Idiopathic scrotal calcinosis is a benign disorder characterized by the deposition of calcium salts in the skin layers of the scrotum, leading to the formation of painless nodules. We present a 60-year-old Thai male patient diagnosed with idiopathic scrotal calcinosis. The patient presented with multiple hard nodules in the scrotal region, a characteristic finding of this rare condition. He did not report any associated symptoms, such as pain or discomfort. The diagnosis was confirmed through pathological examination. Surgical excision was performed on the patient with no complications or recurrence in a two-month follow-up. We reviewed relevant research and clinical studies to better understand the etiology and optimal management strategies of idiopathic scrotal calcinosis.
Idiopathic scrotal calcinosis (ISC) is defined as a rare and benign condition marked by the deposition of calcium in the scrotal dermis, resulting in the development of variable-characteristic single or multiple calcified nodules. The scattered lesion can also be fused into clusters [1-3]. The epidemiology reveals that ISC is a disease of childhood or early adulthood, typically presented in the third decade of life [4,5]. The patient typically has the same presentation: Asymptomatic, indolent, and progressive, with lesions increasing in number and size, raising aesthetic concerns. Other reported presentations consist of mild heaviness, which can also be exhibited in a case with a large lesion, the oozing of chalky content discharge from the lesion, breaking down of the lesion, and infection, with some patients complaining of apruritic sensation at the lesion [2,5,6]. The main components of the nodule are calcium and phosphorus [4].
First studied by Lewinski in 1883, ISC was described as a subtype of the calcinosis cutis [4]. Calcinosis cutis is an abnormal deposition of insoluble calcium salts in skin and subcutaneous tissue [7]. There are five subtypes of calcium deposition, each typically characterized by a lack of overt symptoms. Firstly, the nutritional disorder type arises from tissue damage despite normal calcium and phosphorus levels. Secondly, the exogenous type results from the side effects of drug therapy, such as those based on bleomycin or poppy. Thirdly, the idiopathic type lacks a metabolic cause or tissue damage. Fourthly, the metastatic type is characterized by an abnormal calcium and phosphorus metabolism in patients, promoting calcium deposition. Lastly, the calcification-resistant type involves the calcification of small blood vessels and adipose tissue, leading to manifestations like penile injury and scrotal nodules [8]. As mentioned earlier, idiopathic calcinosis cutis is a distinct subtype that manifests without any underlying tissue anomaly, damage, or metabolic disorder, of which scrotal calcinosis is a specific form [7]. This condition was later termed ISC by Shapiro in 1970 [1]. Shapiro, et al. posited the idiopathic nature of the condition following a thorough histopathologic examination of 14 cases featuring ISC, revealing a conspicuous absence of a cyst wall structure. This proposition has garnered support from subsequent studies. Conversely, certain investigations have presented findings indicative of an epithelial lining [5]. From a histological perspective, ISC can be identified by the presence of calcium deposits of diverse sizes within the dermal layer, frequently encased by a foreign body-type granulomatous reaction [3].
The pathogenesis of this disease remains unclear due to its rarity, resulting in knowledge being limited to case reports and series [4,9,10]. Treatment nowadays mainly involves the surgical excision of lesions for both diagnostic and therapeutic purposes [10].
We report a case of ISC in a 60-year-old Thai male patient who underwent a complete surgical excision with primary closure of the scrotal skin. The patient provided consent for the publication of this case report. Given the remarkable rarity of this disease, we deem it essential to present this case along with a comprehensive review of the relevant literature.
A 60-year-old Thai male sought medical attention at the surgical clinic due to the manifestation of multiple slow-growing nodules on both sides of his scrotum, a condition that had been progressing for one year. The patient did not recollect any precipitating events, such as trauma or infection, which could have catalyzed the development of these scrotal lesions. Initially, he noticed the presence of asymptomatic, indurated nodules without any associated purulent discharge, with their number gradually increasing over the year. It is noteworthy to mention that the patient had a documented history of recurrent pleural tuberculosis five years earlier. Comprehensive tests, including a chest X-ray and an acid-fast bacilli (AFB) stain, yielded negative results, conclusively demonstrating the patient’s treatment and recovery from tuberculosis. Notably, beyond his previous experience with pleural tuberculosis, there were no documented systemic or metabolic comorbidities.
