Nanotechnology means measurements estimated by nanometers or one-billionth of a meter- - to make structures, medical devices, gadgets and frameworks for medical, clinical and other uses, such as disease diagnosis. Cancer immunotherapy uses medications or drugs to help a patient's immune system fight cancer, as opposed to chemotherapy, which uses drugs to directly kill cancer cells, according to the National Cancer Institute (NCI). Antigen-consolidating nanoparticles with immunomodulatory agents activate immune cells and modify the tumor microenvironment to boost antitumor immunity. Scientists have been exploring the potential of nanomaterials to fight metastatic cancer and cancer immunotherapy, taking advantage of their advantageous properties, such as enhanced drug delivery, increased specific surface area, and controlled surface chemistry, which can improve the effectiveness of treatment. Through ongoing applications of nanotechnology and the improved results they yield, as well as new emerging nanotechnologies for drug delivery, this field will continue to grow, ultimately leading to clinical translation of the enhanced immunotherapy of cancer. In this review, the recent applications of nanotechnology in cancer immunotherapy and its future prospects are discussed. Additionally, emphasis are laid on the potential of nanotechnology-based therapies to deliver effective cancer immunotherapy.
Nanotechnology, Nanomaterials, Cancer immunotherapy, Chemoimmunotherapy
Cancer is a major global health issue, encompassing an array of diseases with varying biological characteristics. Cellular and genetic injuries can trigger cancer transformation from a single cell, known as clonal cancer onset. Radiation, smoking, exposure to cancer-causing agents, oncogenic viruses, mechanical friction, and the expression of pre-existing genetic defects can all contribute to the development of cancer.
Carcinogens, which are cancer-causing agents, can be found in many sources including tobacco smoke, certain foods, polluted air, and chemicals used in a variety of industries. The presence of cocarcinogens facilitates the carcinogenic stepwise process, which leads to the transformation of normal cells into malignant ones. To form a visible tumour, cancer cells need to multiply and create a large number of cancerous cells. The tumour grows rapidly, increasing exponentially to reach its maximum size. When a large tumour occurs, it consumes the body's nutrients, which, if left untreated, may result in death of the patient. This growth pattern of malignancy or cancer is called Gompertzian growth [1].
Conventional cancer therapeutic strategies such as surgery, chemotherapy and radiotherapy have been applied in the medical field for several years. Chemotherapy has long served as one of the main clinical treatment methods to cure cancer [2]. A majority of tumours may be eradicated by applying these approaches; however, metastasis and subsequent recurrences remain a formidable challenge in the clinic [3,4]. The major drawbacks of conventional chemotherapy include the possibility of drug resistance, low bioavailability, and severe side effects. Novel drug delivery systems (NDDS) may be an alternative to conventional chemotherapy, as they can help to optimize therapeutic effects and reduce the drawbacks associated with the traditional approach. The proposed advantages of NDDS systems consisting of natural resources materials are biodegradability, high biocompatibility, nontoxicity, and non-immunogenicity. In order to combat this, alternative methods, such as cancer immunotherapy, must be employed. This method aims to completely destroy the primary tumour and tumour metastases as well as induce immunological memory to prevent relapse.
Rapidly advancing cancer treatments such as Cancer Immunotherapy (CI), considered by some to be a “fifth pillar” of treatment, have been developed as an alternative to surgery, chemotherapy, radiation, and targeted therapy [5]. This approach to cancer treatment began in 1891 with William B. Coley's successful application of the first cancer immunotherapy program. A rudiment of cancer immunotherapy, it involved the use of Streptococcus as a bacterial toxin to exploit the patient's natural defense mechanisms. A new stage of exploration and investigation into cancer treatments was commencing [6]. The US Food and Drug Administration (FDA) approved first dendritic vaccine-based cellular immunotherapy Sipuleucel-T (APC 8015) which was the first a fully monoclonal antibody cancer vaccine was approved in 2010 and 2011 [7,8]. Therapeutic strategies of tumour-specific monoclonal antibodies may be divided into tumour-marked cancer cells and immune checkpoint blockades. Antibody-based medications, including bevacizumab (VEGF), rituximab (CD20), and trastuzumab (HER2) can facilitate the chemotherapy process for cancer patients. The development of cancer immunotherapy has seen great progress, yet there are still issues to address such as improving therapeutic benefits and reducing side effects. Cancer treatment will be revolutionized by the advent of cancer immunotherapy, which broadens the range of treatments beyond the traditional methods of surgery, radiotherapy, and chemotherapy. Cancer immunotherapy has shown promising results in providing therapeutic benefits, showing potential for a variety of practical applications. By boosting the host immune system or blocking tumor immune evasion, cancer immunotherapy creates a systemic, targeted, and persistent anticancer response [9].
In the late 1980s, nanotechnology began to emerge as an interdisciplinary field of science, rapidly expanding into the realms of medicine and health, among many other subject areas. Nanotechnology involves the manipulation and use of materials on a nanoscale, typically ranging from 1 to 100 nanometers in size. It has applications across many fields of science, engineering, and technology. Nanotechnology advancements and their therapeutical applications, especially nanomaterials, offer plentiful benefits compared to traditional drug development methods.
Nanotechnology has advanced significantly in recent years, leading to the development and application of nanomaterials in a variety of fields, including physics, chemistry, materials science, medicine, and biotechnology. These nanomaterials possess unique properties due to their structures, which are determined at the nanometer scale [10].
The physical properties of the material significantly alter when the size of the material is decreased. The biological effects of a substance can vary greatly depending on its size, shape, surface structure, chemical composition, charge, agglomeration, aggregation and solubility. The increased surface area, vascular permeability, and cellular penetration of nanomaterials contribute to their enhanced biological effects. Nanomaterials offer beneficial properties that make them advantageous to use in the medicine and biotechnology fields [11].
Nanotechnology has opened the door to numerous possibilities for cancer immunotherapy, with new designs being developed for use in the medical and health fields [12]. Nanoparticles (NPs) and Nanomaterials possess excellent biocompatibility, making them ideal for use in targeted drug delivery systems and for tracking their biodistribution. Furthermore, drug-coated nanomaterials can increase the bioavailability, extend the half-life, and improve the stability of pharmaceuticals while protecting them from degradation [13,14]. Efficient and good physiochemical properties (Figure 1) make polymeric nanoparticles (NPs) ideal for delivering antigens, antibodies, vaccines, cytokines, and adjuvants [15,16]. Furthermore, they preferentially accumulate in important antigen-presenting cells (APCs), such as DCs in the draining lymph nodes. Eradication of cancer by T cells is the only single step in the Cancer-Immunity Cycle, which accomplishes the delicate balance between the recognition of non-self and the prevention of autoimmunity [17,18]. Recognition of cancer cell T cell inhibitory signals, including PD-L1, has provoked the development of a novel class of cancer immunotherapy that specifically hinders immune effector inhibition, reinvigorating and potentially expanding preexisting anticancer immune responses.
