Charcot arthropathy of the foot and ankle is a challenging pathology that can require intensive surgical reconstruction. Most often the pathology involves breakdown of the midfoot. Osteotomies of the midfoot to resect and correct the deformity can be unpredictable and time-consuming. With the advent of 3D printing, we propose a new technique utilizing custom cut-guides for midfoot osteotomies in Charcot reconstruction. This provides a reproducible, accurate and pre-planned direction for reconstruction. We present a series of four patients who underwent Charcot reconstruction with custom cut-guides with discussion of the pre-operative planning period and surgical technique.
Charcot, Osteomyelitis, Midfoot arthrodesis, Patient specific instrumentation, 3D printed implant
The surgical management of Charcot neuroarthropathy is one of the most challenging aspects of modern-day foot and ankle surgery. This progressive, debilitating condition has a strong predilection for the joints of the foot and ankle, particularly the midfoot with around a 60% incidence of tarsometatarsal joint involvement [1-3]. Surgical reconstruction of Charcot deformity aims at creating a stable, plantigrade and ulcer-free foot, with the "superconstruct" method proving to be the gold standard of care [4]. Proper foot alignment is essential; namely the foot must be plantigrade and coaxial to the lower leg to facilitate tibio-calcaneal alignment with axial loading.
Internal pedal amputations" date back to as early as 1887 when midfoot amputations were done in patients with skeletal tuberculosis [5,6]. The rationale behind internal pedal amputations is to preserve bone distally, particularly, if the breakdown is limited to the midfoot. Midfoot osteotomies are a commonly-used to restore a functional forefoot to rearfoot relationship. The osteotomy must be planned to correct the planes of deformity which can be technically challenging both in planning and surgical execution [7].
Patient specific cut guides using computed tomography and three dimensional planning have become a useful tool in many aspects of orthopedic, plastic, and maxillofacial surgery. These guides have been used in mandibular reconstruction, total knee arthroplasty, total hip arthroplasty, and long bone corrective osteotomies. In the realm of the foot and ankle they have been utilized in total ankle arthroplasty as well as supra-malleolar osteotomies. It has been used in many facets of deformity correction but has yet to be described in the use of foot deformity in the presence of Charcot neuroarthropathy.
We present a novel adaptation of the midfoot osteotomy with use of patient-specific three dimensional cut guides to surgically correct midfoot charcot deformities. These guides were found to have reproducible results with the potential to decrease operative time. At most recent follow up all patients had successful limb salvage, were ulceration free, and returned to community ambulation with the assistance of extra-depth shoes, custom accommodative orthoses, or bracing.
A total of four patients presented with midfoot charcot arthropathy deformities. Each patient presented with a progressive deformity, failing conservative treatment with increasing risk of ulceration and infection. One patient had a history of infection which was treated surgically by an outside physician without amputation. Three of the four patients had known diabetes mellitus with complications of peripheral neuropathy while the other patient had peripheral neuropathy due to history of a back injury. All three diabetic patients had glycosylated hemoglobins checked preoperatively and were considered to be controlled prior to proceeding. No patient had a history of tobacco abuse and noninvasive vascular testing was evaluated prior to surgery. No vascular intervention was indicated for any patient (Table 1). Radiographic parameters were measured preoperatively and postoperatively by a single author and confirmed by the senior author (Table 2 and Table 3). Following plain radiographs, preoperative computed tomography (CT) scans were utilized to design and print patient specific three dimensional (3D) cut guides. These guides were utilized to perform a midfoot osteotomy, aligning the forefoot to rearfoot with rigid internal fixation.
Table 1: Demographic measures. View Table 1
Table 2: Radiographic parameters. View Table 2
Table 3: Radiographic measurements. View Table 3
On initial presentation, radiographs were taken (Figure 1). Each was diagnosed with midfoot charcot collapse. Two of the four patients had a nonhealing ulceration that was without acute infection. The other two patients did not have ulceration but radiographic parameters consistent with increased risk of ulceration [8] and progressive deformity that was not stabilized with conservative treatment. Surgical correction of the deformity was discussed with each patient with goals to create a planti-grade, functional foot and reduce the risk of ulceration and infection. A CT scan of the operative extremity was obtained.