Upon a comprehensive physical examination (Figure 1), the patient exhibited multiple non-tender, solid nodules, ranging in size from 1 to 5 cm in diameter, localized on the scrotal skin adjacent to the median raphe. There was an absence of any overt signs of inflammation. We examined both testes and found no discernible abnormalities or clinical evidence of inguinal lymphadenopathy. It is worth noting that the patient did not present with similar cutaneous lesions on other anatomical regions of his body, and an exhaustive physical examination failed to disclose any additional remarkable findings.
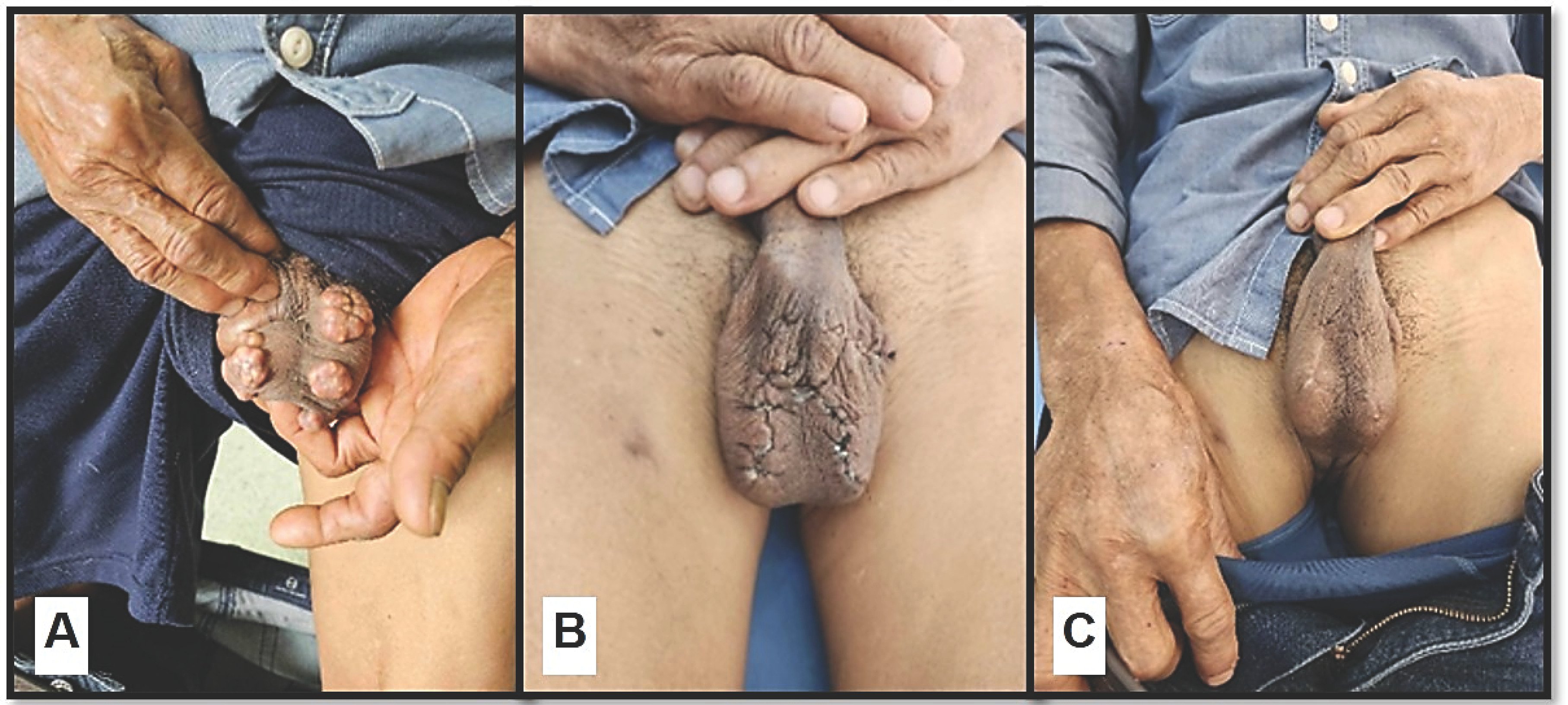 Figure 1: (A) Multiple, painless, hard nodules found underneath the skin of the scrotum; (B) After excision of the masses; (C) Two-month follow-up on the patient with complete wound healing.
