Context: Malaria is a major health problem in India leading to anemia, thrombocytopenia, and leukopenia, and also damages the kidneys and liver if left untreated. Evaluation of hematological parameters and biochemical correlation play an important role in malaria.
Aims: The aims were to analyze the distribution of demographic data, clinical and pathological characteristics, hematological parameters, and biochemical tests in malaria.
Settings and design: From January to December 2021, a retrospective observational study using a cross-sectional approach was conducted at a tertiary care center.
Methods and material: The study included 47 malaria cases and 47 healthy controls. The study examined symptoms, and frequency of changes in hematological, and biochemical parameters. Laboratory values were recorded and analyzed for associations.
Statistical analysis used: Data were evaluated using SPSS version 26 (trial version), compared the study groups with the control group using standard t-tests to identify statistically significant differences. The ANOVA test was used to analyze biochemical tests. Findings with a p-value below 0.05 were deemed to be of statistical significance.
Results: P. vivax was the most commonly observed species, at 43 (91%), while P. falciparum accounted for 4 (9%) of cases. Out of 47 cases, 31 were males; the majority of the cases belonged to people 13-30 years of age. The most frequent hematological abnormalities were normochromic normocytic anemia and thrombocytopenia. The study shows significant mean values for hemoglobin (HB), hematocrit (HCT), red cell distribution width (RDW), total leukocyte count (TLC), and platelet count (PC), but not for mean cell volume, mean corpuscular hemoglobin, and mean corpuscular hemoglobin concentration. The correlation of hematological parameters with parasitemia grades was statistically insignificant. Hyperbilirubinemia was the most common. Blood urea was elevated in more cases than creatinine.
Conclusions: Plasmodium vivax was the most common malaria species in our region, predominantly affecting males of young to middle age. Early diagnosis and management could be facilitated by monitoring HB, HCT, RDW, TLC, and platelet values. Kidney and liver function assessments could prevent organ damage.
Malaria, Anemia, Thrombocytopenia
ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; CBC: Complete Blood Count; HCT: Hematocrit; ICAMI: Intercellular Adhesion Molecule I; LFT: Liver Function Test; MCV: Mean Corpuscular Hemoglobin; MCHC: Mean Corpuscular Hemoglobin Concentration; PFEMP: Plasmodium Falciparum Erythrocyte Membrane Protein I; P. vivax : Plasmodium Vivax; P. falciparum: Plasmodium Falciparum ; PTC: Platelet Count; RBC: Red Blood Cell; RDW: Red Cell Distribution Width; RFT: Renal Function Test; WBC: White Blood Cell
The most common malaria species was Plasmodium vivax , mainly affecting males of young to middle age. Evaluation of hematological and biochemical parameters facilitates early diagnosis and prevents morbidity and mortality.
Malaria stands as a significant global health issue [1]. The latest data from the World Health Organization (WHO) in 2023 indicate that there were approximately 249 million instances of malaria across 85 countries where the disease is prevalent in 2022, a slight increase from 244 million cases in the previous year. Notably, India and Indonesia were responsible for 94% of malaria-related fatalities within the South-East Asia Region [2]. This disease is caused by Plasmodium protozoa , which are transmitted by female Anopheles mosquitoes when they bite. Other less common transmission methods include blood transfusions, needle sharing, and from mother to child during pregnancy [2]. Plasmodium thrives in warm, humid conditions and is particularly prevalent in India during the months from July to November, with states such as Gujarat reporting high numbers of Plasmodium vivax ( P. vivax ) and Plasmodium falciparum ( P. falciparum ) cases [3,4]. The incubation period for P. vivax typically ranges from 8 to 17 days, while for P. falciparum , it ranges from 9 to 14 days [5]. Infection with malarial parasites leads to alterations in blood composition, resulting in a range of blood disorders including anemia, thrombocytopenia, changes in white blood cell counts, and abnormal platelet function and count [6].
The purpose and objectives of this study were to examine the distribution of demographic data, observe the clinical and pathological characteristics, assess and evaluate hematological parameters, and investigate and correlate biochemical tests with malaria.
From January to December 2021, a retrospective observational study using a cross-sectional approach was conducted at the Central Hematology Laboratory within the Pathology Department of a tertiary care center.
The study was approved by the ethical committee and was conducted according to the Declaration of Helsinki. (PJR/2022/42).