 Figure 1: Pre-operative radiograph.
View Figure 1
Figure 1: Pre-operative radiograph.
View Figure 1
The CT scan was sent to the company (Restor3d, Inc. Durham, NC) to be uploaded and a computer-assisted design image was created from the CT scan for analysis. The top priority is to determine how the midfoot osteotomy should be performed so that there is a plantigrade relationship between the forefoot and rearfoot. This should also preserve bone distally and proximally that is not involved in the breakdown. Once this relationship is established, macro anatomy along the area of resection is identified to create the cut-guide (Figure 2). This will allow the surgeon to better identify how the guide must be placed in order to achieve the right angle of resection. A 3D-printed model of the deformity is printed alongside the cut guides. The guides can be made in various sizes; usually with a nominal size, one larger, and smaller (primary surgeon utilizes +/- 5%). Holes within the guide are made for temporary fixation in order to fluoroscopically confirm the positioning of the guide. These guides are impregnated in barium sulfate for fluoroscopic visualization. With accurate designing, the osteotomy should be well opposed and precise deformity correction and bone resection.
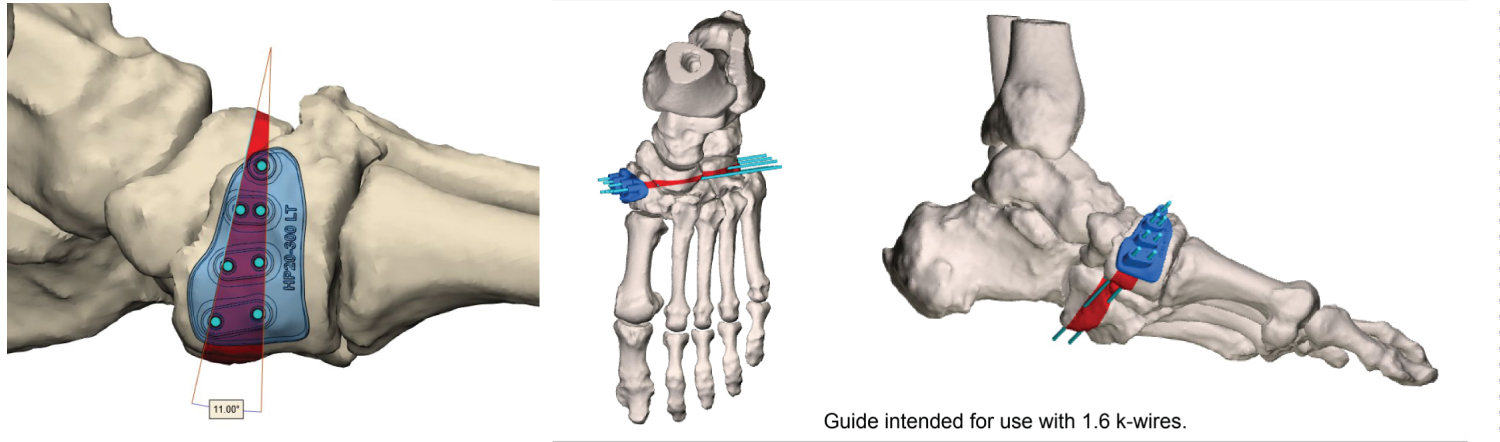 Figure 2: Relationship established, guide based on macroanatomy.
View Figure 2
Figure 2: Relationship established, guide based on macroanatomy.
View Figure 2
At the time of surgery, the patient is positioned supine on the table. Medial and lateral incisions are made and full-thickness flaps are raised from the bone both dorsal and plantar. Once the soft tissues are raised, a malleable retractor is placed deep to the dorsal soft tissues and another deep to the plantar tissues (Figure 3). This protects the soft tissues during placement of the cut guide and osteotomy.