View Figure 1
Figure 1: (A) Multiple, painless, hard nodules found underneath the skin of the scrotum; (B) After excision of the masses; (C) Two-month follow-up on the patient with complete wound healing.
View Figure 1
Furthermore, laboratory analysis of the patient’s serum indicated unremarkable levels of calcium, phosphate, and uric acid (Table 1). The patient then underwent successful surgical excision of the scrotal nodules under spinal anesthesia. Primary wound closure was achieved, with all excised nodules subsequently transferred to the pathology laboratory for further in-depth analysis.
Table 1: Preoperative laboratory investigation. View Table 1
A macroscopic pathological examination (Figure 2) of the scrotal lesion revealed multiple firm-to-hard nodules covered with unremarkable skin. The surrounding skin showed no surface erosion or ulceration. The size of the nodules varied from 0.5 to 2 cm in diameter. The cut surfaces of the specimens show chalky yellow-white masses with a firm-to-hard consistency. Microscopic findings (Figure 2) revealed multiple granular calcium deposits in the dermis and subcutaneous tissue. Chronic inflammation was also observed as well as multinucleated giant cells. The patient was followed up two months after the excision, with no post-surgical complication or recurrence present.
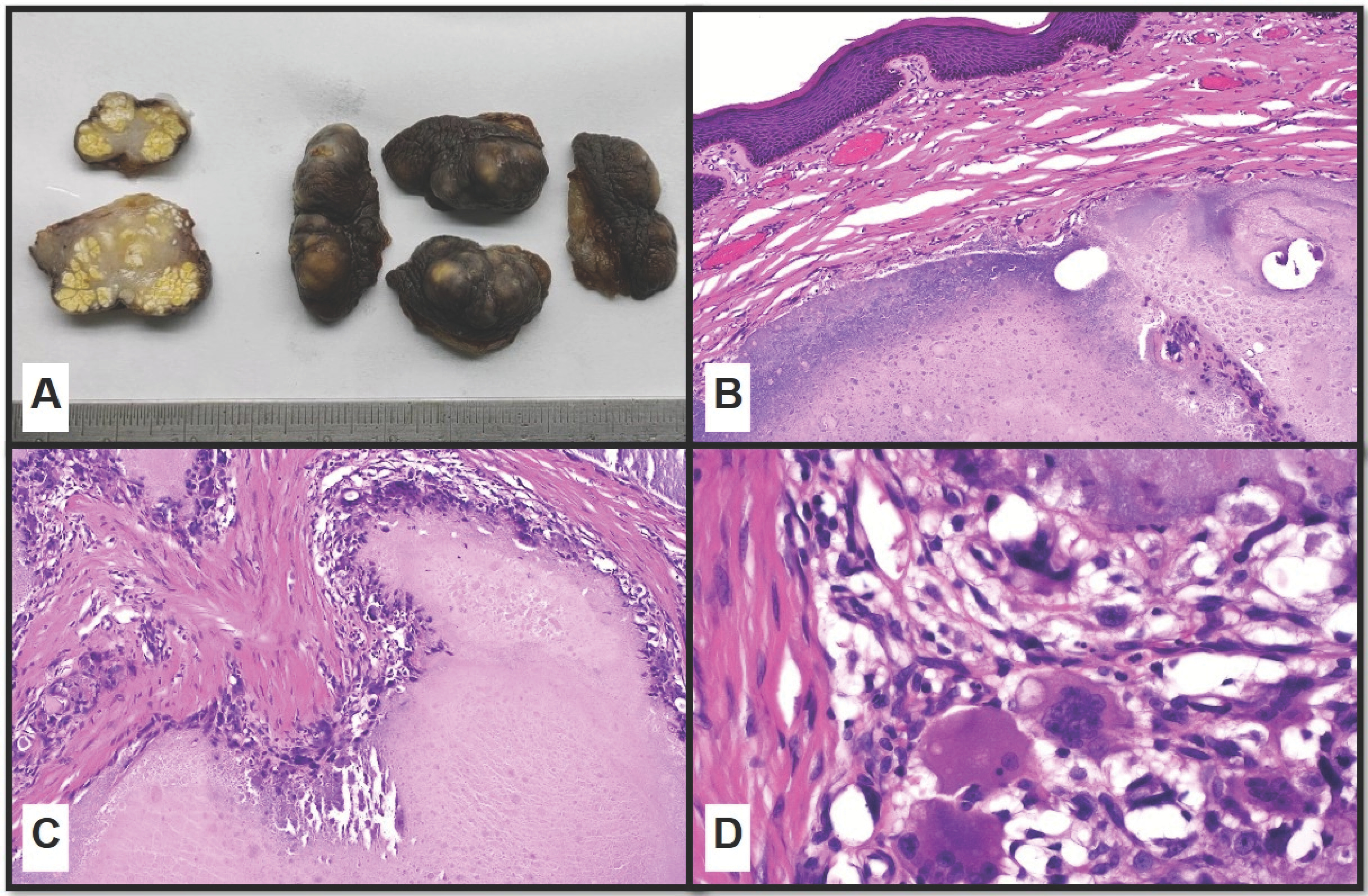 Figure 2: (A) Scrotal skin excision demonstrating skin with underlying yellow-white, well-circumscribed nodules composed of calcified material; (B) Low-magnification showing the calcified area with overlying unremarkable skin (H&E, 40x); (C) Medium-magnification showing the calcified area with surrounding fibrosis and chronic inflammation (H&E, 100x); (D) High-magnification showing multinucleated giant cells (H&E, 400x).
View Figure 2
Figure 2: (A) Scrotal skin excision demonstrating skin with underlying yellow-white, well-circumscribed nodules composed of calcified material; (B) Low-magnification showing the calcified area with overlying unremarkable skin (H&E, 40x); (C) Medium-magnification showing the calcified area with surrounding fibrosis and chronic inflammation (H&E, 100x); (D) High-magnification showing multinucleated giant cells (H&E, 400x).
View Figure 2
ISC predominantly impacts men aged 20 to 40 and usually initiates in childhood or adolescence. Most patients present with multiple scrotal nodules that are firm, ranging in color from yellowish to white and varying in size from several millimeters to centimeters. While the condition is typically benign and asymptomatic, occasional symptoms may include itching or the discharge of chalky materials [3,10,11].
