Introduction: Spontaneous spinal epidural hematoma is a rare spinal pathology, which can result in serious morbidity and disability if not diagnosed promptly. The authors present a unique case of acute plegia in a patient with spontaneous spinal epidural hematoma secondary to herniated disc hemorrhage.
Case presentation: A 66-year-old male with a five-month history of progressive weakness in the upper and lower extremities with associated radiculopathy and numbness presented to the ED with physical exam significant for signs of cervical myelopathy. His presentation was further complicated with hemorrhaging into the spinal canal which required emergency decompression.
Discussion: The diagnosis of neurological disorders is complex and dependent on a thorough history and physical examination. Most patients present with severe radicular back or neck pain, followed by motor or sensory deficits. Hyperreflexia, Hoffmann reflex, Babinski sign, and clonus may be present on physical exam. Simple incorporation of quick upper motor neuron neurological tests can help differentiate upper motor neuron from lower motor neuron lesions. Further study is warranted but treating physicians should be aware of the subtle signs of SSEH present on physical examination.
Epidural hematoma, Epidural spinal cord compression, Trauma care
SSEH: Spontaneous Spinal Epidural Hematoma; OMT: Osteopathic Manipulative Therapy
Spontaneous spinal epidural hematoma (SSEH) is defined as blood within the epidural space that can mechanically compress the spinal cord. It is a rare spinal pathology, which can result in serious morbidity if delayed [1]. It accounts for less than 1% of all spinal canal space occupying lesions [2]. Although SSEH can occur throughout the spine, the most common location is in the cervicothoracic region [3]. The usual clinical presentation of SSEH is sudden stabbing neck or back pain that progresses toward paraparesis or quadriparesis. SSEH may have variable findings on physical examination depending on the level and size of the hematoma. Physical findings may include unilateral or bilateral weakness, sensory deficits with unilateral or bilateral radicular paresthesia, alteration of deep tendon reflexes, and alteration of bladder or anal sphincter tone [4]. A thorough and critical neurological exam and interpretation plays an important role in a clinical setting to raise suspicion of SSEH. We present a unique case of a patient with acute plegia with SSEH secondary to herniated disc hemorrhage. Initially the patient was diagnosed with cervical radiculopathy. However, with a critical neurological exam and interpretation, SSEH was suspected because in addition to the right-side hemiparesis, the patient presented with bilateral hyperreflexia and bilateral Hoffman's reflex indicating an upper motor neuron lesion, such as spinal cord compression.
A 66-year-old male with five-month history of progressive weakness in the upper and lower extremities with associated radiculopathy and numbness, was referred to the neuromuscular institute by his primary care physician for evaluation and management. The patient initially presented to his primary care physician describing a sharp, shooting pain located on the right upper back, radiating down his arms bilaterally. He recalled falling on his right shoulder off a step ladder. Physical exam revealed decreased range of motion and tender trigger points of the head, cervical and thoracic spine. He was diagnosed with neck pain and somatic dysfunctions to the head, cervical, thoracic, lumbar, sacrum, and innominate and was prescribed tizanidine and Medrol dose pack. Osteopathic manipulative treatment was performed to correct his somatic dysfunctions. The patient reported experiencing one week of relief after osteopathic manipulative therapy (OMT) and continued to receive six treatments in total over the following five months.
The patient was referred to physiatry after he reported new onset bilateral leg weakness and stopped benefiting from OMT and physical therapy. On presentation the patient reported numbness and tingling radiating to both upper extremities, right more than left, numbness down anterior thigh, the ball of the right foot and the 4th toe bilaterally, and muscle weakness in bilateral lower extremities and hands. He also reported new onset lower abdominal "band-like" numbness after his last physical therapy session. He expressed losing grip strength in the right hand and having difficulty tying his shoes. On examination, he was found to have right lower rhomboid atrophy, right foot drop, positive Romberg and spurling maneuver on the right, non-sustained clonus on the right ankle, and negative Hoffman and Babinski sign. Hyperreflexia decreased strength and sensation were noted on neurological exam (Table 1). Based on these findings, an urgent MRI of the cervical, thoracic, and lumbar spine was ordered to evaluate for cervical myelopathy and spinal cord compression and a trial of gabapentin and baclofen was prescribed for neuropathic pain and muscle spasms. The patient contacted the office one week later to report that he could not tolerate laying flat in the MRI without experiencing severe radiating neck pain. He also began walking with a cane because of increased instability, numbness and worsening right foot drop. He was advised to go to the emergency department for imaging under sedation and neurosurgical consultation.