The study included 47 individuals previously diagnosed with malaria and 47 healthy controls for comparative purposes.
The study welcomed cases that exhibited positive smears for at least one species of malaria parasite. It considers both patients receiving inpatient care and those treated as outpatients.
This study did not include patients whose malaria diagnosis was solely determined through rapid antigen detection tests.
Patient information, such as age, sex, clinical manifestations, symptoms, and initial diagnoses, were gathered from inpatient medical records and outpatient laboratory systems. Hematological analyses involved the collection of 2-4 mL of venous blood using EDTA vacutainers. The blood was processed and analyzed within 2-4 hours of collection using the Sysmex KX-21 automated 3-part hematology analyzer. The recorded data included hemoglobin (HB), hematocrit (HCT), total leukocyte count (TLC), differential leukocyte count (DLC), and platelet count (PC).
Blood smear analysis revealed thin and thick smears. A thick blood smear was considered negative if no parasites were detected across 100 oil-immersion fields. Parasite density in thick smears was quantified using a plus system scale to indicate parasitemia levels in positive cases: + (1-10 parasites per 100 thick-film fields), ++ (11-100 parasites per 100 thick-film fields), +++ (1-10 parasites per thick-film field), and ++++ (more than 10 parasites per thick-film field) [7].
Peripheral blood smears (PBS) were meticulously reviewed under various magnifications for red blood cell (RBC) morphology, TLC, DLC, platelet sufficiency, and malarial parasite type. Serum samples from the patients were analyzed to determine liver function indicators using Xl-640, a fully automated biochemistry analyzer. Serum bilirubin (both direct and indirect), aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and serum proteins were measured. Renal function was assessed using a fully automated Erba XL-640 biochemistry analyzer, and serum creatinine and blood urea levels were recorded.
Demographic and hematological data, including variables such as HB, RBC count, HCT, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), red cell distribution width (RDW), PC, mean platelet volume (MPV), and platelet distribution width (PDW), were evaluated using SPSS version 26 (trial version). This analysis compared the study groups with the control group using standard t-tests to identify statistically significant differences. Additionally, a biochemical examination was conducted on serum bilirubin, serum creatinine, and blood urea levels in malaria patients using the ANOVA test of analysis. Findings with a p-value below 0.05 were deemed to be of statistical significance.
Throughout the study period, the Central Hematology Laboratory of the Pathology Department conducted 56,774 complete blood counts. Of the 2,469 individuals tested for malaria, 47 were confirmed to have the infection through peripheral blood smear examinations and were enrolled in the current study. Among these patients, 14 were admitted as inpatients, and 33 were treated as outpatients. Most cases were documented from July to October.
