Paraplegia is common following thoracoabdominal aortic aneurysm (TAA) repair. It results from ischemia of the anterior spinal cord in the distribution of the anterior spinal artery and causes anterior spinal cord syndrome. However, this young patient with asymptomatic idiopathic TAA developed pure motor incomplete paraplegia with elevated creatinine phosphokinase levels following repair. The possible etiologies are discussed along with a description of her subsequent rehabilitation and outcomes over the following six weeks.
Thoracic aortic aneurysm, Anterior cord syndrome, Myopathy, Spinal cord injury, Case report
Paraparesis without sensory loss, specifically with respect to pain and temperature sensation, is a rare or never-reported complication of thoracic abdominal aneurysm (TAA) repair. The most common and well-known complication is anterior cord syndrome (ACS), due to ischemia in the distribution of the anterior spinal artery. We present the case of a young woman who underwent repair of an asymptomatic TAA found incidentally on imaging, following presentation to the emergency department. Following open repair of the TAA, she reported lower-extremity weakness without sensory loss. To the best of our knowledge, this is the first case report of ischemic myopathy after TAA repair.
The incidence of TAA is 5-6 per 100,000 people per year, most of which are in the elderly population [1]. By definition, a TAA involves three layers of the arterial wall with a minimum 50% increase in diameter at the aneurysm compared with the rest of the aorta [2]. TAAs are either saccular or fusiform in morphology. Fusiform is the most common type and is symmetrical and pan-circumferential in nature [3]. TAAs generally arise from cystic medial necrosis and/or medial degeneration, leading to a decrease in the number of smooth muscle cells and elastin degradation [1]. Physiologically, as the wall stress increases, the diameter of the aorta increases. There are known risk factors for TAA related to the development of atherosclerosis, including hypertension, age, and hyperlipidemia [1]. Known genetic syndromes such as Marfan syndrome and an increasing number of mutations are associated with the development of TAA [4]. More than 95% of TAAs are asymptomatic up to the point of rupture or dissection [5]. The risk of rupture or dissection increases with increasing aneurysm diameter, with some variance based on the aneurysm location [6].
One of the most feared complications of TAA repair is paraplegia/paraparesis of the lower extremities due to ischemia of the anterior two-thirds of the spinal cord. The blood supply to this portion of the cord comes from the anterior spinal artery, which is fed by the anterior segmental medullary vessels from the aorta, the largest of which is the artery of Adamkiewicz [7]. In open repairs, such as in our patient, the risk was between 8-30% [8]. The usual presentation is flaccid paraplegia/paraparesis and loss of pain/temperature sensation due to involvement of the lateral corticospinal tract and lateral spinothalamic tract, respectively. Light touch and proprioception are preserved given the separate blood supply of the dorsal/posterior columns. Here, we present a case of lower-extremity ischemic myopathy following open repair of TAA.
A 36-year-old woman with no significant past medical history presented to the emergency department with worsening suprapubic pain that had been present for 4-5 months and was found to have a urinary tract infection and symptomatic endometriosis. In the emergency department, computed tomography (CT) showed an incidental 7.3-cm descending thoracic aortic aneurysm. On presentation, the patient was hemodynamically stable with a heart rate of 116 bpm. She said that this could be normal during times of anxiety. On physical examination, she was noted to have normal pulses, well-perfused limbs, and to have moved all extremities appropriately, signaling no neurologic deficit at that time. She lacked any signs of marfanoid habitus. Laboratory results were notable only for hypokalemia, with a value of 2.9 mEq/L. She underwent a CTA confirming the diagnosis of a tortuous descending thoracic aortic aneurysm located at the distal thoracic component with aneurysmal dilation of 6.3 × 5.6 cm with no evidence of dissection or rupture (Figure 1). It is important to note the patient denied any family history of Marfan Syndrome and denied a family history of aneurysms. She also did not have any atherosclerotic risk factors, such as hypertension, hyperlipidemia, or diabetes mellitus, and was a lifetime nonsmoker. Upon genetic counseling, she was not found to have any known genetic associations with aortic aneurysms, including Marfan syndrome and Ehlers-Danlos syndrome.
