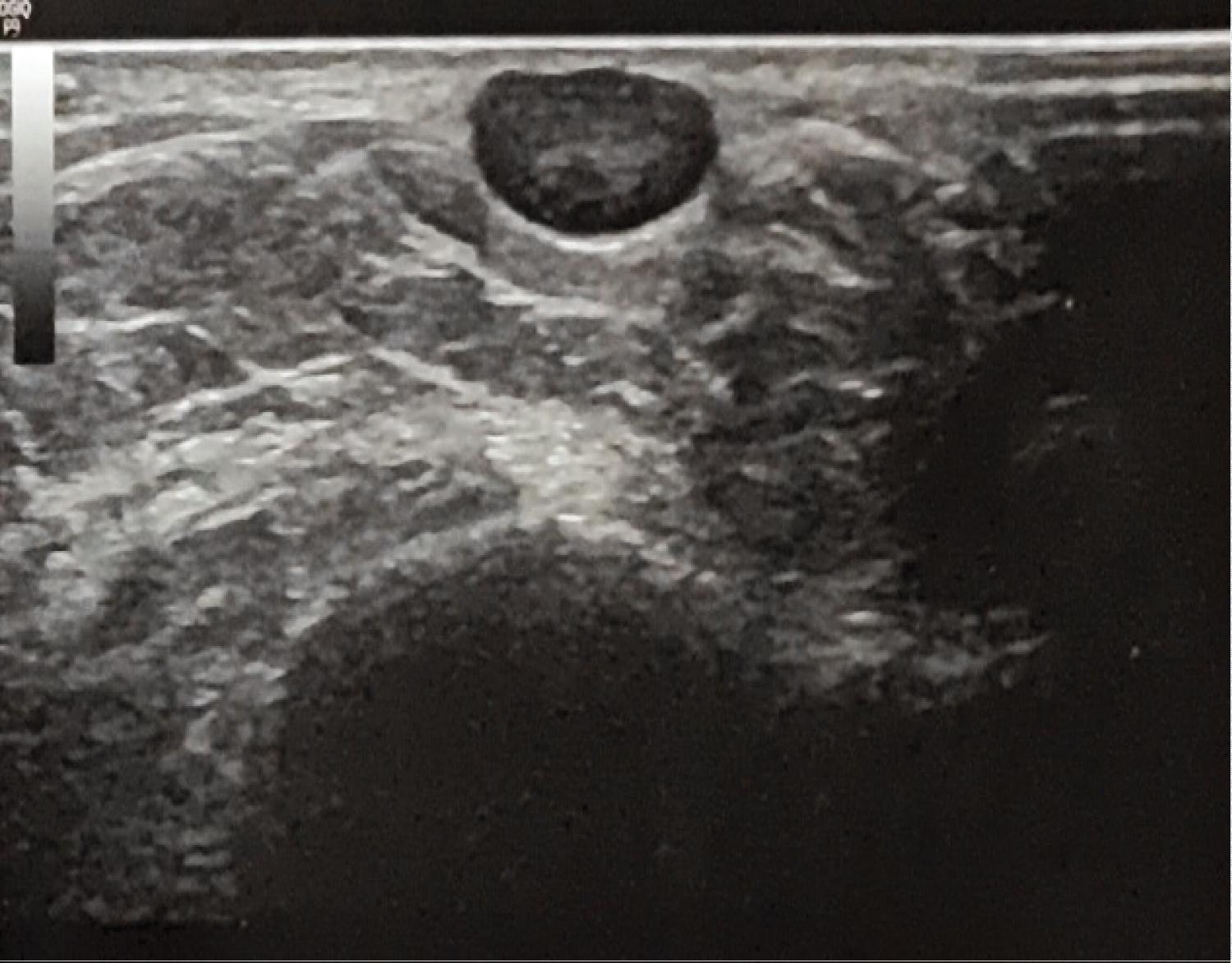 Figure 2: Subcutaneous ovoid structure with sharp and regular contours. Slightly heterogeneous hypoechoic aspect. View Figure 2
Figure 2: Subcutaneous ovoid structure with sharp and regular contours. Slightly heterogeneous hypoechoic aspect. View Figure 2