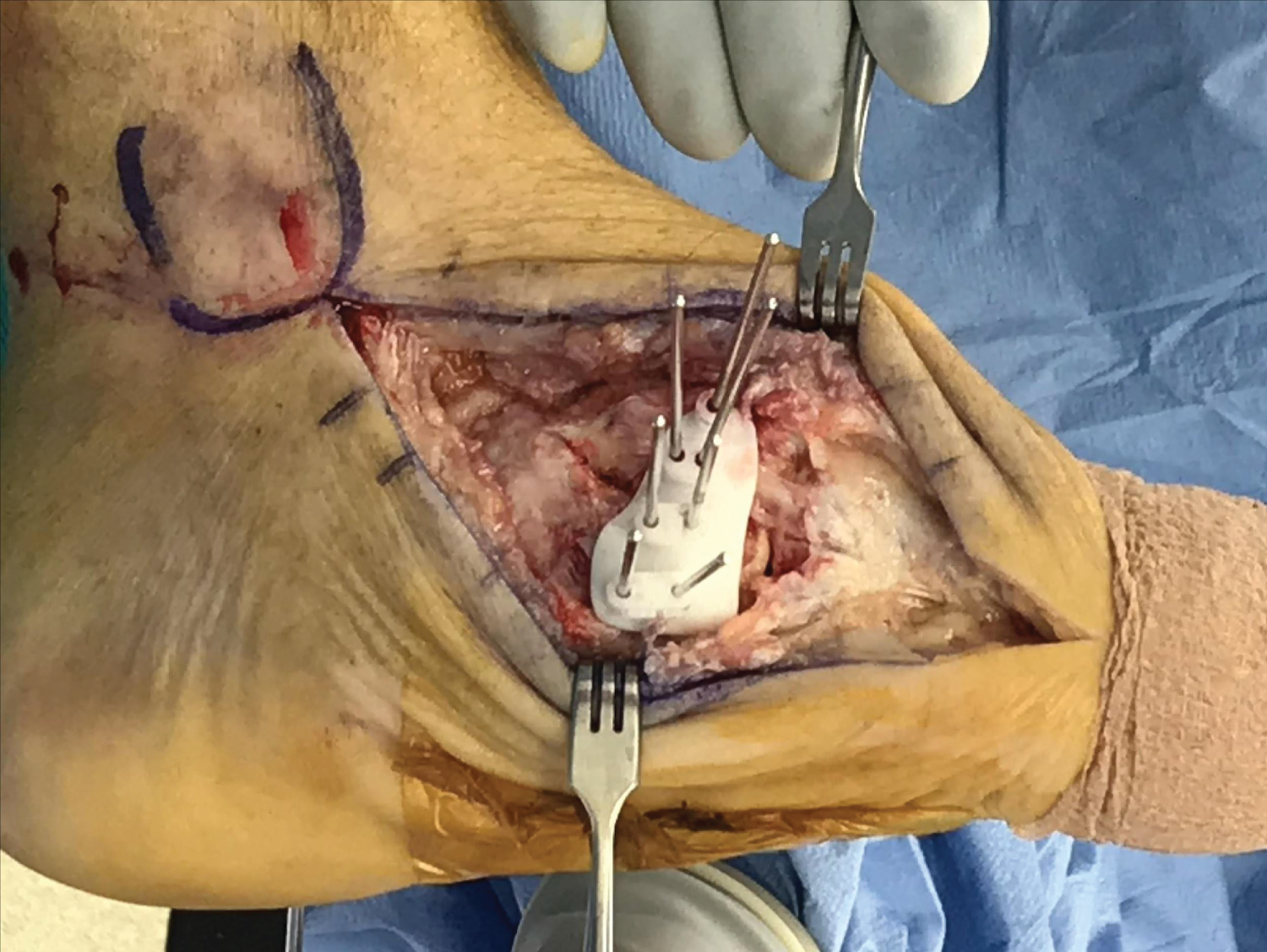 Figure 3: Cut guide intra-op.
View Figure 3
Figure 3: Cut guide intra-op.
View Figure 3
The guides can be placed along the model of the deformity to confirm where accurate placement of the guide should be. Once this is confirmed, the guide is fitted medially along the midfoot. An inherent "press-fit" should be appreciated. Two or three Kirschner wires are placed along the guide and placement is confirmed under fluoroscopy (Figure 4). The surgeon should note parallel placement of the wires indicating that placement is correct. Once this is confirmed, more wires can be placed along the cut guide to prevent movement.