Among the 47 confirmed cases, P. vivax was the predominant species, with 43 cases accounting for 91% of the total. P. Falciparum was identified in 4 of the cases, representing 9% of the sample (Figure 1).
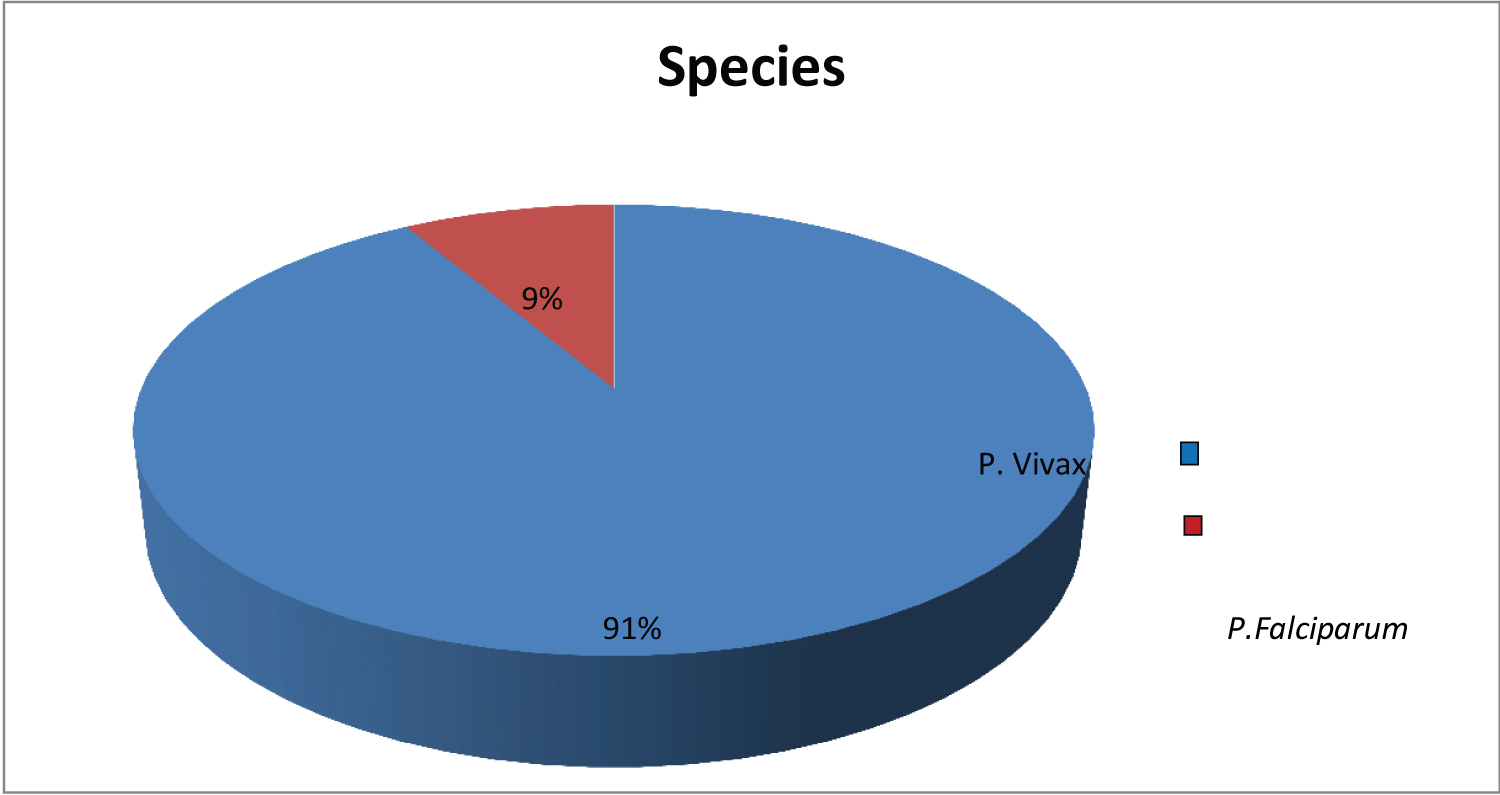 Figure 1: Species distribution of the present study.
View Figure 1
Figure 1: Species distribution of the present study.
View Figure 1
The study observed a predominance of male participants, constituting 31 individuals (approximately 65.95%), whereas female participants numbered 16 (34.04%) (Figure 2).
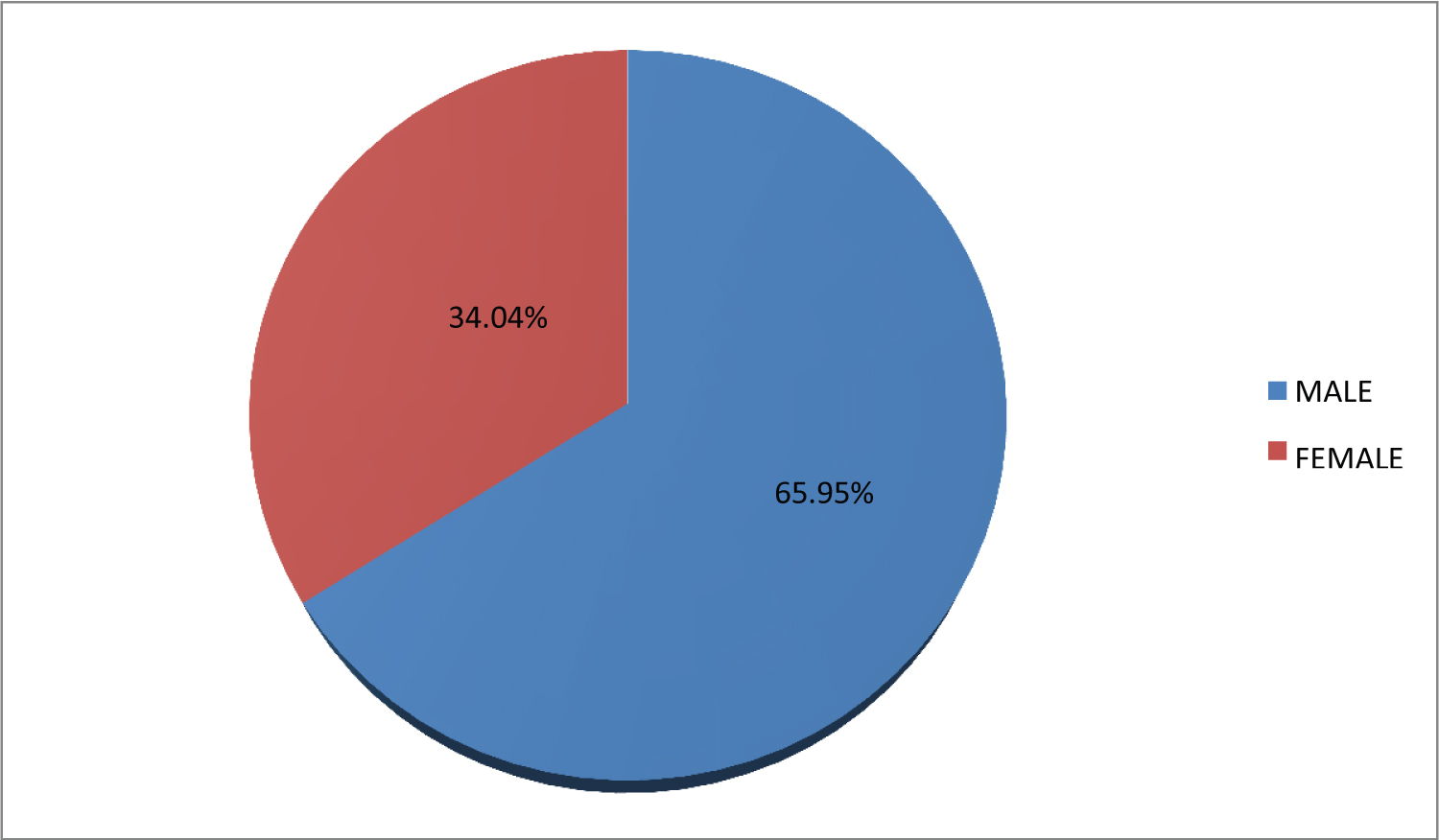 Figure 2: Sex distribution of the present study.
View Figure 2
Figure 2: Sex distribution of the present study.
View Figure 2
As shown in Figure 3, the participants ranged in age from 13 to 60-years-old. The mean age of participants was 32 years. The majority of the patients were in the 16-30 years age group, followed by those 46-60 years (Figure 3). Within the age group, a significant majority (91.4%) of the subjects were diagnosed with P. vivax infection, whereas the rest (8.1%) were diagnosed with P. falciparum infection. Of the 31 males, the majority were infected with P. vivax (n = 28, 90.3%), while the remainder were infected with P. falciparum (n = 3, 9.67%). Among the 16 females, the majority were infected with P. vivax (n = 15, 93.75%), while only one individual (6.25%) was infected with P. falciparum .
