Primary large B-cell lymphoma of immune privileged sites (IP-LBCL) is a rare B-cell lymphoma that arises in the central nervous system (CNS), vitreoretinal tissues, and testis of immunocompetent patients. A search of the health records in the Canadian province of Newfoundland and Labrador over 10 years identified three cases. We highlight pertinent clinical and microscopic features from these cases and discuss the differential diagnosis of this uncommon condition.
According to the 5 th edition of the WHO classification of hemato-lymphoid neoplasms, primary large B-cell lymphoma of immune-privileged sites (IP-LBCL) is a rare B-cell lymphoma that arises in the central nervous system (CNS), vitreoretinal tissues, and testes of immunocompetent patients [1]. Excluded from this category are lymphomas that arise in these same sites in immunodeficient patients, as well as those which involve these sites secondarily. These three anatomical regions are designated as “immune-privileged” because they each contain blood-barriers. Primary large B-cell lymphomas of these sites are therefore combined into one category and share morphologic, immunophenotypic, and molecular features. Given that these sites normally lack regular lymphoid tissue, the etiology of this lymphoma and its cells of origin are still completely unknown [2,3].
A search from the health records of Newfoundland and Labrador, Canada, over 10 years identified three cases meeting these diagnostic criteria.
This 80-year-old male presented with bilateral testicular swelling. Ultrasound examination revealed bilateral enlargement with almost complete replacement of the testicular parenchyma. His lactate dehydrogenase level at diagnosis was 179 U/L.
He underwent bilateral sequential orchiectomies. Microscopy showed a diffuse infiltrate of large atypical lymphoid cells that stained positive for CD20, BCL6, BCL2 and MUM-1 with a Ki-67 proliferative index of 60%. CD3, CD5, CD10, CD30, and EBER-ISH were negative. There was no bone marrow involvement. Central nervous system involvement was ruled out via cerebrospinal fluid cytology. Six months prior to presentation, the patient had a diagnosis of basal cell carcinoma involving the left ear which was managed by radiation. He received six cycles of R-CHOP chemotherapy and five intra-thecal methotrexate therapies for prophylaxis. Various follow-up imaging studies, including CT and PET scan, were negative for recurrent disease and indicated complete metabolic response to treatment. Two and a half years after completion of therapy, scrotal examination revealed no evidence of recurrent testicular masses.
A previously healthy 58-year-old man presented with a 3-month history of a painless enlarging right testis. He had no constitutional symptoms. Staging CT and PET scan demonstrated one small lymph node in the right paratracheal region, but otherwise no adenopathy or evidence of systemic involvement was identified. His lactate dehydrogenase level at diagnosis was 172 U/L. His family history was positive for bowel cancer in his father. In terms of substance use, he smoked one pack of cigarettes per day, drank three to four alcoholic drinks per week, and occasionally smoked marijuana. He worked for the Coast Guard and had multiple chemical exposures over his lifetime. After initial workup, he went on to have a right orchiectomy. Microscopy showed a diffuse sheet of centroblastic cells that stained positive for CD20, BCL2, and MUM1 with a Ki-67 proliferative index of 70%. Staining was negative for CD3, CD5, CD10, BCL6, CD30, and EBER-ISH (see Figure 1). Overall this was consistent with a diffuse large B-cell lymphoma, activate B-cell type. He received six cycles of R-CHOP chemotherapy and five intra-thecal methotrexate therapies for prophylaxis. This was followed by contralateral radiotherapy. He was in a state of clinical remission until October 2019, approximately 10 months after his last chemotherapy treatment. At this time, he was discovered to have a CNS relapse in the left frontal lobe of the brain after presenting with seizures. He received high-dose methotrexate and Ibrutinib. Despite this, his disease progressed and he received palliative radiotherapy before passing away from his disease.