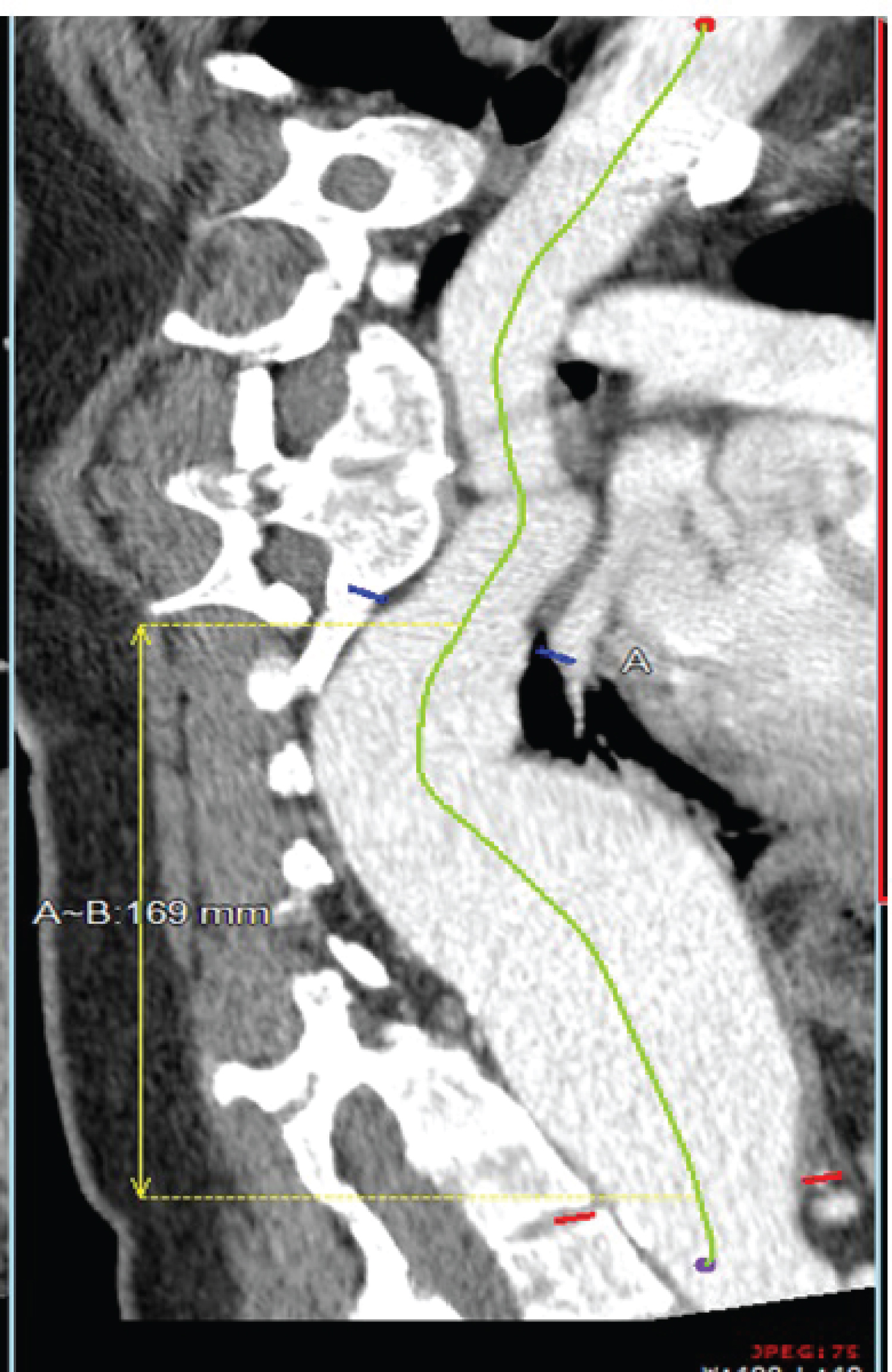 Figure 1: CT of the chest confirmed a greater than 6 cm thoracic aneurysm extending from the mid-descending thoracic aorta to the arch of the celiac artery.