ISC is diagnosed through both clinical and histological assessment. Factors such as size, number, skin surface involvement, and age of onset serve are indicative parameters for the presence of ISC. Confirmation is typically attained through histopathological examination [12]. A nodular lesion in the scrotum can be associated with multiple potential differential diagnoses, encompassing a variety of conditions, such as epidermal inclusion cysts, steatocystoma, scrotal lipodystrophy multiplex, angiokeratoma, solitary genital leiomyoma, and dermatomyositis, particularly the juvenile subtype [5,12]. Additionally, other relevant considerations involve conditions like scleroderma, especially in patients with CREST syndrome (calcinosis cutis, Raynaud phenomenon, esophageal dysfunction, sclerodactyly, and telangiectasia), pilomatricoma, and nodular variant of scabies [5].
Epidermal inclusion cysts, commonly referred to as sebaceous cysts, stand out as the most prevalent type. Typically benign, these cysts are filled with keratin and are often associated with inflammatory reactions. They are frequently misdiagnosed as abscesses due to the outflow of keratin, prompting many physicians to perform incisions and apply antibiotics [8]. Despite their generally benign nature, around 1% of these cases may progress to squamous or basal cell carcinoma. Some authors propose that epidermal inclusion cysts can evolve into ISC over time [5].
In contrast to ISC, steatocystomas are characterized by skin-colored soft nodules ranging from 1-3 cm in diameter. Darker than ISC, angiokeratomas of Fordyce present as red to purple papules (2-5 mm in diameter) with surrounding erythema of the scrotal skin. Solitary genital leiomyomas, originating from the dartos muscle tissue, manifest as single or multiple firms, non-tender pink to red-brown papules, appearing deeper in the tissue than ISC [5].
It is essential to consider CREST as a relevant differential diagnosis because calcinosis cutis is observed in 25-40% of cases, particularly involving fingers and pressure points. Clinically presenting as rock-hard nodules that may exude white chalky material similar to ISC, calcinosis cutis should be carefully considered. In dermatomyositis, 30% of adult cases and 70% of juvenile dermatomyositis cases present with subcutaneous yellow-white nodules, plaques, and ulceration, with typical locations excluding knees and elbows, unlike ISC [5].