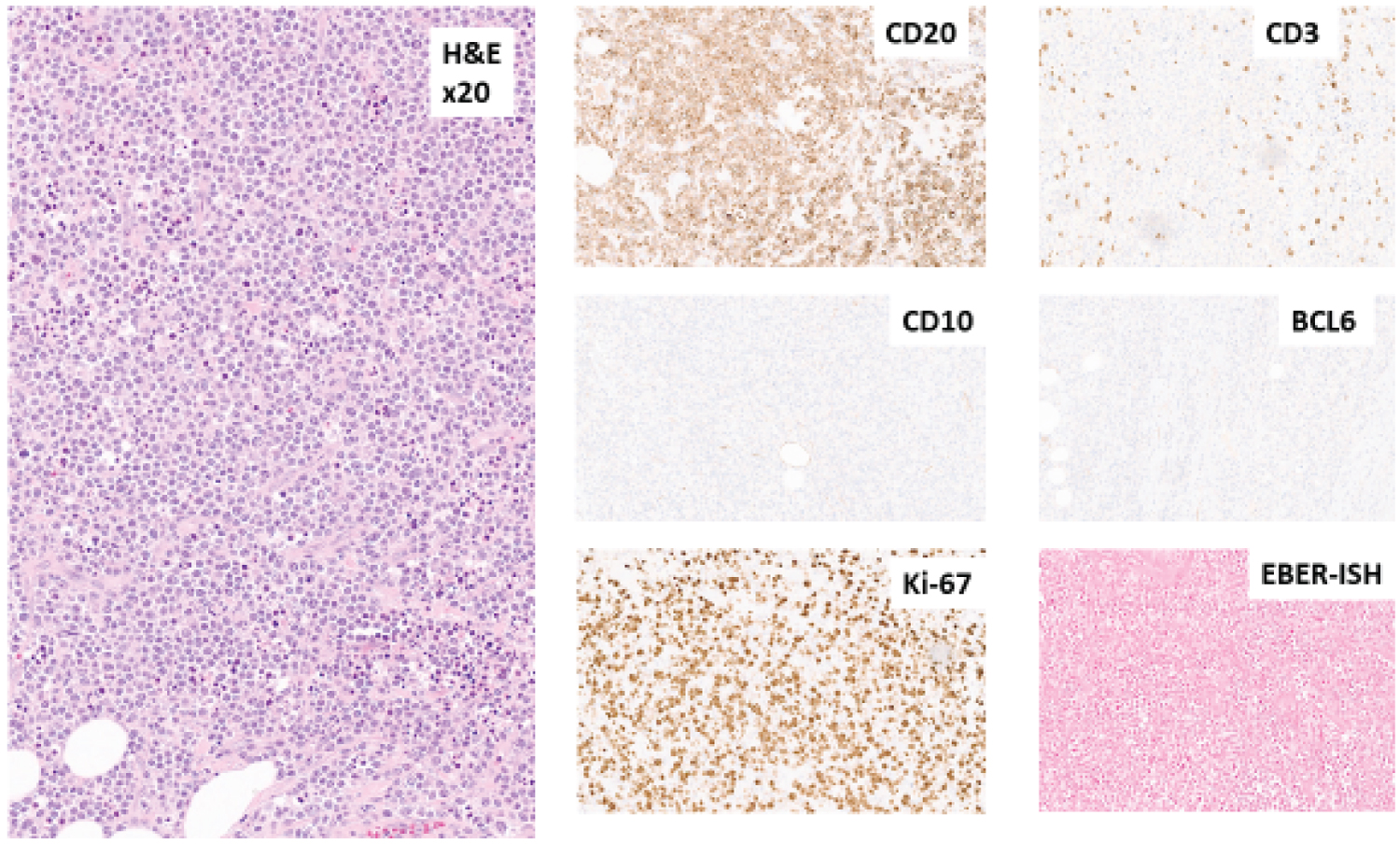 Figure 1: Microscopy from of orchiectomy specimen from patient #2 showing an infiltrate of large lymphoid cells, positive for CD20 but negative for CD3, CD10, BCL6. Ki67 proliferative index is 70%. EBER-ISH is negative.
View Figure 1
Figure 1: Microscopy from of orchiectomy specimen from patient #2 showing an infiltrate of large lymphoid cells, positive for CD20 but negative for CD3, CD10, BCL6. Ki67 proliferative index is 70%. EBER-ISH is negative.
View Figure 1
This 80-year-old male had been having chronic pain and discomfort in his right testis. Despite being treated with doxycycline for presumed epididymal orchitis, his symptoms and swelling persisted. Otherwise he had no palpable lymphadenopathy or hepatosplenomegaly. He had a minor history of smoking but quit over 50 years prior to his diagnosis. He rarely drank alcohol and worked as a welder in the dockyard. There was no known family history of any hematologic malignancies. His blood work during workup showed a total white count of 8.5 × 10 9 /L with a hemoglobin of 131 g/L and platelet count of 411 × 10 9 /L. His lactate dehydrogenase was elevated at 454 U/L. Immunoglobulins were normal and viral serology was negative. He was reported as Stage IVB after thorough clinical and radiological assessment.