View Figure 1
Figure 1: CT of the chest confirmed a greater than 6 cm thoracic aneurysm extending from the mid-descending thoracic aorta to the arch of the celiac artery.
View Figure 1
The patient was discharged from the emergency department and was instructed to follow-up in the clinic to determine her treatment plan. Subsequently, open repair of the type III thoracoabdominal aneurysm was deemed most appropriate. Seventeen days passed between her initial presentation to the ED and her repair. The evening before the operation, the patient had a CSF spinal drain placed without complications. The patient was placed in the right lateral decubitus position under general anesthesia, with the right femoral artery A-line placed under ultrasound guidance. A circumferential thoracoabdominal incision was made in the left second intercostal space to expose the proximal aneurysm end. The left femoral artery and vein were exposed to distal limb perfusion via femoral-femoral cannulation and a centrifugal pump. There was adequate control of the proximal and distal aorta without complications, allowing placement of a 24 cm Hemashield© Graft. No significant intercostal arteries were used for reattachment. The aortic clamps and cannulas were removed without any complications, and the patient was transferred to the ICU while intubated. Intraoperative data showed an operative time of 4 hours, aortic clamp time of 38 minutes, an estimated blood loss of 1.5 L, an episode of SVT that responded to medication, and an episode of hypotension during aortic clamping that responded to pressors and intravenous fluids, and blood product resuscitation culminating in a total of 4 L. The mean arterial pressure (MAP) was greater than 80 mmHg, except for six brief instances throughout the surgery.
On the evening following surgery, the patient remained intubated with 10 mL of fluid removed hourly from the spinal drain. Her MAP was maintained at greater than 90 mmHg. Following extubation, the patient was noted to have bilateral foot movements; however, the proximal muscles of the lower extremities were profoundly weak, but she had an intact sensation. Her MAP was maintained at > 110 mmHg and her baseline hemoglobin level was maintained at > 10 g/dL. On postoperative day three, a physical medicine and rehabilitation team was consulted to evaluate the patient with a presumptive diagnosis of ischemic myelopathy. However, the surgeon noted that the examination was atypical, observing "the muscles are just twitching when she tries to move." On physical examination, her upper extremities were normal in terms of strength, reflexes, and all modalities of sensation. Her motor exam results were also intact with respect to her chest and abdomen, including an absent Beevor's sign. Her lower-extremity motor examination was as follows: Hip adductors graded 0/5 bilaterally, hip flexors graded 0/5 bilaterally, knee extensors graded 1/5 bilaterally, toe extensors graded 1/5 bilaterally with slightly increased strength on the left, plantar flexors graded 2/5 bilaterally with a half-grade greater strength on the left, and hip abductors/external rotators graded 2/5 with a half-grade greater strength on the left. Thus, her pattern of muscle weakness was most severe in the L2-3 innervated muscles and weaker on the right side than on the left. Lower extremity reflexes were absent and there was no Babinski sign. The lower extremity sensation was intact with light touch and proprioception. Unexpectedly, the sensation of pain and temperature in the lower extremities remained intact. No distinct sensory level was observed in this patient. Of note, she had an intact sensation in the perineal area and anal contraction. Over the following few days, serial physical therapy muscle examinations revealed a similar motor examination that did not change prior to discharge. Although she continued to complain of moderately severe aching in her muscles, rated between 5 and 10/10 on the pain scale as recorded by the nursing staff, the patient's sensory examination remained normal. The patient had urinary retention after surgery without bladder spasms and continued to stay at an inpatient rehabilitation center. Urology consultation prior to discharge was thought likely due to "postoperative urinary retention". The urinary retention resolved. At the rehabilitation hospital, she progressed through therapy and was ultimately discharged to her condo with a modified independent status using a wheelchair. She was even able to go up 16 stairs on her bottom using her arms but was still unable to walk. At six weeks, the greatest muscle grade remained at no greater than 2/5. To date she still has not experienced any signs of spasticity and exam findings remain asymmetric. Currently, she is still awaiting further diagnostic testing consisting of imaging and electrodiagnostic testing.