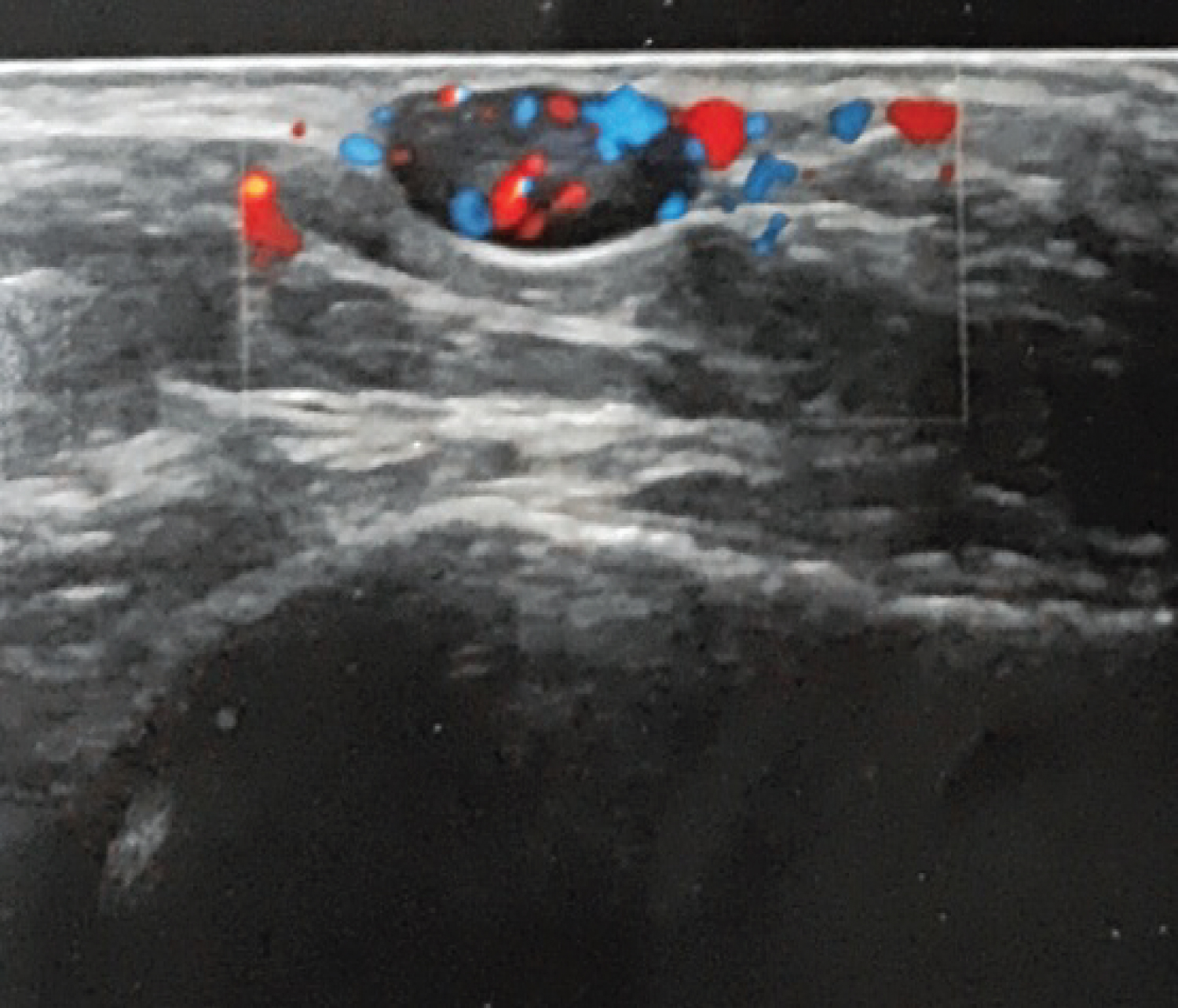 Figure 3: Significant peripheral and central vascularisation. View Figure 3
Figure 3: Significant peripheral and central vascularisation. View Figure 3
Considering the benignity of the clinical and radiological aspects, it was then recommended to perform a surgical excision and histopathological investigation.