Orchiectomy was performed and microscopy showed a diffuse infiltrate of large lymphoma cells with brisk mitosis. By immunohistochemistry, these were positive for CD20, CD79A, weak CD5, BCL6, BCL2 and MUM1. Ki-67 proliferative index was greater than 80%. Tumor cells were negative for CD3, cyclin D1, SOX11, CD10, CD30 and EBER-ISH, confirming a diagnosis of diffuse large B-cell lymphoma of post germinal center origin. His molecular testing showed no MYC, BCL6, or BCL2 gene rearrangement. Treatment included six cycles of R-CHOP chemotherapy and involved-field radiation therapy to the contralateral testicle. He is currently in clinical remission.
Only 3 cases of primary testicular lymphomas were seen over 10-years in the Canadian province of Newfoundland and Labrador. Microscopy from all three cases showed a diffuse large B-cell lymphoma, non-germinal center phenotype with negative EBER-ISH. Two of these occurred in older males, both diagnosed at 80 years of age, who are currently in clinical remission after chemotherapy and intrathecal methotrexate with prophylactic irradiation to the contralateral testis. The one patient that was younger developed a worse clinical outcome with CNS involvement.
Primary testicular lymphomas are uncommon, accounting for 1-2% of all non-Hodgkin lymphomas. They occur predominantly in older men during or after the 7 th decade of life, with a median age at diagnosis of 67-years in the USA. The majority of patients clinically present with painless unilateral testicular enlargement and show associated constitutional symptoms such as fever and weight loss. Over 90% present with localized disease (stages 1 and 2). Bilateral testicular involvement is seen in about 35% of patients. An interesting observation of this entity is the pattern of relapse and propensity for extra-nodal sites such as the central nervous system and contralateral testis [4,5].
The majority (80-90%) of primary testicular lymphomas are diffuse large B-cell lymphoma, non-germinal center phenotype with activated B-cell like gene expression profile (GEP) subtype. These cases tend to display a diffuse intertubular infiltration growth pattern with recognizable tubular remnants and perivascular growth patterns comprised of medium-to-large cells with moderate-to-high mitotic activities and a variable degree of tumor necrosis. Precursor intratubular germ cell neoplasia is absent. Testicular lymphomas are often positive for CD45 and CD20, but they are negative for OCT3/4 and placental alkaline phosphatase [6,7].
Clinical and histologic mimics of primary testicular lymphomas include germ cell tumors (such as classic seminoma, spermatic seminoma, and embryonal carcinoma), as well as granulomatous and viral orchitis. One of our three cases was clinically suspected to be a persistent epididymal orchitis. Seminomas tend to occur in younger males and microscopically have distinct cell membranes, abundant glycogen-rich cytoplasm, and rounded but focally flattened central nuclei with one or few prominent nucleoli. Seminomas stain for antigens characteristic of immature, fetal-type germ cells, including placental alkaline phosphatase, KIT, OCT3/4, SALL4, SOX17, and podoplanin. They lack expression of CD30 and alpha-fetoprotein. Embryonal carcinoma has a characteristic epithelioid appearance that frequently forms glandular, papillary, or tubular structures. Serum markers like alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG), and lactate dehydrogenase (LDH) are useful in diagnosis and disease monitoring. Embryonal carcinoma is a germ cell tumor characterized by primitive epithelial cells with marked pleomorphism and various histologic patterns. It may present in pure form but often is part of a mixed germ cell tumor. Tumor cells stain positive for cytokeratin A/E, CD30, and OCT3/4. They are negative for CD45, CD117, D2-40, and glypican 3. Viral and granulomatous orchitis have a patchy distribution with polymorphic inflammatory cellular infiltrates.
An orchiectomy is usually performed as part of the diagnostic and therapeutic approaches as it provides specimens that allow for thorough pathologic diagnosis and removes a potential “sanctuary site”, as the blood-testis barrier makes testicular tumors inaccessible to systemic chemotherapy [7]. Due to the high risk of contralateral testicular involvement during progression, the uninvolved testis is often irradiated. Similarly, prophylactic intrathecal methotrexate may reduce CNS involvement during relapse or progression. Genomic analyses have shown that both primary and relapse LBCL-IP appear to have a common progenitor cell with minor genetic alterations. These minor alterations may reflect clonal evolution of LBCL-IP [3].