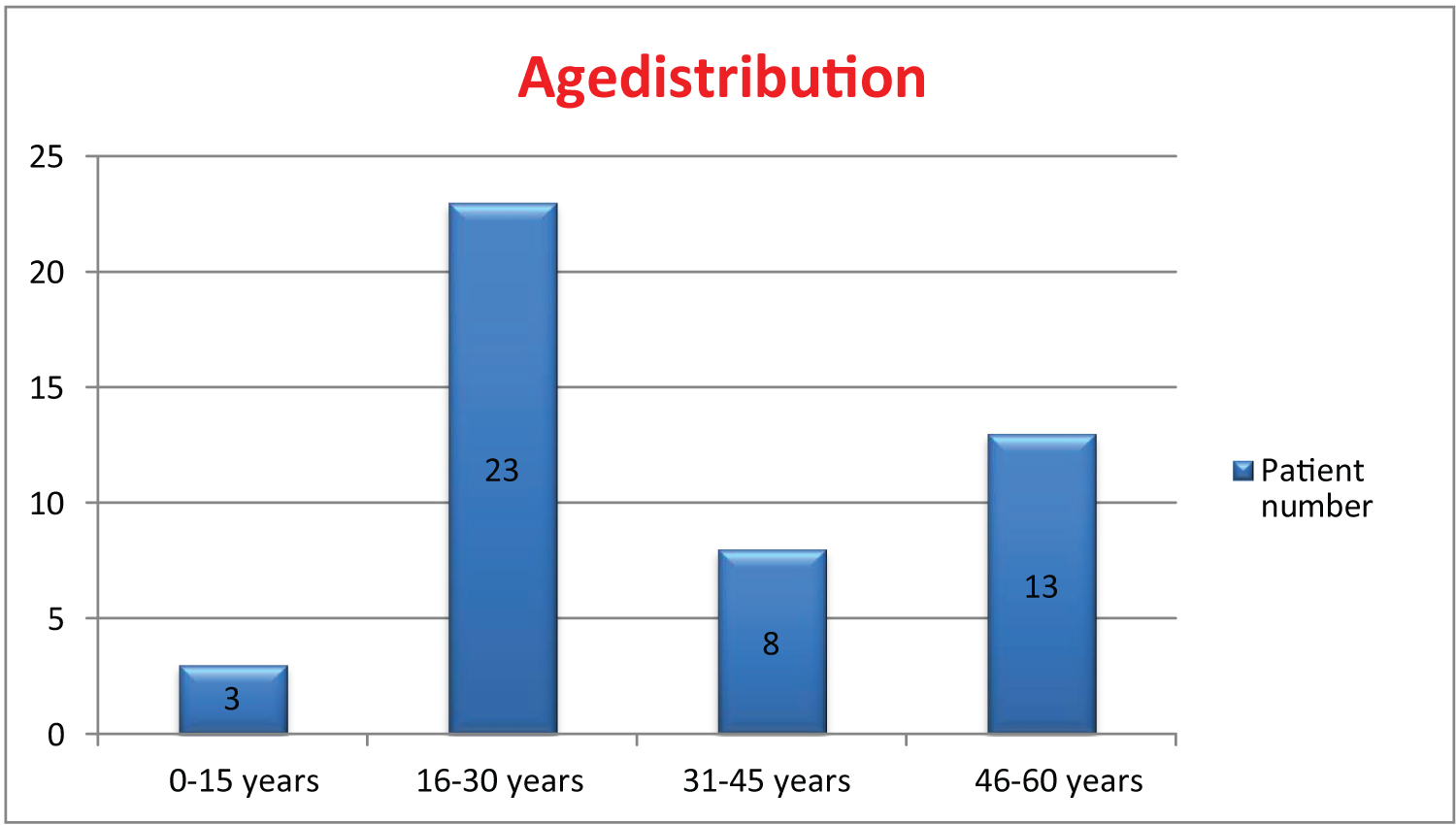 Figure 3: Age distribution of the present study.
View Figure 3
Figure 3: Age distribution of the present study.
View Figure 3
Symptoms were examined in 14 of 47 indoor patients. Symptoms included fever, chills, nausea, vomiting, and malaise. The most prevalent symptoms were fever and chills, followed by vomiting. Splenomegaly was found in one indoor patient (Figure 4).