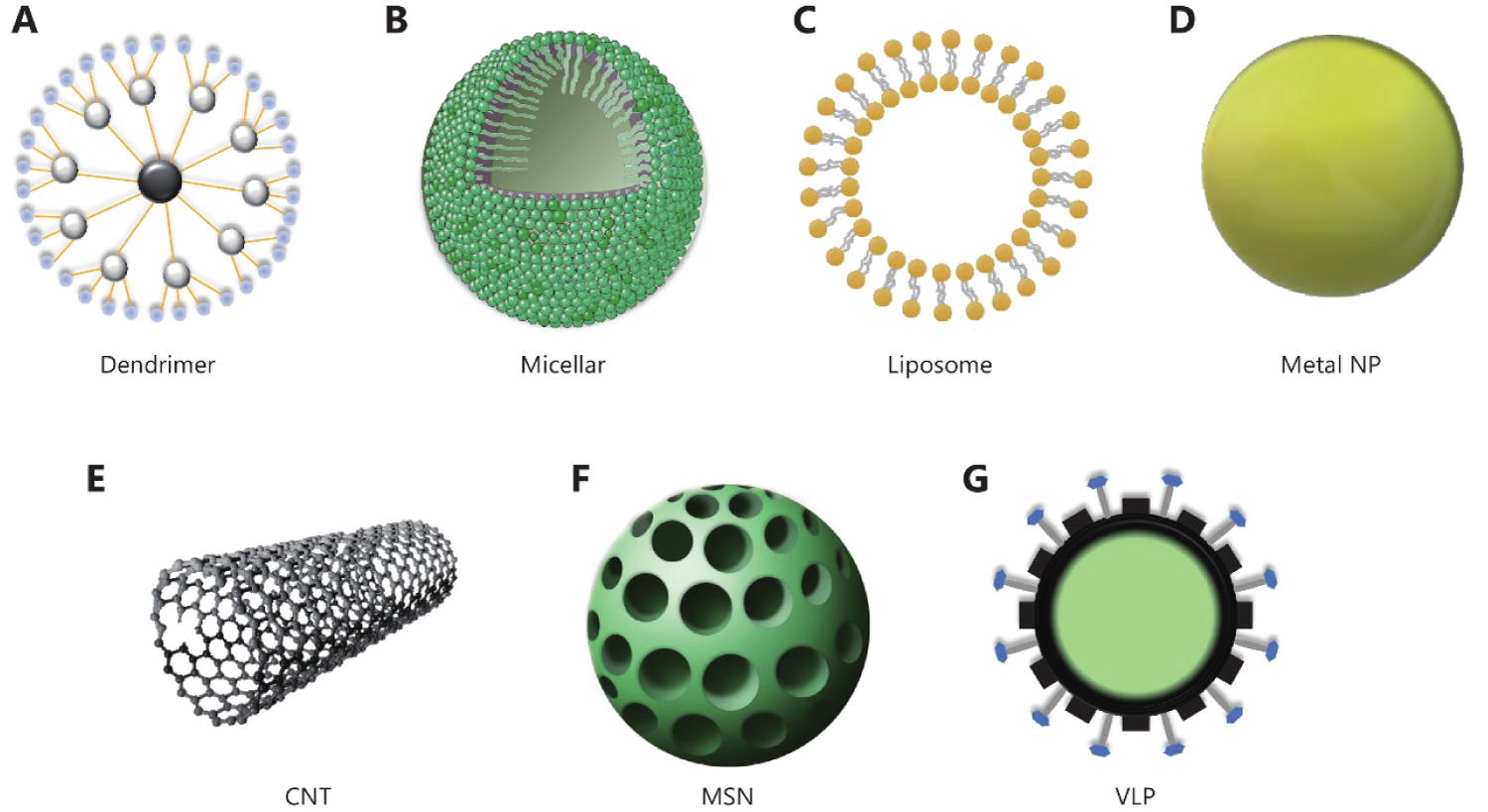 Figure 1: In cancer immunotherapy, a variety of nanomaterials with distinct architectures can be employed. Polymeric NPs, such as (A) Stepwise branching dendrimer and (B) Core-shell structure micellar; (C) Liposome with lipid bilayer; (D) Solid gold NP; (E) CNT comprises of carbon cylindrical models; (F) Honeycomb-like porous structure MSN; and (G) VLP generated from virus without genetic material [25].
View Figure 1
Figure 1: In cancer immunotherapy, a variety of nanomaterials with distinct architectures can be employed. Polymeric NPs, such as (A) Stepwise branching dendrimer and (B) Core-shell structure micellar; (C) Liposome with lipid bilayer; (D) Solid gold NP; (E) CNT comprises of carbon cylindrical models; (F) Honeycomb-like porous structure MSN; and (G) VLP generated from virus without genetic material [25].
View Figure 1
Nanotechnology is currently providing an excellent possibility for the advancement of cancer immunotherapeutic methods. This paper covers the underlying ideas, current state, and future perspectives of the application of nanotechnology in cancer immunotherapy research [19].
Cancer immunotherapy is considered to be the most effective approach to treating cancer, as it harnesses the power of the patient's own immune system to target and destroy cancerous cells. This method has been shown to produce stronger anti-tumor responses and carry a lower risk of metastasis and recurrence than more traditional treatments. Nanomaterials are essential for the successful delivery of medications targeted at cancer, and they offer tremendous potential to enhance the efficacy of cancer immunotherapy in many cases. This is due to their rapid growth and complex vascular structure. Nanomaterials are defined as materials with at least one dimension from 0.1-200 nm. Nanomaterials with a size of 0.1-200 nm evade kidney clearance while specifically accessing tumour tissues. The use of nanomaterials to deliver medications results in a prolonged blood retention time, an extended half-life, an improved drug-distribution in tumours, and a decreased toxicity-all of which together allow for a larger tolerated dose [20-23]. Nanomaterials' characteristics, such as their ease of modification and the ability to target ligands preloaded on the surface, will aid in the intake of immune cells [22,24,25]. The application of nanomaterials for the delivery of anti-cancer drugs or cancer-detecting agents will also be beneficial for cancer immunotherapy. Typical structures of nanomaterials have been used to cancer immunotherapy shown in Figure 1.
Nanomaterials are used in cancer immunotherapy are many types and can be classified into organic Nanoparticles like polymeric NPs such as dendrimer, liposome, exosome, Hybrid Nanoparticles like Hydrogel and Inorganic Nanoparticles like carbon nanotubes (CNTs), mesoporous silica NPs (MSNs), metal NPs and virus-like particles (VLPs) (Table 1).
Table 1: Nanomaterials used for cancer immunotherapy [25]. View Table 1
Over the past decade, polymeric nanoparticles (NPs) have been developed as an effective drug delivery system for cancer treatment. These polymeric NPs are composed of highly biodegradable and biocompatible polymers, both synthetic and natural, that are designed to act as a targeting vehicle for a specific disease [26,27]. To improve the effectiveness of antitumor vaccines, tumor-associated antigens (TAA) are encapsulated in polymer nanoparticles for enhanced antigen (Ag) delivery. Biodegradable polymers have a major advantage are they degraded within the body either enzymatically or non-enzymatically to produce biocompatible, nontoxic byproducts. These byproducts are then excreted by normal metabolic pathways such as the TCA cycle (tricarboxylic acid cycle).