Furthermore, scrotal lipodystrophy multiplex is a disease requiring differentiation. It can occur at any age, featuring rubber-like hard nodules that release sebaceous or oily material. In contrast, scrotal calcinosis typically occurs in children or adults without a family history, with harder nodules that break down and exude sand-like particles or cheese-like material [8].
As an idiopathic condition, the exact etiology is unknown, prompting an intense debate challenging its idiopathic nature. Many authors argue that ISC is a misnomer and the underlying cause is the dystrophic calcification of the pre-existing epidermal cystic components of the scrotum, the most suggested theory by many authors being a possible pathogenesis, sebaceous cyst, and eccrine epithelial cyst, and this issue is still subject to debate [1,4,7,9,10,12-16]. Dartos muscle degeneration causing dystrophic calcification, emerging de novo without any triggering metabolic condition, infiltration of foreign body material, or induced by trauma have each been hypothesized as an etiology [1,4,6,7,10,16]. Some authors liken the calcification process to that of uterine leiomyomas [6].
Most epidermal inclusion cysts originate from epithelial inflammation, which is secondary to excessive collagen synthesis around blood vessels and adipose tissue. This surplus synthesis can lead to rupture and calcification, resulting in the deposition of calcium salts. Another contributing factor is extraosseous calcification caused by nanobacteria, which can invade the skin through micro trauma sites without causing overt features of infection [13,14]. A notable characteristic of nanobacteria invasion is the formation of calcium apatite crystals at neutral pH and at the physiological levels of blood calcium and phosphate [14].
However, some researchers propose that the foundation of scrotal calcinosis (SC) lies in dystrophic calcifications within the dartos muscle. They suggest that the initial events in the pathogenesis of the disease involve the degeneration and necrosis of the dartos muscle [4,9,14,15]. Dystrophic calcifications are typically triggered by inflammation, leading to the loss of their epithelial lining and the resorption of cyst walls, ultimately leaving behind only calcific deposits in older lesions [3,4,9,14,15,17]. In a study by Song, et al. where 51 nodules were examined from a patient with SC, the findings revealed that epidermal cysts experienced mild to moderate inflammation. This was followed by mononuclear cell or foreign body granuloma formation, culminating in the resorption of cyst walls and keratinous material until only calcified deposits remained. One crucial observation was the rapid resorption of the cyst wall, marking a significant stage in the sequence [18]. Histopathological findings of SC vary depending on the age of the cysts, leading to long-term cysts having fewer or no epithelial lining cells [3,17]. Wollina, et al. also emphasized a major distinction from calcified cysts, highlighting the complete absence of a lining epithelium [19]. In a study by Chakrabarti, et al. fine-needle aspiration (FNA) and smears stained with May-Grunwald Giemsa (MGG) and hematoxylin and eosin (H&E) revealed an amorphous basophilic substance suggestive of calcific deposits, with no evidence of epithelial cells. The absence of epithelial cells in the aspirate aided in cytologically differentiating this condition from a calcified epidermal cyst [20].
The etiology of ISC has been the subject of prolonged controversy. Initially, ISC was considered genuinely idiopathic, given the absence of cellular elements, cysts, lipids, or organisms within the calcified nodules. However, subsequent studies have suggested that ISC might originate from the dystrophic calcification of epidermoid cysts, epithelial walls, and keratin fibers [16]. Nevertheless, the true idiopathic nature of ISC remains a possibility. In their comprehensive review of histologic data, Shapiro, et al. found no evidence of an epithelial lining, residual cysts, lipids, or organisms. Consequently, they concluded that the calcification was indeed idiopathic, coining the term “idiopathic scrotal calcinosis” [11].
The current treatment modalities for ISC encompass medication, follow-up observation, laser or cryotherapy, and surgery [8,13]. Among these options, conservative treatments like medication and follow-up observation are ineffective, while laser or cryotherapy may lead to recurrence [13]. Attempts to treat ISC with drugs such as corticosteroids, diltiazem, sodium edetate, and fibrin phosphate, in combination with a low-calcium diet, have shown partial improvement in symptoms for only some patients [8].