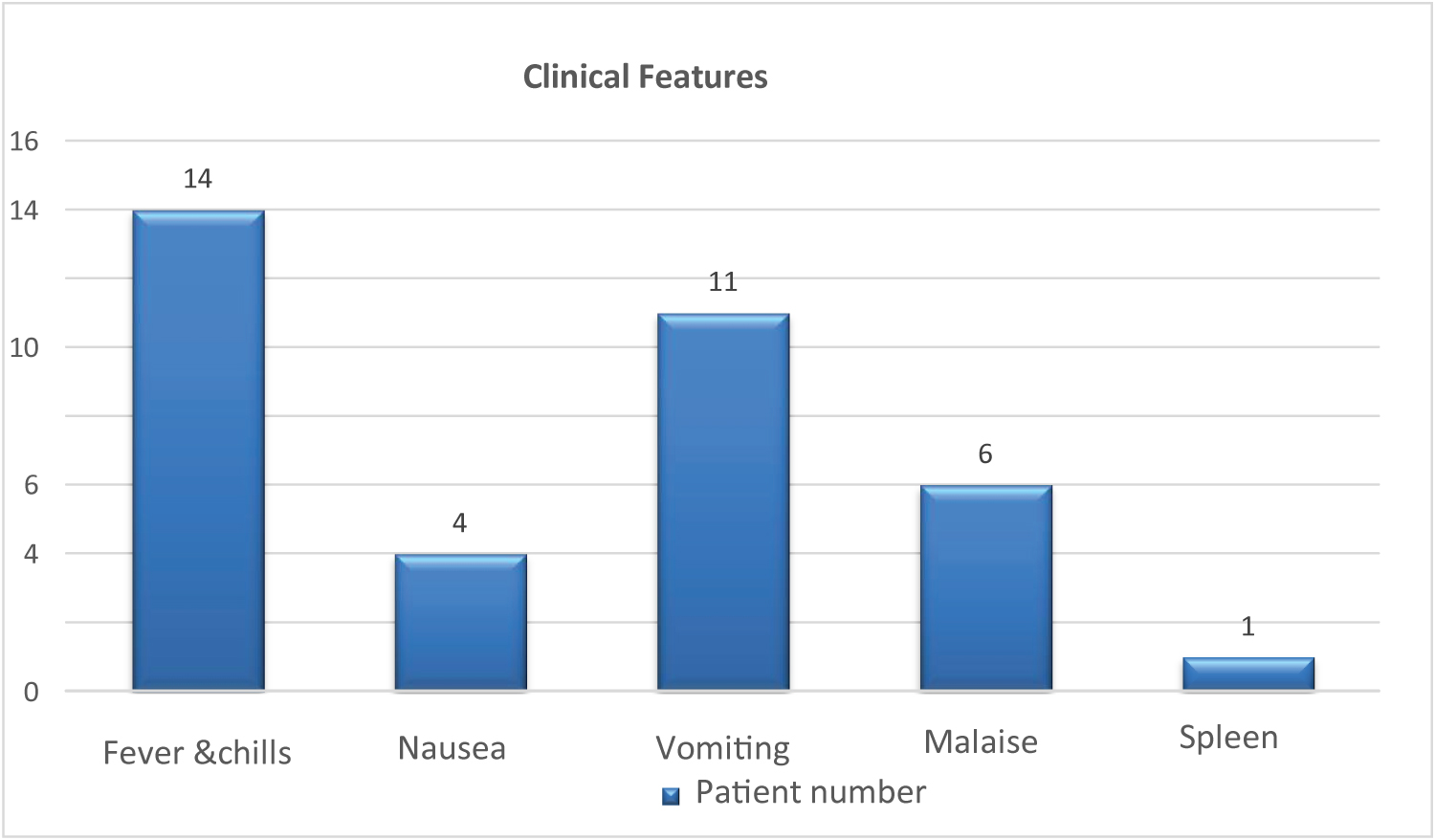 Figure 4: Symptoms of the study participants of the present study.
View Figure 4
Figure 4: Symptoms of the study participants of the present study.
View Figure 4
Anemia affected 14 individuals (29.78%), with an equal distribution between mild and moderate anemia. This investigation found no cases of severe anemia. In the case of anemia, females outnumbered males by nine (Table 1).
Table 1: Number of males and females with mild, moderate, and severe anemia. View Table 1
RBC count, HCT, RDW, TLC, and PC were significantly associated (p < 0.05). Most patients (65.95%) had normal TLC, while the majority (76.69%) had thrombocytopenia (Table 2).
Table 2: Frequency distribution of RBC count, RBC indices, RDW, TLC, and PC in the present study. View Table 2
Most individuals had a normocytic normochromic morphology (Table 3).
Table 3: RBC morphology on peripheral blood smears in the study participants. View Table 3
In the LFT analysis, serum total bilirubin was elevated in 78.37% of the patients, but AST, ALT, ALP, and serum protein levels were generally normal (Table 4).
Table 4: Analysis of biochemical parameters in the study participants. View Table 4
HB, RBC count, HCT, MCV, TLC, and PC were not significantly associated with parasitemia grade (p > 0.05, Table 5).