Chitosan, micelles, dendrimers, hydrogels and Polymeric NPs, such as poly(D, L-lactide co-glycolide) copolymer (PLGA), polylactide acid (PLA), Poly(1-caprolactone) (PCL), have been widely employed in drug delivery systems and targeting vehicles. The Food and Drug Administration (FDA) has approved the use of polymeric nanoparticles, such as polylactide acid (PLA) and polylactic-co-glycolic acid (PLGA), which are biocompatible and biodegradable. These nanoparticles can be loaded with a variety of biologically active chemicals, making them an ideal delivery vehicle for drugs or other therapeutics. PLGA is a random ring-opening copolymer produced by combining two monomers, such as cyclic dimers (1,4-dioxane-2,5-dione) of glycolic and lactic acids. Depending on the ratio of lactide to glycolide used in the polymerization, different forms of PLGA may be obtained [28,29]. PLGA is a polymer of lactic acid that is preferred over other lactic acid-based polymers, such as PLA and polyglycolide, due to its greater solubility. PLGA can be dissolved by a range of solvents including tetrahydrofuran, acetone, dichloromethane, etc. PLGA microspheres and its monomers are commonly employed in the delivery and encapsulation of numerous anticancer drugs. In recent years, PLGA nanoparticles (NPs) with siRNAs, cytokine agonists or CpG-coated tumor antigens have been used to enhance the uptake of antigens by dendritic cells (DCs) and the activation of both cytotoxic T lymphocytes (CD8+) and T helper cells (CD4+) immune responses [30-32]. PLGA nanoparticles (NPs) can be used as delivery tools to reach the processing pathways for both MHC class I and II molecules, thereby facilitating the maturation of dendritic cells (DCs) [33]. Dendrimers are synthetized with a distinct, stepwise branching pattern radiating outward from a central point, creating unique physical characteristics. Dendrimers are loaded with peptides that specifically target dendritic cells, such as ICAM-3-grabbing non-integrin (DC-SIGN) or MHC class II-targeting peptides, for the purpose of antigen presentation and efficient targeting of DCs [34,35]. Micellar nanoparticles possess an inner amphiphilic polymer core surrounded by external hydrophilic residues, while hydrogels are comprised of three-dimensional polymeric networks [36-38]. Micellar nanoparticles and hydrogels have been investigated for their potential to enhance antigenic peptide-based cancer immunotherapies through improved vaccine delivery.
Liposomes are artificially created vesicles that are used primarily to deliver both hydrophilic and hydrophobic drugs. Liposome are bilayer, the membrane is made of phospholipids that contain head group and tail group. The head groups are hydrophilic and the tail groups are hydrophobic due to a log hydrocarbon chain which greatly improves drug-loading efficiency [39].
Liposomes, consisting of phospholipids, have a structure that is similar to that of the cell membrane, resulting in decreased organ toxicity and improved biocompatibility when compared to inorganic nanoparticles. Cationic liposomes, due to their positive charge on their surface, are highly efficient for nucleic acid transfection. Furthermore, the polyethylene glycol (PEG) shell of liposomes ensures prolonged blood circulation in vivo [40]. Numerous phospholipid materials can have capacity to release accurately drug in different environments, and multiple components facilitate their modification. Most immune agents are antibody, polypeptide, or nucleic acid drugs. So, liposomes are considered perfect delivery carriers for mediating effective cancer immunotherapy by activating either the cellular or humoral response [41].
The delivery of cGAMP to metastatic melanoma tumors in the lung utilizing liposomal encapsulation resulted in anti-tumor activity, whereas no effect was produced at the same dose when administered as a free drug. The delivery of cGAMP liposomes into orthotopic melanoma tumors was facilitated, resulting in an improved retention of cGAMP at the tumor site, as well as enhanced co-localization with tumor-associated APCs. Liposomal delivery improved the agonist activity of the immune adaptor protein STING and increased immunological memory in previously treated mice from rechallenge with tumor cell [42].
Guan, et al. synthesized and characterized immunostimulatory Liposomal spherical nucleic acids (IS-LSNAs) that can selectively target RNA selective for toll-like receptors (TLRs) 7/8. Plasmacytoid dendritic cells have been shown to take up IS-LSNAs and activate TLR7/8 via NF-κΒ signaling, as revealed by an increase in cytokine production and the upregulation of costimulatory receptors in reporter cell lines and primary immune cells. The antigen-loaded core of the liposomes ensured enhanced antigen-specific T-cell priming like TLR7/8 and TLR3 can also be exploited to induce DC maturation. The first introduction of IS-LSNAs consisting of RNA, experiments show that one can improve an antigen-specific T cell response greater than that of free or cationic lipid-transfected RNA of the same sequence selective for TLR7/8 [43].
Kranz, et al. show that dendritic cells can be targeted precisely and effectively in vivo using intravenously administered RNA-lipoplexes (RNA-LPX) based on well-known lipid carriers by optimally adjusting net charge. Furthermore, there would be no need for functionalization of particles with molecular ligands. A liposome-lipoplex combination can protect and facilitate the efficient uptake and expression of a encoded antigen by dendritic cells and macrophages found in various lymphoid compartments. RNA-LPX vaccines represent a commonly applicable class of vaccines for cancer immunotherapy that can be used to elicit both highly potent adaptive immunity and type-I-IFN-mediated innate immunity responses. This is because any polypeptide-based antigen can be encoded as RNA [44].
Exosomes have a similar vesicle structure as liposomes, it can be categorized as organelles in between macromolecules and cells, and have attracted increasing attention as diagnostic markers, therapeutic agents and immunotherapy of cancer [45]. Exosomes, which are endogenously produced by a variety of cells and circulate freely in all body fluids, possess greater potential for delivering immunological regulators under both normal and pathological conditions due to their natural targeting, non-immunogenicity, good biocompatibility, and high penetration of biological barriers [46]. They are mostly derived from multivesicular bodies formed by intracellular lysosomal microparticles. Publish report show that that exosome released by immune cells play important role in activating immune suppression.
Wolfer, et al. observed in a human in vitro model system that exosomes, secreted by living tumor cells, may be contain and transfer tumor antigens to dendritic cells. The antitumor effects of Tumor-Derived Exosomes (TEX) were demonstrated in mice after uptake of tumor exosomes and induction of potent CD8+ T-cell-dependent dendritic cells. Tumor-Derived Exosomes (TEX) offer a promising way to generate tumor-rejection antigens for T-cell cross priming, thus providing a valuable resource for the development of cancer immunotherapies [47].
Mahmoodzadeh, et al. novel designed exosomes derived from macrophage cell and staphylococcal enterotoxin B. To evaluate the therapeutic potential of these novel constructed nano-vesicles against fibrosarcoma tumor, animals were immunized with different types of extracellular vesicles (EXOs). The animal models demonstrated that EXOHSP was significantly more effective than EXO and EXOLys in reducing the number of tumor cells and stimulating immune responses. The results show that a novel HSP70-enriched EXO, designed specifically for use as an immunoadjuvant, is an effective tool in cancer immunotherapy [48].
Romagnoli, et al. treated human breast adenocarcinoma cells (SK-BR-3) with Dendritic Cell-Derived Exosomes, which stimulated the secretion of interferon-γ (IFN-γ) and stimulate and activate SK-BR-3-primed CD3+ T-cells. The incorporation of DC-Exo by the tumor cells demonstrated improved therapeutic response, suggesting that DC-Exo may be an effective tool in cancer immunotherapy [49].
The blood-brain barrier (BBB) basically restricts medicine from entering into the brain. Exosomes derived from brain endothelial cells have been successfully used to overcome the "blood-brain barrier (BBB)" and deliver anti-cancer drugs in a zebrafish (Danio rerio) brain cancer model. These studies suggest that exosomes may be a viable option for delivering anticancer drugs in immunotherapy for brain cancer [50].
Exosomes have revolutionized drug delivery, allowing for the efficient transport of drugs, genes, antibodies, adjuvants, antigens, and cytokines to target cells with precision, making them invaluable tools for cancer immunotherapies.
NP-gels, a novel type of hydrogel nanoparticle, have demonstrated superior capabilities in controlling drug release kinetics, providing remote-controlled drug release, aiding in targeted drug delivery, delivering drugs in a stimuli-responsive manner, and enhancing nanoparticle-based detoxification to improve drug delivery efficiency due to their increased structural diversity. Nanogels are three-dimensional, cross-linked polymeric networks that offer the best of both hydrogels and nanoparticles, combining their respective advantages. The inclusion of labile bonds in the composition of hydrogels can result in the formation of a relatively stable system, allowing for the adjustment of its service life, gel strength, and sustained release properties to meet specific demands. Hydrogel Nanoparticles possess two essential properties for hydrogel therapy - biodegradability and biocompatibility - as they are designed to resemble biological cells and tissues and remain in contact with the body for extended periods of time [51,52].