Given these limitations, surgical excision followed by primary closure or complex scrotal reconstruction remains the primary management approach [1,4,6-8,10,12,13,15]. The risk of recurrence is a matter of debate, with some authors emphasizing a high probability after primary excision [15]. Many authors suggest complete excision of all minute nodules to prevent recurrence [7,9,12,15]. Although surgical excision may have associated complications, the results are definitive, and the recurrence rate is low if complete excision of all nodules can be achieved. Therefore, surgical intervention is the recommended approach for managing ISC. The primary indications for surgical removal include the presence of clinical symptoms (such as pruritic sensations, the occurrence of white material discharge, etc.) and/or the patient expressing concern about aesthetic disfigurement [7,8]. Surgical excision should be confined to the scrotal skin since calcified nodules are limited to the dermis, leaving the dartos layer intact. The high laxity of scrotal skin allows for the easy closure of large cutaneous defects with interrupted sutures, ensuring good scrotal coverage and an excellent cosmetic outcome [5,6,10]. However, Tela, et al. argue that the unique cosmetic and functional features of scrotal skin can complicate reconstruction. They advocate for the conservation of the scrotum’s rugae nature to ensure satisfactory testicle function, spermatogenesis, and a good cosmetic outcome [16]. Reconstruction modalities mentioned include mesh skin grafts and skin flaps from the groin or a medial circumflex femoral perforator flap [14]. The procedure is typically performed under local or spinal anesthesia, allowing time for more complex reconstruction to be accomplished [1].
Indeed, surgical management aids in confirming the diagnosis of SC through histologic examination [15]. Conversely, Chakrabarti, et al. have proposed fine-needle aspiration cytology (FNAC) as a valuable tool for diagnosing this rare disorder. A diagnosis by aspiration cytology may, at times, offer comfort to both the patient and the treating physician, potentially helping to avoid unnecessary surgery [20].
An intriguing therapeutic approach involves the use of the CO 2 laser, an ablative laser commonly employed in the treatment of various dermatological conditions. This procedure is purported to be less invasive, with reduced tissue loss and a favorable aesthetic outcome. According to a study by Cannarozzo, et al. CO 2 laser treatment demonstrates a superior aesthetic outcome compared to traditional surgery, sparing scrotal tissue with minimal risk of complications and scarring [21].
To the best of our knowledge, 23 pieces of literature on idiopathic calcinosis of the scrotum have been reported since 1997 (Table 2) [1-17,19-24]. The table compares the clinical features, overall disease courses, and treatment selection of 23 published studies. Most authors observed no postoperative complications and reported satisfactory or good cosmetic outcomes following surgical excision and primary closure within the 3-30 months postoperative period [1-5,7-10,12-15,17,20,24]. However, Kyei, et al. (multiple nodules) documented a single recurrent nodule, measuring 5 mm at 30 months of follow-up [1]. Salvarci, et al. (33 nodules) reported a single recurrent nodule, measuring 8 mm at 19 months of follow-up [23]. Despite the asymptomatic nature of the disease, it can impact patients’ marital relationships. In some cases, patients experienced stress, believing the nodule was related to a transmissible disease, leading to the avoidance of sexual intercourse. Other patient concerns included issues related to cosmesis and itching, adversely affecting their overall quality of life [1,4,6,16].
Table 2: Twenty-three cases of idiopathic scrotal calcinosis in previous literature. View Table 2
ISC is an uncommon skin disease characterized by the accumulation of calcium in the tissue of the scrotal skin. The primary therapy for this condition is surgical removal of the lesion, which has shown significant and impressive outcomes. This disease must be distinguished from epidermal inclusion cysts with calcification, scrotal lipodystrophies, and other calcified disorders like scabies nodules.
This case report was approved by the Faculty of Medicine, Chiang Mai University Human Research Ethics Committee (approval number: HOS-2566-0609). This research was conducted in accordance with the Good Clinical Practice (ICH GCP). In this case report, the patient was de-identified, and the need for written consent was waived following a review by the ethics committee.
This work was supported by the Faculty of Medicine, Chiang Mai University [grant number 53-67].
Data will be made available upon request.
The authors declare no conflict of interest.
No additional information is available for this paper.
The authors would like to extend their gratitude to Ms. Naorn Sriwangdang for her assistance in preparing the proposal.
All the authors listed have contributed significantly to the investigation, development, and writing of this article.