Table 5: Correlation of hematological parameters with grading of parasitemia. View Table 5
vivax malaria was more prevalent than P. falciparum malaria (91.48% vs. 8.51%, respectively). No cases involved other species. Similar to the current investigation, Akhter N, et al. [8], Ullah I, et al. [9] from Pakistan, and Shah P, et al. [10] from Gujarat all identified P. vivax as the primary species causing malaria, accounting for 84%, 56.6%, and 77%, respectively. In contrast, P. falciparum was the most common species reported by Sakzabre D, et al. [11] from Ghana (87.3%) and Karlkekar SR, et al. [12] from Maharashtra. The WHO reports that 53% of the P. vivax burden is in Southeast Asia, with India accounting for 47%. Malaria caused by P. vivax and P. falciparum is approximately 51:49 [13,14].
This study found that more males were infected (65.95% vs . 34.04%), which is consistent with the findings of Akhter N, et al. [8] (64%), Ullah, et al. [9] (52.9%), Shah P, et al. [10] (65%), and Awok N and Arota A [15] (68%). Males may engage in more outside activities, which could explain the relative prevalence of men. In a study conducted by Sakzabre D, et al. [11] in Ghana, they discovered that females were more affected (69.07%), which contradicts the current data. The gender-based variations in the current study's findings could be attributed to variables in size, population density, climate, and geographic location, as well as disparities in the health counseling practices of men and women. Overall, men are more likely to take medication than women. When a woman feels ill, she visits a doctor.
The majority of the patients were between 16 and 30 years of age. Sakzabre D, et al. [11] found similar results with the majority of patients aged 18-44 years.
Fourteen patients (29.78%) with anemia were classified as mild (n = 7, 14.89%) or moderate (n = 7, 14.89%). The difference in Hb levels was statistically significant (P > 0.0001).
The majority of anemic patients (n = 13, 92.8%) had P. vivax , and the majority of these patients (n = 9, 64.2%) were female. P. falciparum was primarily seen in male patients (n = 2). These results disagreed with those of a study by Shah P, et al. [10] that indicated 53.1% of cases had anemia. The fact that the majority of research participants were male may be the reason why this study found fewer cases of anemia. Although the study's highest number of P. vivax species in anemia was comparable to that of Shah P, et al. [10] ( P. vivax 76.9%). Seasonal or regional variances can occur.
The majority of patients (n = 34, 72.34%) had normocytic normochromic RBC shapes, regardless of the species. All P. falciparum malaria patients showed normocytic normochromic RBC, whereas 63.8% of P. Vivax -positive individuals had similar morphology, followed by normocytic and hypochromic RBCs (23.4%). The macrocytic RBC morphology was the least common (4.3%). These findings were consistent with those of Shah P, et al. [10], who reported normocytic normochromic RBCs in 46.6% of cases, with 21.2% of patients having microcytic hypochromic RBCs. In a rural investigation, the inclusion of previously iron-deficient patients may have revealed the occurrence of microcytic hypochromic anemia. Malaria usually causes normocytic normochromic anemia. Severe hemolysis can reveal macrocytic RBCs.
In contrast to the findings of Antwi Bafour S, et al. [16], who concluded that TLC and MCH had a significant correlation with the degree of parasitemia at 95% and 99% confidence levels, respectively, and that TLC and PC showed statistically significant relationships, our attempt to correlate hematological parameters with parasitemia grades was found to be statistically insignificant (p > 0.05, Table 5).
RBC counts were normal in the majority of patients (n = 21), with significantly decreased and increased counts in 18 and 8 patients, respectively (P > 0.0001) which is In line with the findings anemia of Shah P, et al. [10] Malaria-induced anemia can be caused by a variety of factors, including the destruction of infected red blood cells, resulting in lower RBC numbers, as well as the rapid elimination of both parasitized and non-parasitized RBC.
Malaria patients had greater mean values for MCV (87.2 ± 9.7) and MCH (28.6 ± 3.9) than control patients, although their mean MCHC (32.8 ± 2.2) was lower. There were no significant variations in MCV, MCH, and MCHC (p > 0.05). These findings are consistent with those of Kotepui M, et al. [17], who found that the RBC count was significantly lower in patients with falciparum, and the median MCV, MCH, and MCHC in patients were significantly greater than those in the non-malaria group (P > 0.001). There was no significant relationship between malaria infection status and MCV, MCH, or MCHC cut-off levels (P > 0.05).
This study found that RDW was normal in the majority of instances (n = 34, 72.34%), but mildly increased in the remaining 27.65%. RDW was significant in this study (P < 0.0001) which is non-concordant to the observation by Awok N and Arota A from Ethiopia [15]. In this investigation, no moderate or severe increase was observed. These data rule out a relationship between iron-deficient anemia and severe hemolysis.