Chemical modification of the NP-gels is one of the future generations of drug delivery systems (DDS) as it has several advantages such as nano size, better drug encapsulation efficiency, surface modulation, lesser toxicity and serum stability of nanoparticles, improved swelling capacity, hydrophilicity, longer plasma circulation times, biocompatibility, and stimuli-responsiveness characteristics [53,54].
Nanogels, due to their small size, are well-suited for intravenous injections, can easily cross the blood-brain barrier, and can be readily internalized by cells. In comparison, macroscopic hydrogels are typically used for in situ administrations. Nanogels are also capable of encapsulating and protecting biomolecules from chemical and enzymatic degradation while maintaining their functionality and allowing the free flow of substrates and products [55].
It is not surprising that hydrogels, as drug delivery systems (DDS) for pharmacological class of anticancer agents, have been mostly used to carry hydrophilic drugs, given their equally hydrophilic nature. Anticancer agents most of them are low solubility in aqueous media. Hydrophobic anticancer agents present a major challenge in their use with hydrogels, as the incompatibility between their hydrophilic matrices and hydrophobic drugs often leads to low encapsulation and thus low efficacy. Though this issue has not posed any hindrance to wagering on Hydrogel Nanoparticles as an anticancer therapy [56].
Ueda, et al, evaluated the anticancer effect of IFN-α incorporated hyaluronic acid–tyramine (HA-Tyr) hydrogels and synergistic efficacy of IFN-α-incorporated HA-Tyr hydrogels + Sorafenib in human renal cell carcinoma (RCC)-xenografted in nude mice. A HA-Tyr hydrogel drug delivery system may prolong the biological half-life of natural human IFN-α and improve its anticancer effects on human RCC cells, according to the results of a study [57].
Bencherif, et al. designed a cryogel-based delivery system to encapsulate GM-CSF and CpG-ODN and administered it subcutaneously into mice to localize transplanted tumour cells. This vaccine is designed to induce a strong antitumor T-cell response and improve the survival rate of B16F10-bearing mice by releasing immunomodulatory factors and cancer antigens in a controlled spatio-temporal manner. These results suggest that cryogels may be a viable platform for the development of cancer immunotherapy [57,58].
MNPs have been investigated for their potential use in cancer immunotherapy, biomedical imaging, diagnostics, and treatment because of their versatile characteristics, such as size, shape, charge, and surface chemistry modification [59]. Gold nanoparticles (AuNPs) have been shown to be safe and can be used to improve the effectiveness of immunotherapeutic agents. The AuNP immunotherapies are better suited for synergetic combination treatment with existing cancer treatment like photothermal ablation [60].
Adam, et al. conjugated a modified CpG oligodeoxynucleotide and AuNPs to stimulates macrophages and inhibits tumor growth for improved cancer immunotherapy. AuNPs in combination with modified CpG attenuates side effects and stimulates macrophages and DCs to significantly inhibit tumor growth when compared to treatments with unmodified CpG [60].
Cho, et al. designed iron oxide-zinc oxide core-shell nanoparticles to deliver carcinoembryonic antigens into dendritic cells. The complexes, when acting as imaging agents, are efficiently taken up by DCs within one hour. This results in an improved tumor antigen-specific T cell response in mice, better survival and delayed tumour growth as compared to controls [61].
MNPs have a higher density than non-metallic nano formulations of the same size, which makes them more efficiently taken up by cells and provides a greater advantage for cancer vaccination strategies [62,63]. MNPs possess optical properties which can be leveraged to enhance combined metallic nanoparticle-mediated tumor ablation and cancer immunotherapy.
One-dimensional (1D) nanomaterials made from carbon, known as Carbon Nanotubes (CNTs), are synthetically produced by three major techniques: Laser ablation, electric arc discharge, and thermal or plasma enhanced chemical vapor deposition (CVD) Carbon nanotubes (CNTs) are being utilized due to their unique physicochemical properties to detect cancerous cells, deliver drugs, and treat cancer. CNTs are well known for their effectiveness in near-infrared photothermal ablation therapy, as they are able to rise temperature within tumors as a function of the light intensity and CNT dose applied [64-66].
CNTs possess unique properties, such as an ultrahigh surface area, that enable beneficial molecules, including drugs, nucleic acids, and peptides, to be attached to their walls and tips, thus promoting target specificity and facilitating the transport of antigens across cell membranes.
Many studies have demonstrated that CNTs can be efficiently transported across biological barriers, such as mammalian cell membranes, through endocytosis or other mechanisms and can effectively transport molecules into the cytoplasm without inducing any toxic effect [67-69].
Anti-neoplastic drug molecules have usually formed cleavable bonds between functional groups on the CNT surface or through polymer coatings of CNTs. CNTs are often functionalized by forming cleavable bonds between different functional groups on their surface, or by coating them with a polymer, in order to be used as anti-neoplastic drugs. CNTs can be used to boost the immunogenicity of weakly immunogenic tumor-associated peptides/antigens, serving as antigen-presenting carriers to stimulate a humoral immune response against cancer in the tumor microenvironment. CNTs have the potential to revolutionize vaccine development and immunotherapy by overcoming various challenges [70,71]. Research has uncovered that when a combination of carbon nanotubes (CNTs) and anti-CTLA-4 antibodies are administrated, tumor metastasis can be effectively prevented and strong adaptive immune responses can be activated [72].
Mesoporous silica nanoparticles (MSNs) have a honeycomb-like porous structure, with hundreds of empty mesopores, which allows them to absorb large amounts of bioactive molecules. Mesoporous Silica Nanoparticles (MSNs) are proving to be an ideal vesicle for drug delivery due to their excellent biocompatibility, biodegradability, and strong chemical and biological stability. Furthermore, their physical casing ensures that drugs housed within are protected from degeneration or denaturation. MSNs containing hundreds of empty mesopores provide a significant opportunity to control the loading rate and release kinetics of drugs, allowing for targeted delivery of antineoplastics to improve cellular uptake and prevent premature release before reaching the target site [73,74].
Drugs and siRNAs can be delivered into the body via MSNs, which have apertures that allow the substances to be co-delivered and induce the secretion of cytokines [75].
MSNs can deliver hydrophobic, membrane-impermeable drugs, making them a versatile transmembrane carrier for drug delivery and imaging applications. They are emerging candidates for both passive and active targeted drug delivery systems and can accumulate via better permeation and retention (EPR) effect in to tumor tissues. MSNs can be functionalized with targeting ligands, such as folate (FA) or EGF, to actively target specific drug delivery systems [76]. Their special structures have piqued the interest of many for potential use in cancer immunotherapy.
Virus-like particles (VLPs) are particles resembling viruses in terms of structure, form spontaneously, but do not possess the ability to replicate. VLPs are artificial nanostructures 20-100 nm in size. They are biocompatible and non-infectious, making them ideal vehicles to present many potential vaccine epitopes in a dense repeating array, as well as to produce antibodies against non-immunogenic substances along with tumor-associated self-antigens. VLPs are immunogenic and can stimulate immune responses, which can be used for cancer immunotherapy. VLP-based vaccines can target immune cells and enhance vaccine effectiveness [77].