Incomplete paraplegia following TAA repair is common, affecting up to 8-22% of patients [9,10]. However, the patient's condition was unremarkable. She is a young patient. She did not have any known genetic markers for Ehlers-Danlos or Marfan syndrome. The patient presented with symptomatic endometriosis. However, similar to 95% of patients with TAA, the hers were asymptomatic. Her aneurysm may have been congenital but certainly idiopathic. Postoperatively, instead of anterior cord syndrome, she developed only muscle weakness (pure motor incomplete paraplegia) following TAA repair.
Our patient was at risk of ischemic myelopathy. Her aortic clamp time was > 30 min, and she had intraoperative hypotension. The patient had a complex aneurysm. However, given the findings of this patient's physical examination, she did not meet the criteria for a diagnosis of anterior cord syndrome, given the sparing of the lateral spinothalamic tract.
We hypothesized that the same mechanisms that cause spinal cord ischemia may also cause muscle ischemia. This could lead to muscle injury or death (ischemic myopathy), given sufficient aortic clamping, blood loss, hypoxia, or hypotension during open repair. We suspected myopathy, given her lack of sensory loss, and the left side was stronger. The right side was down during the operation, and the left side was superior on the operating table; thus, the left side was not subjected to direct pressure effects, which can contribute to ischemic muscle [11]. The CPK level was first measured on postoperative day three and was markedly elevated at 1403 mcg/L. Presumably, it was higher immediately after surgery and trending downward, with the pattern noted after the highest result. This information, combined with our examination findings, made our most likely diagnosis of ischemic muscle injury, ischemic myopathy.
However, other diagnoses were also possible. Endometriosis has been reported in the spinal cord causing paraplegia; in this case, the conus medullaris [12]. Endometriosis can cause nerve impingement and lumbosacral plexopathy; however, both are expected to cause sensory and motor loss. Bilateral anterior spinal artery embolic stroke has been reported in literature [13]. We did not perform arteriography of the brain. Ascending polyradiculopathy, such as Guillain-Barre syndrome, can cause paraplegia but is expected to progress. Anterior horn cell diseases such as polio, West Nile virus, or post-enterovirus infection can cause pure motor paraplegia, but this presentation on awakening after surgery would be surprising; she presented with no other symptoms of infection and did not have any diarrheal symptoms in the 2-3-week window before the surgery.
Could she have had an anatomical variation in which ischemic myelopathy spared her sensation? Could her spinothalamic tract pass through the posterior columns, thus sparing pain and temperature sensations? Alternatively, could the spinothalamic tract be less sensitive to ischemia than the corticospinal tract (or her anterior horn cells)? If so, she would have presented this way. Perhaps, she had arteriolar branches of her anterior spinal arteries that led to a different blood supply to the motor and sensory fibers. In our literature search, neither of these possibilities was reported. However, there is extensive literature on the variation in the artery of Adamkiewicz [14]. In time, she hopes to arrange for further imaging studies and electrodiagnostic testing; which as of now is a limiting factor in the confirmation of our suspected diagnosis.
We reviewed all of this information with the patient. The patient wanted to learn more about the diagnosis and prognosis. She was interested in being the subject of this case report, and she provided written informed consent.
This is the first case report of a patient who developed pure motor paraplegia after repair of a thoracoabdominal aneurysm. She continues to slowly improve.
Peyton Miles and Dr. Jeff Hecht wrote this case report.
The authors confirm that they have no competing interests, received no funding for the project, have no financial benefits, and there has been no previous presentation of the research, manuscript, or abstract in any form.
The authors confirm equal contribution by each individual author.
The patient involved in this case report provided informed consent.
No funding was received for this study.
All relevant data are within the paper and its supporting information files.
The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interests in the subject matter or materials discussed in this manuscript.
The authors declare that they have not previously presented this research, manuscript, or abstract.