The operative procedure was performed under local anaesthesia. Pneumatic tourniquet at the root of the limb was inflated to 300 mmhg during 15 minutes.
A 3-cm, oblique, external retro-malleolar, skin incision was made. Sharp and blunt dissection was used to dissect to the level of the mass. It was firm, yellow-tan in colour, and didn't seem to be expanding or invading surrounding features. The sural nerve was identified and protected.
The tumor was completely removed excised in toto. Meticulous haemostasis was ensured after deflating the tourniquet to prevent hematoma formation. The wound was flushed and closed with 4/0 prolene sutures.
The specimen was sent to pathology for both gross and microscopic examination.
The incision site was closed anatomically and a sterile dry compressive dressing was applied. The histopathology findings were consistent with a postoperative diagnosis of a benign angioleiomyoma (Figure 4).
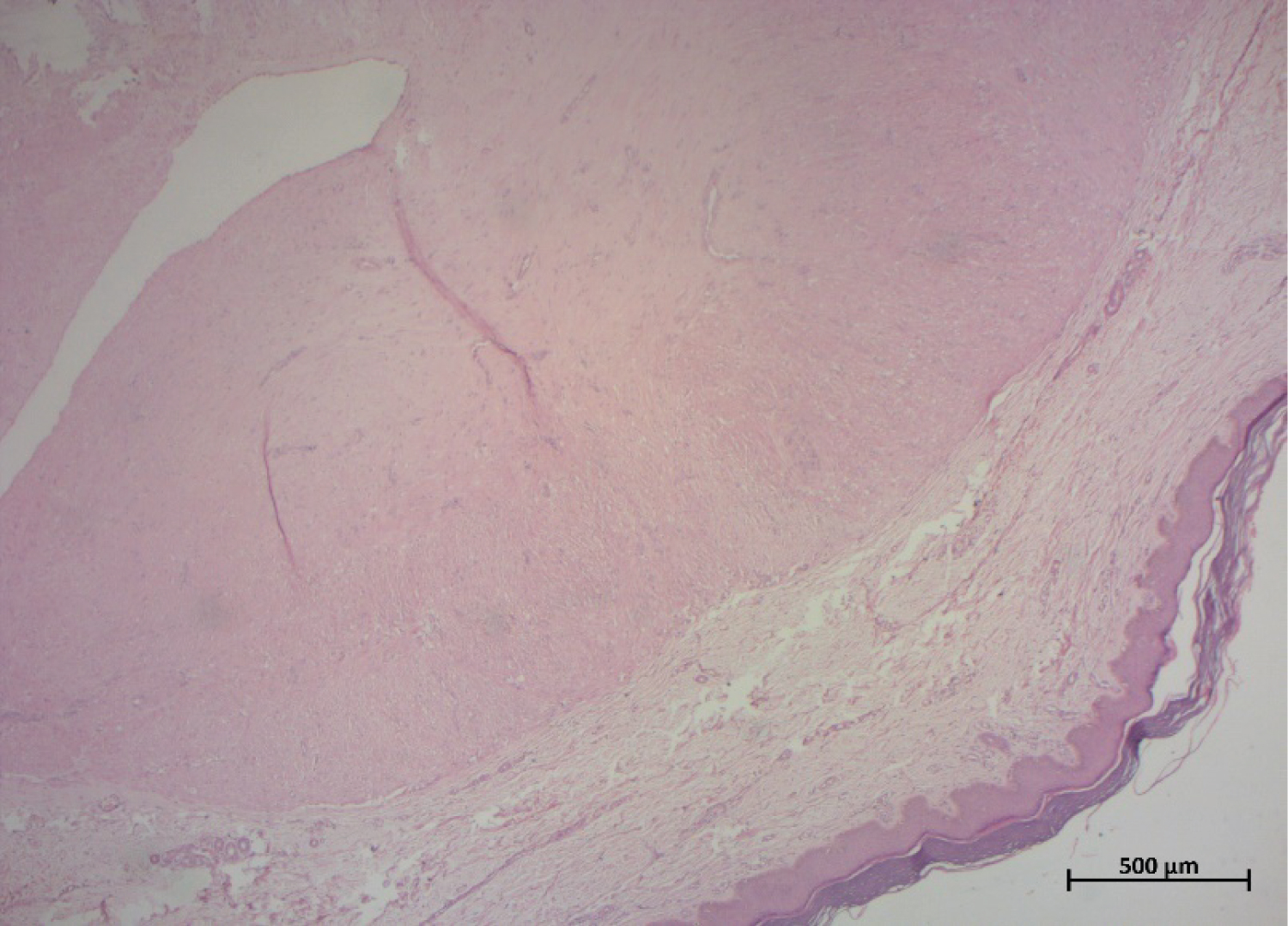 Figure 4: A well circumscribed nodule of the dermis showing interlacing bundles of smooth muscle cells which surround compressed vascular channels (HE x25). View Figure 4
Figure 4: A well circumscribed nodule of the dermis showing interlacing bundles of smooth muscle cells which surround compressed vascular channels (HE x25). View Figure 4
Postoperative healing was uncomplicated and there were nil symptoms or evidence of regrowth at 2 months review.
The pain was removed, the mobility of the ankle is complete and the sensibility of the dorsal side of the foot was intact.
Angioleiomyoma is one of the three different forms of leiomyoma, which is also known as vascular leiomyoma [1,2]. They seem to be more prevalent in women, and typically affect patients in their fourth to sixth decades of life [3].
Several theories have been floated, however no specific etiologic factors for the pathogenesis of angioleiomyoma have been identified. These hypotheses include pregnancy, hormonal changes, vascular malformations, and venous stasis induced by trauma. None of them was found in our case [4,5]. Another potential etiologic element is heredity, an autosomal dominant inheritance pattern has been cited [4].
Considering the angioleiomyoma's chronic nature and the paucity of any recorded familial history, its specific etiology is challenging to determine [4,5]. Therefore, further research report is needed [3-6].