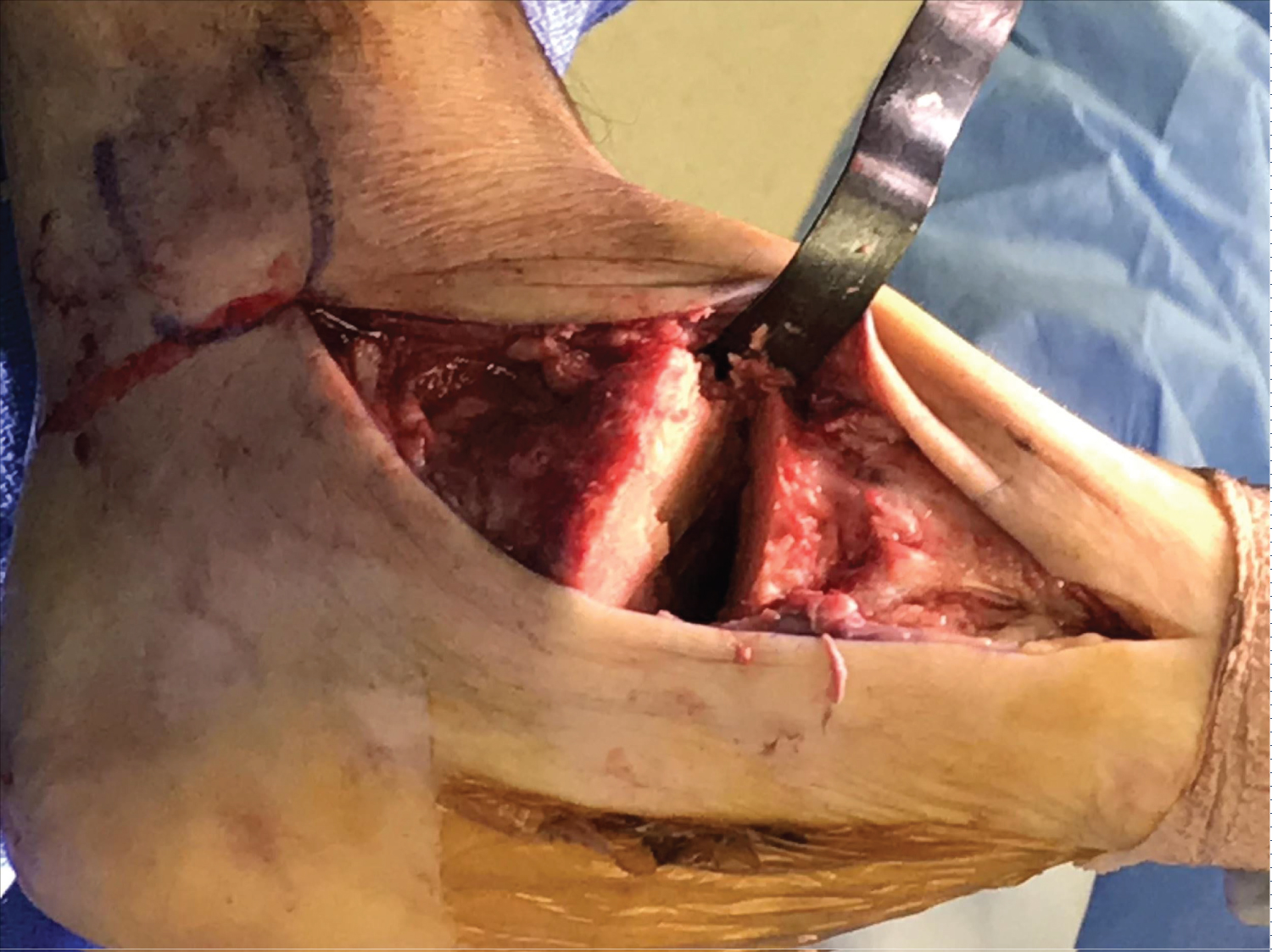 Figure 4: Wedge resection based on cut-guide.
View Figure 4
Figure 4: Wedge resection based on cut-guide.