Lizotte, et al. first reported that a VLP-based NPs generated from cowpea mosaic virus (CPMV) could suppress metastatic cancer and so it can be used as a cancer immunotherapeutic agent, rather than a delivery vesicle. CPMV nanoparticles are highly stable, non-toxic, and capable of being modified with drugs and antigens. Furthermore, their nanomanufacturing process is highly scalable. CPMV derived NPs specifically target and activate neutrophils within the TME, coordinating a downstream anti-tumor immune response which is able to kill multiple types of tumor cells, including those from ovarian, lung, breast, and colon cancers [78]. VLP nanocarriers can be used to deliver tumor antigens, drugs, and immunological adjuvants, and have been proven to have efficacy as a monotherapy. Such applications have opened up fresh possibilities for VLPs to improve cancer immunotherapy. The use of virus-like particle (VLP) based vaccines has advanced greatly over the last few decades, leading to a reduction in the morbidity and mortality associated with many infectious diseases and a potential prevention of cervical cancer caused by human papilloma virus [71].
Adoptive cell therapy (ACT), also known as cellular immunotherapy, is an ex vivo therapeutic treatment that utilizes the powerful and highly effective autologous immune cells of an individual's immune system to attack and eliminate cancer cells. Adoptive cell therapy leverages the natural capacity of the immune system to recognize and destroy cancerous cells, and can be administered through various methods, including Tumor-Infiltrating Lymphocyte (TIL) Therapy, Engineered T Cell Receptor (TCR) Therapy, Chimeric Antigen Receptor (CAR) T Cell Therapy, and Natural Killer (NK) Cell Therapy [79,80]. Tumor-infiltrating lymphocyte (TIL) therapy is a method of treatment that utilizes naturally occurring T cells which have already infiltrated a patient's cancerous tumor. This approach works by increasing the number of these T cells, and then activating them so they can fight the cancer. The more of these activated T cells that are re-infused into patients, the better their chances of effectively killing cancer cells and destroying tumors [81]. The adoptive transfer of tumor-infiltrating lymphocytes to patients with metastatic melanoma has been found to reduce relapse of the disease, as well as to induce autoimmune destruction of melanocytes [82]. TCR therapy for those patients who does not have T cells that have already diagnosed with cancer may be an option for patients who have been diagnosed with cancer and do not have functional T cells. In many patients, T cells may not be activated sufficiently in order to generate enough numbers to fight against cancerous cells. As such, TCR therapy may be needed in order to boost T cell activation. In the TCR approach, T cells are taken from patients and then activated and expanded to target specific cancer antigens, thereby allowing anti-tumor T cells to be more readily available [83,84]. Chimeric Antigen Receptors (CARs) have a key advantage in that they can bind to cancer cells even in cases where the antigens are not presented on the cell surface through Major Histocompatibility Complex (MHC). This enables them to target a larger number of cancer cells, thus improving their efficacy. However, CAR T cells are limited in the range of potential antigen targets they can identify, as they can only recognize antigens that are already expressed on the surface of the cell. In October 2017, the FDA approved the first ever CAR T cell therapy to treat certain types of large B-cell lymphoma in humans [85-87]. The formation of autologous CAR-T/NK cells for each individual patient often takes a number of weeks, making it a time-consuming and costly process that limits its availability for many patients. Therapeutic effectiveness against solid cancerous cells is limited, and this type of therapy can cause severe toxicity, including organ damage. The complexity and safety concerns surrounding ACT are limiting its clinical applications [88-90].
Hence, nanotechnology combined with ACT has the potential to enhance the efficacy of T-cell targeting strategies and cancer treatments. The application of nanotechnology in adoptive immunotherapy is more prevalent in targeting T cells than NK cells.
The treatment of T cells has seen many innovations in viral vectors and non-viral approaches, with the aim of genetically reprogramming NK cells as a substitute. High gene transfer efficacy with NK cells has been attained using viral vectors. Nonviral vector and gene transfer approaches, such as electroporation, lipofection, nanoparticle delivery, and trogocytosis, are becoming increasingly prevalent. Despite the improved gene transfer efficiency achieved by using NK cell lines with viral vectors, challenges remain when working with primary NK cells [91].
Stephan and other researchers are currently exploring the potential of scaffold-based T-cell delivery to improve adoptive T cell immunotherapy for inoperable tumors and reduce the rate of metastatic relapse after surgery using a mouse breast cancer resection model [91].
Nanotechnology offers a distinct advantage over viral vector methods for achieving transient gene expression. The viral method involved expensive instruments, as well as steps like exchange of culture medium and centrifugation which can lead to errors and increase the risk of contamination, compromising the final cell product. The automated method can lead to a decrease in cell viability, resulting in a decline in product yield and quality. The NP approach does not necessitate mechanical permeabilization of cell membranes in order to introduce transgenes, but instead, it binds to target cells and initiates receptor-mediated endocytosis [92] (Figure 2).
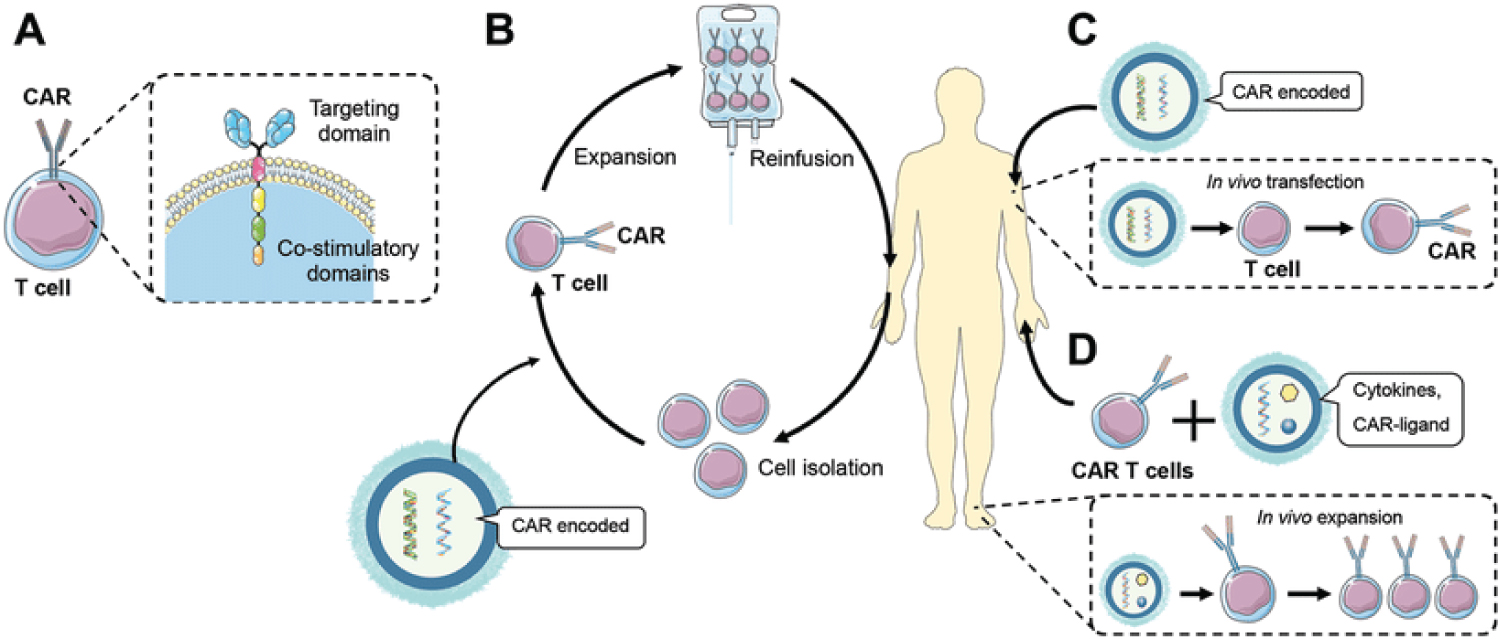 Figure 2: The application of nanotechnology to improve adoptive cell therapy. A) Design of a CAR-T cell. B) Nanoparticle‐assisted ex vivo transfection of patient's T cells. C) Nanoparticle-mediated in vivo transfection of CAR-T cells. D) Nanoparticles loading cytokines, or mRNA‐coding for a CAR ligand, with the aim of facilitating the in vivo expansion of the transferred CAR-T cells [93].