Table 1: Physiatry office Motor, DTR, and Sensory exam. Each Motor reflex is scored out of 5. Each reflex is scored out of 4. View Table 1
The patient initially presented to emergency department with progressive upper and lower extremity weakness. Physical exam revealed right greater than left upper and lower extremity weakness, radiculopathy and decreased sensation in bilateral upper extremities and hyperreflexia in the right lower extremity. Neurosurgery recommended MRI under sedation or CT myelogram, which the hospital does not perform. He was transferred to another facility with those capabilities. The patient presented to the ED with physical exam significant for signs of cervical myelopathy. He exhibited Hoffman's sign bilaterally, clonus in the right ankle, and hyperreflexia in upper and lower extremities bilaterally. Babinski was absent. Weakness in right hand and lower extremity was seen on motor exam (Table 2). MRI of the cervical, thoracic, and lumbar spine were performed under sedation. It displayed severe cervical degenerative disease spanning from C2-C7, ossification of the posterior longitudinal ligament of the C5-C6 segment, and severe spinal canal stenosis with moderate to severe cord compression from C5-C6, C6-C7 (Figure 1 and Figure 2). Two hours after the initial MRI, the patient developed sudden onset right leg plegia and worsening motor weakness in his right hand (Table 3). A repeat MRI was performed and revealed a hyperacute hemorrhage surrounding the extruded C6-C7 disc was revealed through T1 weighted imaging. The patient underwent an emergent anterior posterior cervical decompression fusion involved laminectomy's from C3-7 and a posterior fusion with pedicle screws from C2-T1 (Figure 3). On postoperative day 6, there was some improvement in neurology, with a returning of lower extremity strength from 0/5 to 4/5 (Table 4). During a follow-up of 3 months after discharge, the patient reported relief of pain and full return of sensory and motor deficits.
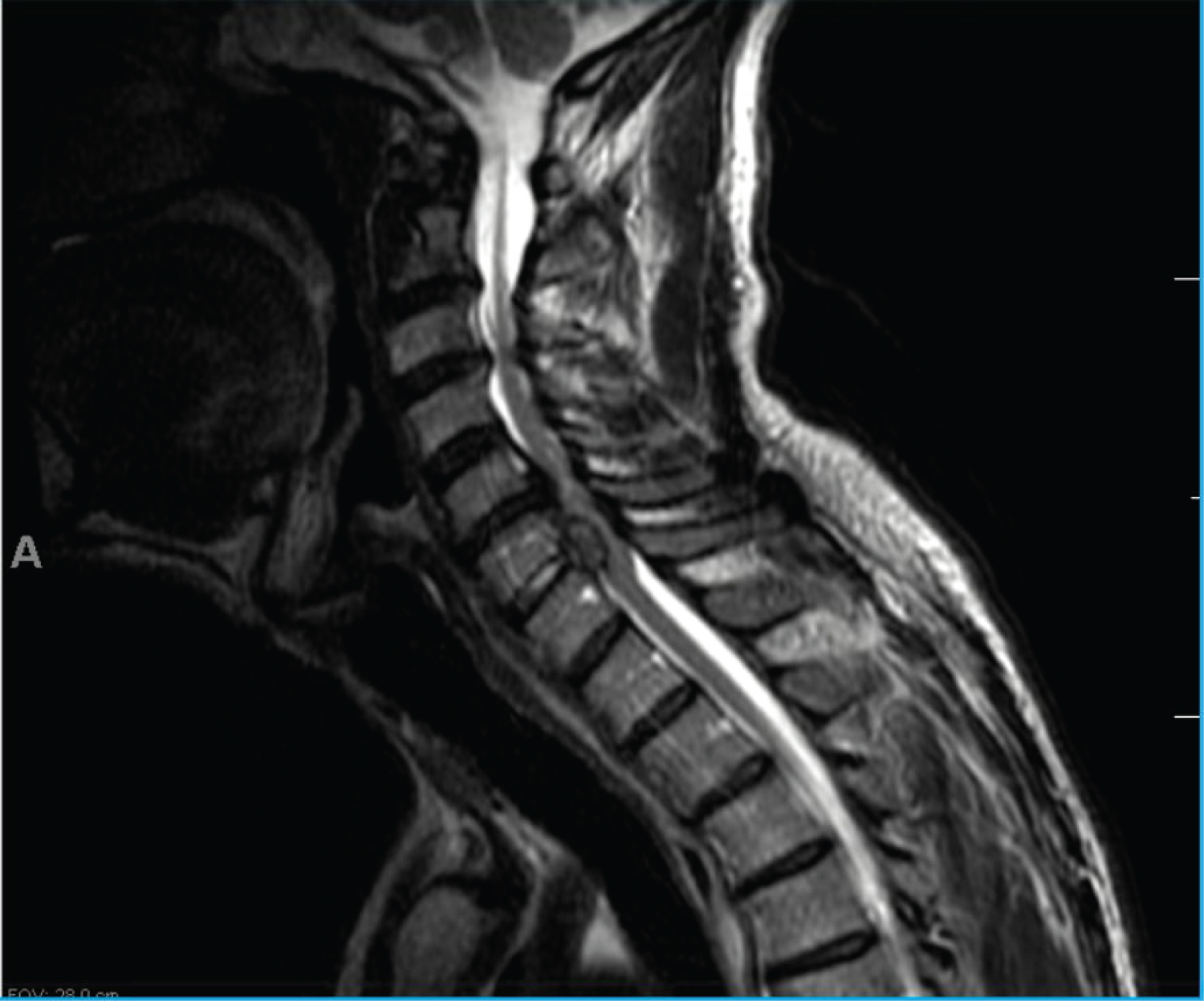 Figure 1: MRI of cervical spine shows a massive disc herniation at C6-C7 causing severe central canal narrowing. There is ossification of the posterior longitudinal ligament at C4-C6. 2 small foci of T2 signal hyperintensity in the left dorsal aspect of the cord at C5 level.
View Figure 1
Figure 1: MRI of cervical spine shows a massive disc herniation at C6-C7 causing severe central canal narrowing. There is ossification of the posterior longitudinal ligament at C4-C6. 2 small foci of T2 signal hyperintensity in the left dorsal aspect of the cord at C5 level.