View Figure 4
The cut guide is then removed once the wires are in place. If the cut guide is able to slide off easily with multiple wires placed, this also confirms accurate placement of the guide and wires for the osteotomy. A saw is then used to make the midfoot osteotomy on the outside of the wires. The saw should hug alongside the wires and be through and medial to lateral. After the osteotomy is made, the wires can be used to joystick the wedge resection out of the midfoot. This can be passed off the operating table. Any use of biologics or adjunctive bone graft should be placed within the osteotomies at this time. The forefoot and rearfoot are then opposed and temporarily pinned. Positioning of the rearfoot and forefoot are checked under fluoroscopy and compared to the preoperative planning guide to confirm accurate placement and opposition of the osteotomy.
Once positioning is confirmed and accurate, rigid internal fixation can be placed across the osteotomy in a superconstruct fashion. The use of beaming, plating, and multiple screws is recommended here (Figure 5).
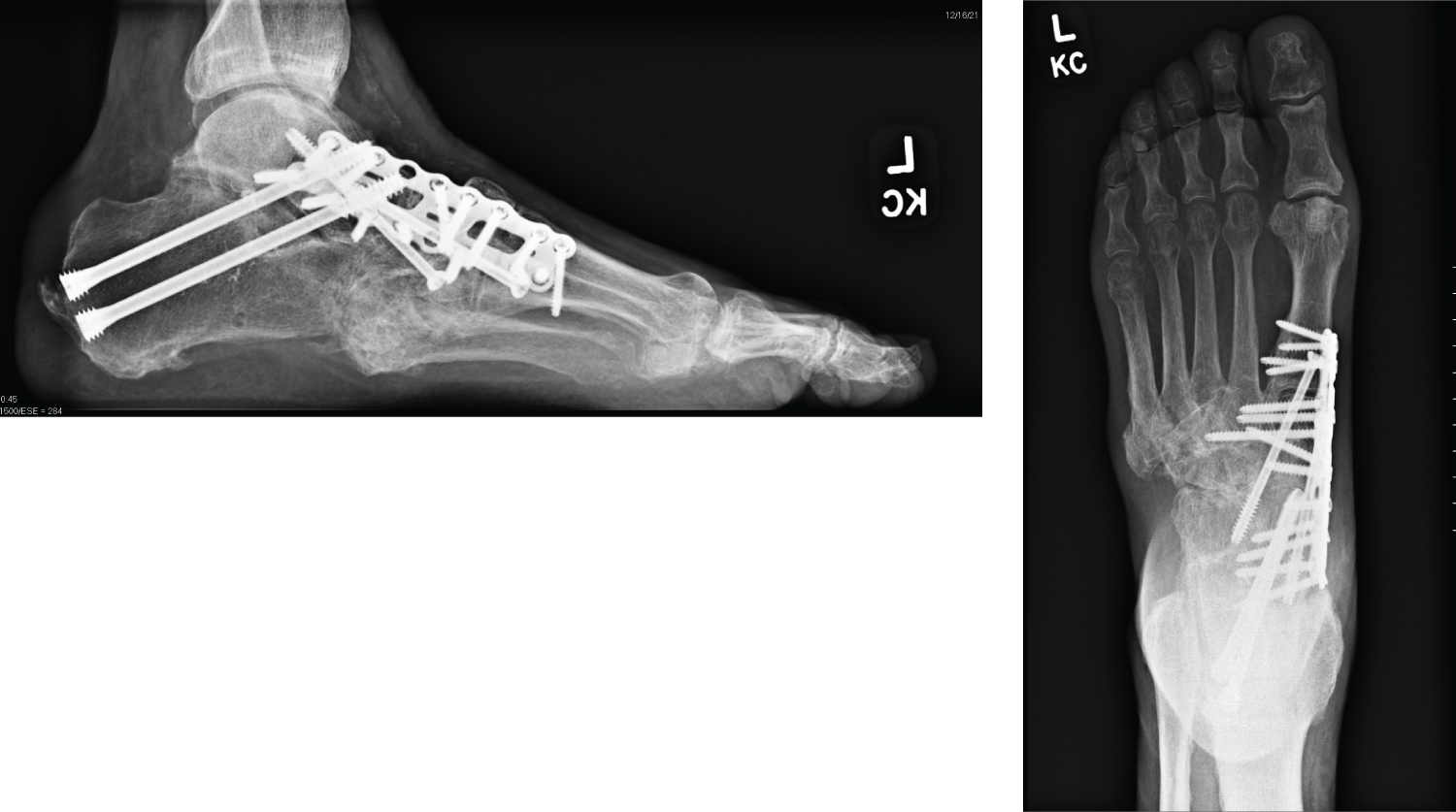 Figure 5: Final fixation.