View Figure 2
Figure 2: The application of nanotechnology to improve adoptive cell therapy. A) Design of a CAR-T cell. B) Nanoparticle‐assisted ex vivo transfection of patient's T cells. C) Nanoparticle-mediated in vivo transfection of CAR-T cells. D) Nanoparticles loading cytokines, or mRNA‐coding for a CAR ligand, with the aim of facilitating the in vivo expansion of the transferred CAR-T cells [93].
View Figure 2
CAR-T therapy has limited effectiveness against solid tumors due to the intricate and inhibitory microenvironment of solid tumors, which is hostile to T cells. Nanotechnology has emerged as an innovative, non-viral approach to immunotherapy for cancer treatment. Though CAR-T therapy has certain limitations, nanotechnology can be used to address these challenges and enhance the current applications of this treatment. Over the past three years, CAR-T therapy using a novel and potent targeting molecule CD3 has emerged as a promising therapeutic strategy. This strategy involves the use of efficient DNA carriers to quickly and specifically edit T cells in order to efficiently kill tumor cells while decreasing the risk of serious systemic toxicities [12]. Nanotechnology has the potential to provide cost-effective and wide-reaching treatments for cancer through the use of adoptive immunotherapy. This has become a key focus of nanotechnology research.
Advancement of vaccine development technology is one of the most critical steps for protecting the lives of millions of people, and is essential for public health. Cancer therapeutic vaccines can be used to both prevent and treat certain cancers caused by viruses in healthy people.
The application of nanotechnology in cancer therapeutic vaccines offers distinct advantages over traditional cancer vaccines, such as:
Protection of vaccines from rapid degradation;
Targeting DCS with the use of ligands;
Nanomaterials can deliver vaccines, targeted antigens and adjuvants or other agents to increase antitumor response;
Enhancing cross-presentation to induce ctls;
The ability to site-specific delivery of antigens and enhancement of the bioavailability and distribution of antigens,
Enhance the retention time of tumor antigens in lymphatic and tumor tissues [93,94].
The U.S. Food and Drug Administration (FDA) approved three cancer therapeutic vaccines:
TheraCys ® (Bacillus Calmettle-Guerin) - a live attenuated strain of Mycobacterium bovis bacteria for non-muscle invasive bladder cancer;
Provenge ® (Sipuleucel-T) - a dendritic cell (DC) vaccine to treat certain men with advanced prostate cancer; and
T-VEC or Imlygic ® ) (talimogene laherparepvec) an oncolytic viral-based vaccine to treat a type of skin cancer called melanoma [95].
The challenge of vaccine development is to create an efficient delivery system for antigens that minimizes the antigen dose and prevents recognition by antigen presenting cells (APCs). Therefore, nanomaterials, with their many capabilities, serve as the basis for creating novel vaccines that generate strong, comprehensive immune responses [96]. Nanomaterials used for antigen delivery offers several advantages, including sustained and controlled release properties, high bioavailability, targeted delivery, and imaging capabilities due to their physicochemical properties [97]. Nanomaterials can provide a protective and controlled delivery of antigens, allowing for their sustained release and increased uptake by antigen-presenting cells (APCs) [98].
Various nanomaterial-based delivery systems, such as polymeric nanoparticles, solid lipid nanoparticles, co-polymer nanogels, and liposomes, have been developed for antigen delivery [95,98].
Current developments related to nanocarriers for vaccine delivery, such as antigen, can be categorized into three distinct groups:
Actively APC-targeting nanocarriers,
Passively APC-targeting nanocarriers,
Cytosolic delivery and smart nanocarriers.
Song, et al. combined a novel emulsion-type adjuvant PEG-b-PLACL, Span ® 85 and squalene to form a stable isotropic emulsion. The efficacy of the peptide-epitope-linked carrier (PELC) approach in stimulating cytotoxic T-lymphocyte (CTL) responses for the treatment of tumors was examined through a series of experiments. The formulation contained a combination of peptides or protein antigens derived from HPV16 E7, PELC nanoparticles, and CpG oligodeoxynucleotides. Results of in vitro and in vivo studies demonstrated that the PELC formulation was able to effectively protect the antigen from degradation and extend its release time. Furthermore, the vaccine was found to be highly effective in increasing the number of CD4+ T cells and RAH-specific CD8+ T cells, as well as the number of IFN-γ secreting cells, leading to a bolstered CTL response and antitumor effect in mice. These findings suggest that the PELC/CpG nanoparticle-formulated peptide antigens are a viable option for cancer immunotherapy [99].
Standley, et al. synthesized nanoparticles with acrylamide as a monomer, that can degrade in the acidic lysosomal environment and covalently bind to CpG oligonucleotide ligands and encapsulate ovalbumin (OVA) to co-deliver antigen and CpG. DCs can significantly enhance the production of interleukin-12, a cytokine that assists in T-cell activation, and costimulatory molecules by APCs when compared to free OVA, OVA-NPs, or OVA + CpG. The vaccination with particles containing both ovalbumin (OVA) and CpG DNA leads to a more robust CD8 T-cell immune response, increased secretion of the proinflammatory cytokine IFN-γ, and the induction of OVA-specific cytotoxicity [100].
Fox, et al. used anionic liposomes to carry the TLR4-agonist glucopyranoside A and the TLR7-agonist imiquimod. The synergistic adjuvant biases away from Th2 responses, as evidenced by decreased IL-5 and increased CD4+ T cells that produced interferon gamma upon antigen-specific stimulation of cells from immunized mice, when compared to the use of a single TLR agonist. This conclusion indicates that nanoparticles that combine multiple immunostimulants can produce a synergistic effect, which can be more powerful than the individual components on their own [101].
Rosalia, et al. studied vaccine delivery to DC via CD40-targeting using a multi-compound particulate vaccine with biodegradable poly(lactic-co-glycolic acid) nanoparticles (NP). This formulation encapsulating a protein Ag, Pam3CSK4 and Poly (I:C) and coated with an agonistic αCD40-mAb (NP-CD40). The experiment concludes that CD40-mediated delivery to DC of NP-vaccines, co-encapsulating Ag and adjuvants, efficiently drives specific T cell responses, and therefore, is an attractive method to improve the efficacy of protein-based cancer vaccines undergoing clinical testing in the clinic [102].
Hassan, et al. utilized multi-walled carbon nanotubes (MWNTs) in co-delivering antigen along with different types of immunoadjuvants to antigen presenting cells (APCs). They investigated the effective method to co-deliver OVA, CpG and αCD40 using MWNT to the APC. MWNT remarkably improved the ability of co-loaded OVA, CpG and αCD40 in inhibiting the growth of OVA-expressing B16F10 melanoma cells in subcutaneous or lung pseudo-metastatic tumour models. So, this study suggests that the utilization of MWNTs for the co-delivery of tumour-derived antigen, CpG and αCD40 could be a competent approach for effective tumours eradication [103].
Lizotte, et al. showed that inhalation of self-assembling virus-like nanoparticles from cowpea mosaic virus (CPMV) reduces established B16F10 lung melanoma and simultaneously generates potent systemic antitumour immunity against poorly immunogenic B16F10 in the skin. CPMV nanoparticles possess excellent stability, lack toxicity, and can be modified to incorporate drugs and antigens, making them highly beneficial for medical applications. Furthermore, their nanomanufacturing process can be easily scaled up for large-scale production. CPMV's immunogenicity, efficacy against poorly immunogenic tumours, and other advantageous properties make it an appealing, novel immunotherapy option for metastatic cancer [78].