View Figure 1
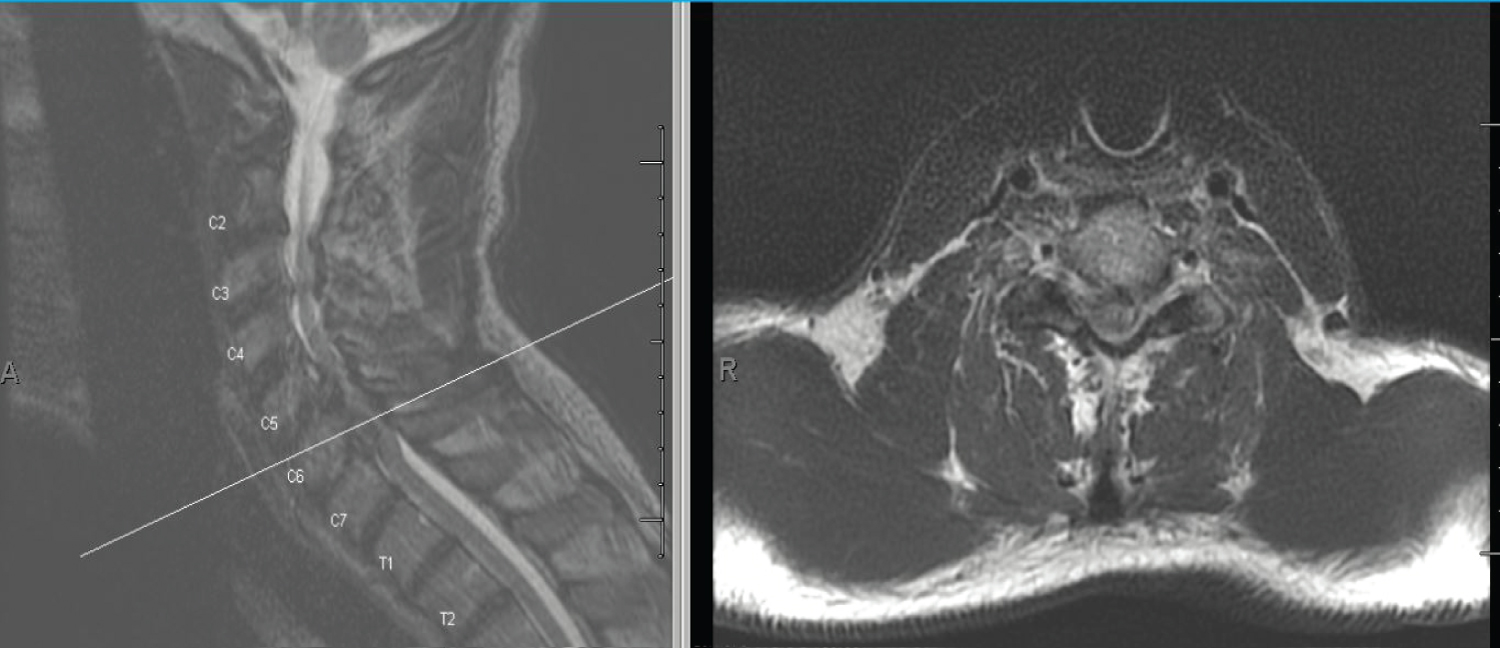 Figure 2: MRI of cervical spine shows a massive disc herniation at C6-C7 causing severe central canal narrowing. Cross-section.
View Figure 2
Figure 2: MRI of cervical spine shows a massive disc herniation at C6-C7 causing severe central canal narrowing. Cross-section.
View Figure 2
 Figure 3: Post-operative AP and lateral view X-rays after posterior instrumented fusion C2-T1 and anterior interbody fusion C6-C7. Decompression was performed posteriorly C3-C7 and anteriorly C6-C7.
View Figure 3
Figure 3: Post-operative AP and lateral view X-rays after posterior instrumented fusion C2-T1 and anterior interbody fusion C6-C7. Decompression was performed posteriorly C3-C7 and anteriorly C6-C7.
View Figure 3
Table 2: Neurosurgery, Preoperative Motor, DTR, and Sensory exam. Each Motor reflex is scored out of 5. Each reflex is scored out of 4. View Table 2
Table 3: Motor reflexes after the incident. View Table 3
Table 4: Motor reflexes after the surgical procedure. View Table 4
We present a unique case of acute plegia in a patient with spontaneous spinal epidural hematoma secondary to herniated disc hemorrhage. Neurological complaints and symptoms account for 5% of patients presenting to the emergency department [5]. The most common chief complaints were focal weakness, headache, dizziness, or vertigo [6]. In many neurological conditions, accurate diagnosis is critical because the patient outcomes are often dependent on prompt treatment. A study investigating the importance of a neurologist in the emergency room (ER) found that for 52.5% of the patients had a complete change of diagnosis from the initial diagnosis made by the ER physician [7]. Similarly, this was seen in our case. During the patient's initial encounter with the ER physician, he was diagnosed with cervical radiculopathy, which is consistent with upper and lower motor symptoms, but would not explain the upper motor neuron lesion sign such as a bilateral positive Hoffman's sign. However, after the neurosurgery consult the patient was diagnosed with cervical myelopathy, which explained the bilateral positive Hoffman's sign [8]. Thus, a thorough and critical physical exam becomes important to suspect the diagnosis of cervical myelopathy.