The differential diagnosis may include leiomyosarcoma, ganglionic cyst, fibroma, neurofibroma, gouty tophus, glomus tumor, lipoma, and hemangioma [2-5].
The clinical diagnosis of angioleiomyomas is often challenging because of their similar clinical appearance towards other types of neoplasms. As a result, a histopathologic investigation is necessary for a definitive diagnosis of angioleiomyoma [6].
Typically, angioleiomyomas appear as a compact, spherical mobile mass that develops from the deep dermis and subcutaneous tissues. They usually have small dimensions (0.5-2 cm in diameter) [1].
Even though pain isn't always noticed, when it does, it can have a variety of characteristics, such as pressure, sharpness, or pinching discomfort, and it is temperature-dependent. It has been suggested that this pain may be caused by compression of the nearby neural structures or local tissue anoxia [1].
Pain was the major symptom in our case, which drove us to inaccurately diagnose a schwannoma.
Imaging findings are frequently variable and non-specific, with the potential to appear as giant cell or neurogenic tumors. Therefore, MRI or doppler outcomes, despite their contribution to surgical planning, are generally unreliable [4].
According to recent research, simple excision and primary closure are the recommended course of treatment, with extremely low recurrence rates (around 0.36%) and minimal morbidity. The prognosis following surgical excision is favorable [4].
Malignant transformation to leiomyosarcoma is uncommon. It should be suspected if the lesion involves the bone structure or recurs [4-6]. In case of recurrence, it has been discussed that the new lesion must be removed and treated like other low-grade malignancies [1].
Angioleiomyoma is relatively uncommon benign soft-tissue that can develop in the extremities of middle-aged persons [3]. Preoperative diagnosis remains challenging to determine since clinical and radiographic evaluations are imprecise and ambiguous. Simple excision is extremely effective. The gold standard for establishing a conclusive diagnosis is histopathology [3,4].
Further researches are required to establish an accurate preoperative diagnosis, avoid therapy delays, enhance results, and assist in ruling out the development of malignancies [1].