Zupancic, et al. comprehensively studied co-delivery of antigen along with two adjuvants (Monophosphoryl lipid A, oligodeoxynucleotide cytosine-phosphate-guanine motifs (CpG)) by nanoparticles being crucial for dendritic cell activation. Comparing single vaccination to the co-delivery of an antigen along with two adjuvants, it was found that the latter approach led to a 3-fold decrease in cytotoxic memory on T cells and an increased antigen-specific immune response against B16.M05 melanoma. Furthermore, it stimulated at least 5 times the amount of IFN-γ cytokine-secreting cells and more than doubled the number of lymphocytes in the tumor microenvironment as compared to the control. The number of lymphocytes at the tumor site doubled with triple immunization with significant tumor reduction. The nanoparticle also showed strong immune responses against B16.M05 melanoma [104].
Riabov, et al. studied virus-like particle vector encoding PSA (VLPV-PSA) in male mice expressing human PSA and HLA-DRB1( * )1501 transgenes were vaccinated. In vitro experiments showed that mouse dendritic cells could be infected with VLPV-PSA, and that this infection could generate a strong immunological response to PSA when tested in vivo . A substantial proportion of splenic CD8-T cells produced IFNγ upon exposure to the immunodominant peptide PSA. The administration of combination VLPV-PSA vaccination significantly increased the production of IgG2a/b anti-PSA antibodies, resulting in an augmented immune response and a delay in tumor growth [105].
NPs can serve as carriers to not only present tumor-associated antigens, thereby inducing DC maturation and activating tumor-specific T cells in lymph nodes, but also provide an efficient delivery system for other types of antigens, such as cytokines, nucleic acids, adjuvants, and soluble molecules. Cytokines are essential regulators of immune responses, controlling cell growth, differentiation, and their effects. Despite their approval by the FDA for the treatment of cancer, safety and the potential for loss of blood circulation remain major concerns with their use.
The need for innovative vaccine and adjuvant delivery vehicles has been imperative. Adjuvants are substances which are capable of amplifying or augmenting the immune response to antigens by activating immune cells, thereby increasing the effectiveness of the immune response while reducing the risk of toxicity or side effects. The components of adjuvant may facilitate the targeting and/or controlled release of the antigen to antigen-presenting cells, as well as into the lymphatic system, in order to create a sustained immune response. Furthermore, they can reduce the degradation rate of the antigens [106,107]. Nanomaterials that are employed to act as adjuvants are commonly referred to as self-adjuvants or nanoadjuvants, as they possess inherent immunological regulatory properties that can be used to strengthen and enhance the body's immune response.
Nanomaterials offer an advantage when delivering both antigens and adjuvants simultaneously to avoid immune tolerance caused by the absence of “danger signals” which are usually produced by specific adjuvants when DCs encounter antigens when delivered separately [108,109]. Carbon nanotubes (CNTs), Poly(d,l-lactide-co-glycolide) (PLGA), acetylated dextran, and graphene-based nanomaterials have been demonstrated to be effective nano vehicles for use as self-adjuvants in tumor immunotherapy due to their ability to induce the uptake of antigens by antigen-presenting cells (APCs) and enhance the activation of these cells, resulting in an enhanced immune response against the tumor [109,110].
Fang, et al. reported that biological functionalization of polymeric nanoparticles (NPs) coated with cancer cell membranes, in combination with immunological adjuvants, may offer potential for anticancer therapy and could be utilized in vaccines to augment tumor-specific immune responses [111].
Jambhrunkar, et al. developed pristine mono-dispersed invaginated mesostructured hollow carbon spheres (IMHCSs) have been found to be a viable protein nanocarrier and adjuvant for enhancing the Th2-biased immune responses associated with vaccine delivery. IMHCSs possess the potential to provide a safe and effective means of stimulating the immune system [112].
Monoclonal antibodies (mAbs) are being utilized as a form of cancer therapy, either as a standalone treatment or as a supplement to other chemotherapy agents. MAb therapy for cancer has seen rapid growth due to its ability to specifically target cancer cells, providing potent antitumor effects. Traditional cancer drugs typically kill tumors by directly attacking them, and can often cause severe side effects. In comparison, cancer immunotherapy drugs activate or stimulate the body's own immune system to fight the tumor, often resulting in fewer side effects and enhanced immune response, making them a more effective treatment option [113]. Cancer immunotherapy drugs have the potential to be effective treatments, however, they are not without drawbacks. These include monoclonal antibodies triggering a series of cytokine releases that can lead to cytokine storms, more toxic side-effects, and decreased effectiveness of treatment. To combat these shortcomings, nanomaterials are being used to improve the effectiveness and reduce the toxicity of cancer immunotherapy drugs [17,114].
The United States Food and Drug Administration (FDA) approved the mAbs in cancer therapy. Bevacizumab, the first anti-VEGF monoclonal antibody, has been shown to significantly extend the survival time of patients suffering from metastatic colorectal, breast, kidney and lung cancers when used in combination with standard chemotherapy regimens [18]. Cetuximab is a monoclonal antibody that has been developed to specifically target and inhibit the epidermal growth factor receptor (EGFR). This antibody has been found to produce strong antitumor effects in patients with chemotherapy-resistant colorectal cancer [115].
The revolutionary hybridoma technology has been an immense success in the utilization of monoclonal antibodies in clinical trials. The modified nanomaterials, which are enhanced with antibodies, have the advantage of selectively delivering drugs to tumor cells and increasing permeability and retention of various antitumor cytotoxic agents within targeted cells [116]. The nanoparticles were modified to express an antibody that distinguishes the epidermal growth factor receptor, expressed by the cancer cells.
Wartlick, et al. formulated biodegradable nanoparticles modified by covalent attachment of the biotin-binding protein NeutrAvidin for the breast cancer. The surface of these nanoparticles was conjugated with trastuzumab (herceptin), a HER2 receptor-specific antibody, to target HER2-overexpressing cells and observe effective endocytosis [117].
Choi, et al. prepared iron oxide NPs and DOX-encapsulated multifunctional nano-carrier to act on tumor cells with anti-human epidermal growth factor receptor 2 (HER2) antibody drug Trastuzumab. The studies of nano-carrier indicated that cellular uptake and cytotoxicity to HER2 overexpressed SK-BR-3 (human breast cancer cells) were significantly increased, leading to an enhanced tumor regression [118].
The preparation of PEGylated multifunctional nanoprobes conjugated with CD44v6 monoclonal antibodies based on gold nanostars showed high affinity towards GCSC spheroid colonies and completely destroyed them, making it an ideal strategy to improve prognosis and reduce recurrence of gastric cancer. The CD44v6-GNS nanoprobes show great promise for use in gastric cancer targeted imaging and photothermal therapy in the near future [119].
Kirpotin, et al. prepared immunoliposomes bearing trastuzumab (Herceptin ® ), which targets human epidermal growth factor receptor (HER-2). The results revealed that immunoliposomes induced a much stronger anti-proliferative effect than trastuzumab alone [120].
Pal, et al. synthesized Cetuximab immunoliposomes (ILs) for delivery of boron compounds targeted to epidermal growth factor receptor (EGFR)-positive glioma cells. These studied showed that cetuximab-targeted treatment resulted in an 8-fold increase in boron uptake into the target cells, significantly improving the effectiveness of the boron payload delivery [121].