The diagnosis of neurological disorders is complex and dependent on a thorough history and physical examination. It helps you recognize and as a result, manage disease earlier in their course. A complete neurological examination should contain an assessment of sensorium, cognition, cranial nerves, motor, sensory, cerebellar, gait, reflexes, meningeal irritation, and long tract signs [9]. The patient's signs and symptoms depend on the location of the epidural hematoma and the degree of cord compression. There is a combination of severe pain and neurologic deficit. Most patients present with severe back or neck pain, often with a radicular component. After sudden and abrupt pain, motor or sensory deficits occur. The severity and progressiveness of sensory and motor deficit depend on the severity and progression of bleeding [10]. The severity of sensory and motor deficit has a prognostic value; patients with residual function are more likely to show complete recovery than those patients with no motor function [10,11]. A total of 37% of cases of SSEH show complete sensory and motor deficit, and the remainder of cases have some sensory or motor function intact [11]. The clinical picture of SSEH also depends on the location of the hematoma. SSEH may be presented as hemiparesis, hemiplegia, quadriparesis, quadriplegia, and other presentations [10,11].
A study investigating the sensitivities of pyramidal signs in patients with cervical myelopathy found that hyperreflexia showed the highest sensitivity followed by Hoffmann reflex, Babinski reflex, and ankle clonus. The prevalence of upper motor neuron signs correlated with increasing severity of myelopathy, especially with the severity of motor dysfunction in the lower extremities. Most notably, patients with ossification of the posterior longitudinal ligament were more likely to exhibit ankle clonus [12]. Sensation, deep tendon reflexes, clonus and Hoffman sign were not checked at our patient's initial emergency room visit. The presence of upper motor neuron signs such as hyperreflexia, Hoffman reflex, clonus, and Babinski sign is a hallmark of myelopathy which is considered a key component in the diagnostic process. His reflexes were not checked, missing the upper and lower extremity hyperreflexia and right ankle clonus. Hoffmann and Babinski reflexes were omitted, which could indicate an upper motor neuron issue [13]. Our patient exhibited a positive Hoffmann sign bilaterally indicating an upper motor neuron lesion such as cervical spinal cord compression or cervical myelopathy. In our case, our patient's radiological finding suggested the patient had spontaneous spinal epidural hematoma secondary to herniated disc hemorrhage, which necessitates prompt treatment to avoid serious morbidity or mortality.
Accurate diagnosis of cervical myelopathy is important because of the significant degree of disability associated with this condition. However, the diagnosis is often delayed, or the urgency of the situation is missed because of an incomplete neurological exam, which can lead to development of neurologic complications [13]. The ER can have an overwhelming number of patients that need to be seen and a thorough exam can be compromised. However, simple incorporation of quick upper motor neuron neurological tests, such as a glabellar reflex, Hoffman's reflex or cerebellar exam can help differentiate upper motor neuron lesions from lower motor neuron lesions. The physical exam is a valuable tool in the clinical setting. Early and accurate clinical diagnosis is the first step in the proper initiation of treatment modalities and improvement in overall patient outcome. Ultimately, further study is warranted, but treating physicians should be aware of the subtle signs of SSEH present on physical examination.
DJR and SEM contributed equally to this work in study design, data collection, interpretation of data, drafting and revising the article. JWB supervised this study and patient's treatment and provided final approval of this version for submission.
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient.
The authors have no relevant financial or non-financial interests to disclose.
All authors declare that they have no conflicts of interest.