View Figure 5
Figure 5: Final fixation.
View Figure 5
Traditional post-operative recovery for charcot reconstruction should be utilized.
All patients went on to heal uneventfully. In terms of sagittal plane radiographic parameters, the mean +/- standard deviation correction in Meary's angle was 17.63 +/- 4.46. The mean +/- standard deviation correction in cuboid height was 4.83 mm +/- 2.88. The mean +/- standard deviation correction in talar declination was 12.93 +/- 2.59. The mean +/- standard deviation correction in calcaneal inclination 5.08 +/- 1.73. In the transverse plane, The mean +/- standard deviation correction in the talo-first-metatarsal angle was 16.00 +/- 4.95 and calcaneo-cuboid abduction was 9.90 +/- 8.55 (Table 3). All patients returned to ambulation in accommodative shoe gear or bracing without recurrent Charcot event or ulceration.
Midfoot osteotomies are powerful procedures to correct deformities in order to achieve a functional plantigrade foot. This becomes particularly important in patients with Charcot arthropathy. Most charcot arthropathy is found in the midfoot and can lead to severe multi-planar deformity. It is important that the surgeon is able to identify which plane(s) of deformity are present in order to successfully execute a correctional osteotomy.
In the frontal plane, radiographs with midfoot charcot will show a varus or valgus malalignment. This is depicted by "stacking" and superimposition of the metatarsals on radiographs, respectfully. In the sagittal plane, radiographs with midfoot charcot will show a dorsiflexed or plantarflexed malalignment. This can sometimes be superimposed by a "bayonette" deformity where there is subluxation or dislocation of one bone sagittally displaced atop another. In the transverse plane, radiographs with midfoot charcot will show a abductor or adductory malalignment. Goals of reconstruction focus on creating a plantigrade foot and restoring anatomic relationships [9]. Sagittal plane deformity is more often associated with ulceration, thus emphasis was placed on lateral radiographic parameters in terms of correction [10].
Radiographic parameters such as Meary's angle, the talo-first-metatarsal angle, cuboid sag, and talar declination have been identified as predictors for ulceration in midfoot Charcot [10,11]. Therefore, these angles must be focused on when correcting the midfoot deformity. Based on the plane of deformity, a wedge osteotomy can be performed with the base oriented to restore these anatomic alignments. Sometimes, this wedge may be biplanar to correct more than one plane of deformity.
Previous techniques to create this wedge resection have been described utilizing axis guides intraoperatively. This technique is fully dependent on accurate fluoroscopic utilization, proper placement of axis guides and proper wedge resection [12,13]. This can lead to lessened accuracy of correction which can require more time in the operating room or result in a less-than accurate correction in a high risk patient. 3D patient specific cut guides may result in reduced operative time, improved efficiency and more reproducible results.
The use of 3D printed cut guides has grown in popularity for treatment of other orthopedic pathology. The use has been primarily for pre-operative planning and allows determination of correction prior to the actual surgery. Early research on its use in orthopedic surgery has shown to improve visual and conceptual calibration by the surgeon. There is a reduction in reoperation rates and improved technique by novice surgeons [14]. The argument against use of 3D-printed technology is primarily its novel use and economic costs. As this becomes more normalized in surgery, its novelty and costs will also resolve [15].
With the utilization of patient-specific 3D cut guides for midfoot Charcot deformity, the guides remove all variable factors that play into the use of axis guides. This is because the guide is determined pre-operatively based on desired correction via CT and shaped to fit the patient's macro anatomy. Therefore, the guide can only be placed in a single orientation. The advent of 3D printing allows for more reliable preoperative planning to treat complex deformities such as midfoot Charcot [16].
Amar Gulati, Lance Johnson and Peter Highlander have no financial disclosures, commercial associations, or any other conditions related to this study posing a conflict of interest to report.