Fujita, et al. conjugated two different mAbs (OX26, a mouse anti-TF receptor mAb; 2C5, a mouse anti-nucleosome mAb) onto PLA to construct a dual-targeted immunopolymer NP (synthetic polymer NP) against brain tumors. The results of the studies indicated that the immunopolymer NPs carrying the tandem configuration of antibodies displayed increased efficacy compared to those carrying single configurations [122].
Kos, et al. prepared an immunopolymer NP by conjugating an anti-cytokeratin mAb to cysteine protease inhibitor (cystatin)-loaded poly(lactic-co-glycolic acid) (PLGA) NPs. The PLGA immunopolymer NPs loaded with cystatin effectively attached to breast cancer cells expressing cytokeratin, inhibiting the production of plasmin and promoting cell adhesion, thus preventing the spread of malignant cells. This was achieved through the cystatin blocking cathepsin B [123].
Colloidal Gold Nanoparticles (AuNPs) are an ideal contrast agent due to their small size, high atomic number and good biocompatibility. Nunes, et al. showed that AuNPs target cells through both active and passive mechanisms. Hybrid anti-HER2 gold nanoshells were injected into a mouse model of breast cancer that overexpresses the HER2 gene. This preclinical study has demonstrated the potential of anti-HER2 gold nanoshells and photothermal therapy to overcome trastuzumab resistance in HER2-overexpressing breast cancer [124].
Liang, et al. formulated nano vaccine composed of liposome-coated gold nanocages (Lipos-AuNCs), modified with the dendritic cell-specific antibody aCD11c to enhance the activation and maturation of dendritic cells and enhance tumor-specific T lymphocyte responses. This nano vaccine is further modified with the adjuvant MPLA and the melanoma antigen peptide TRP2, allowing for targeted delivery of these components. The targeted antigen/adjuvant-loaded liposomes-coated gold nanocages were shown to increase antitumor immune response, inhibiting tumor growth and metastasis in both B16-F10 prophylactic and lung metastasis models [125].
Chen, et al. formulated immunotherapeutic bio responsive in situ gel that controls both local tumour recurrence after surgery and development of distant tumours. In situ spraying of an anti-CD47 antibody-encapsulated calcium carbonate nanoparticle suspension into a fibrin gel was performed. The administration of an anti-CD47 antibody enhances macrophage-mediated phagocytosis of cancer cells, and also triggers T cell-mediated immune responses that suppress tumour growth and hinder recurrence and potential metastasis following surgery [126].
Mi, et al. utilized dual immunotherapy via coadministration of antagonistic antibodies such as antiprogrammed cell death-1 (aPD1) and agonistic antibodies such as antitumor necrosis factor receptor superfamily member 4 (aOX40). The studies revealed that T-cell activation was more precise, therapeutic efficacy was improved, and immunological memory was amplified [127].
The size of nanocarriers is a critical factor for their selection, as it affects their cellular uptake and can cause them to cluster in solution. Therefore, it is important to consider the size of nanocarriers when choosing them for a particular application.138-139 A recent study suggested that the size of oxide nanoparticles influences their propensity to aggregate when taken up by human pneumonocytes in vitro [128,129].
The shape of the particles is also an important parameter that affects their performance [130]. Studies have shown particle shape significantly affect their pathways into cells, cycling time, targeting effect, ability to overcome biological barriers, and other properties. This is due to their influence on the transport of particles in small vessels and tumour vessels, as well as on how cells perceive and respond to them. In particular, the shape and shape correlation factors, such as aspect ratio or geometric structure, can have a significant influence on the transport properties of particles and the interaction between the cells and the particles [131].
The surface charges of nanoparticles play a major role in their various biological performances, such as solubility, biodistribution, stability, cellular uptake, and cytotoxicity [132,133]. The electrostatic interactions between particles and cells play a crucial role in the functioning of biological processes [134]. Particle-to-cell attraction is mainly determined by the presence of molecules on the surface of the cell that interact with molecules on the surface of the particle. Protein-coated particles may help identify antigens or receptors, but they are not the primary factor in determining particle-to-cell attraction. The cell membrane, which is usually negatively charged, sometimes with a small amount of positive charge in patches, facilitates the adsorption of positively charged particles more easily than negatively charged or neutral particles due to its surface charge. Graf, et al., based on the study of silica nanoparticles, found that particles with a high positive charge can promote successful cellular internalization, whereas those with a negative charge or which are functionalized with poly(ethylene glycol) (PEG) have reduced cellular uptake.
Before they can be employed in clinical practice, nanoparticles must be thoroughly evaluated and assessed to ensure they are not toxic to humans [135,136] must be taken into account when selecting nanocarriers, as it is a critical factor. More research needs to be carried out in this respect. The toxicity of nanoparticles is dependent on a variety of factors, including size, shape, and concentration [137]. The adverse effects of nanoparticles on human health may be due to their interactions with biological systems in the body. In addition, the toxicity of nanoparticles is largely determined by their structure, particularly the core material. The release of hazardous substances resulting from the breakdown of nanoparticles is one of the primary ways that they can cause toxicity. An inorganic core or a silicon shell can be used to reduce decomposition of the material, either by being structurally stable on its surface or by being embedded in a cross-shaped polymer.
The design of nanomedicine is heavily reliant on the careful consideration and manipulation of the various parameters of nanoparticles, as demonstrated by strong theoretical and experimental results. These parameters influence the properties of the nanoparticles, and thus must be taken into account for the successful creation of nanomedicine. In order to optimize the application of nanomedicine treatment for cancer, it is essential to rationally adjust the aforementioned parameters in order to change the physicochemical properties of nanoparticles, such as permeability, drug loading, targeting specificity, and to overcome MDR while ensuring low toxicity. This will ultimately enable personalized tumor treatment [138].
In this review, we abridged the principles and applications of nanotechnology in cancer immunotherapy. Despite recent advances in immunotherapy, the complexities of tumors and the tumor microenvironment, potential off-target side effects, and low immunogenicity remain major obstacles for the successful treatment of cancer. Tumor-specific T cells are inhibited by the combined action of tumor cells, tumor-associated stromal cells, tumor-infiltrating immune cells, and various cytokines or chemokines. It is a major challenge to reactivate the immune response in this intricate system. Nanotechnology, with its unique advantages, can be a great boon to the field of cancer immunotherapy research by addressing the current problems and technical challenges therein. The exploration of cancer immunotherapy is entering a new era of possibilities with the emergence of nanotechnology and nanomaterials. Genetically engineered cells have been used to create PD-1-expressing cellular nanocarriers, which can be used to deliver small immunological molecules. These cellular nanocarriers offer a novel approach to targeted drug delivery and could potentially be used to improve the efficacy of therapies. These strategies are also expected to offer novel insights for tailored immunotherapy. Nanomaterials offer unique advantages for targeted delivery in cancer immunotherapy; however, their efficacy is hindered by the lack of control over their targeting abilities. The continual improvement of clinical data and the development of advanced measurement and characterization techniques are necessary for the successful application of nanomaterials. The impact of nanomaterials on human patients and clinical transformations has not been significant so far. The limited distribution of the delivered drug at tumor sites due to the selectivity and effectiveness of nanocarriers hinders the clinical application of nanomaterials. The potential toxicity of nanomaterials as a drug carrier needs to be further evaluated for safety. The pharmacokinetics of nanomaterials and their effects on the host immune system should be further explored using animal models, with particular attention paid to the various components involved. The clinical development of nanomaterials continues to pose many challenges and questions, yet the advancement of nanotechnology, the deepening of clinical research, and the design and fabrication of nanomaterials are paving the way for the development of safe and effective cancer immune-therapeutics. The future holds great potential for the merging and progression of nanotechnology and cancer immunotherapy.