The current study also found thrombocytopenia to be a significant hematological shift in malarial parasitemia, with more than 76.59% of the sample population showing decreased PC. This is consistent with the data of Kotepui M, et al. [17], who discovered a considerable reduction in PC. PC was normal in 23.40% of cases, indicating that patients infected with Plasmodium species and experiencing symptoms may not have thrombocytopenia. Under such circumstances, a thorough PBS examination is required, even with minimal parasitemia. Despite the prevalence of thrombocytopenia, no single incidence of bleeding symptoms was observed in the current investigation, confirming the WHO guidelines that platelet transfusion is not recommended in all patients with malaria.
In this study, the majority of patients (n = 31, 65.95%) had TLC within the reference interval, with leukopenia detected in only 16 (34.05%) cases, similar to the observation of Tobón-Castaño, et al. [18] that most cases (79%) were within the normal range, followed by leukopenia (18%). This study found that leukopenia had a significant effect (P > 0.0001). This conclusion is consistent with that of a study conducted by Chandra S and Chandra H [19], in which leukocyte counts were considerably lower in cases of acute malaria than in controls. Our investigation identified no single incidence of leukocytosis, which contradicts the findings of Khuraiya P, et al. [20], who showed a lower prevalence of leukopenia (3.84%) and leukocytosis (8.65%).
Biochemical data were available for 37 participants. Of these, 29 (78.37%) exhibited hyper bilirubinemia, which was similar to the findings of Khuraiya P, et al. [20], who reported elevated bilirubin levels in 27.88% of the cases, and the majority of the cases were P. falciparum malaria, with a large proportion of P. vivax . This study found a larger number of P. Vivax with increased blood bilirubin levels, indicating that infection with P. vivax can cause hemolysis. AST and ALT levels were increased in 15 (40.54%) instances, which were similar to those reported by Khuraiya P, et al. [20] in 31.73% and 33.65% cases, respectively. Most patients (n = 27, 72.97%) had ALP levels within the normal range, and only 27.02% had elevated levels. Sixteen individuals (43.24%) had low total serum protein levels.
Das S, et al. [21] and other writers discovered a substantial statistical correlation between AST and total bilirubin when compared to non-malaria counterparts, indicating impaired liver function [22,23]. However, this study also found LFT changes in the majority of P. vivax patients, indicating that liver functions can be affected during P. vivax infection, similar to the findings of Woodford J, et al. [24], which showed greater rates of P. Vivax infection early transaminase increase compared with the normal group.
Serum creatinine and blood urea levels were measured in 34 patients. Blood urea levels were greater than serum creatinine levels in 21 (61.7%) and four (11.7%) patients, respectively. The mean ± SD value for blood urea in P. vivax was 34.68 ± 21.35 mg/dl, similar to the work done by Khuraiya P, et al. [20] (38.72 ± 17.92 mg/dL). The serum creatinine level in P. vivax was 1.15 ± 0.47 mg/dl, similar to Das S, et al. [21] but lower than the higher value reported by Khuraiya P, et al. [20] (1.43 ± 1.05 mg/dl). This higher score could be explained by the fact that they had the majority of P. falciparum malaria cases. Similarly, Oyewole IO, et al. [25] similarly reported that most patients with P. falciparum malaria have significantly elevated serum urea and creatinine levels, indicating a change in kidney function.
The present study has limitations as study type, sample size, inclusion, and exclusion criteria. Additionally, confounding factors affecting hematological parameters like nutritional deficiencies, bacterial, viral, and helminth infections, and the genetic backgrounds of patients were not ruled out. Additional large-scale prospective studies involving more biochemical tests such as serum haptoglobin levels and lactic acid dehydrogenase, together with follow-up studies that demonstrate the effect of malaria treatment on anemia, could be beneficial and contribute to our understanding. However, anemia and thrombocytopenia can be used as supportive diagnostic criteria for malaria, in addition to clinical indices, in instances where microscopic diagnosis is not sufficient, like low parasite density PBS.
vivax species was the predominant cause of infection among the studied patients, with males being more frequently affected than females. Individuals between 13 and 30 years of age constituted the age group with the highest infection rate. Fever accompanied by chills was the leading clinical symptom, with vomiting also widely reported. The most typically observed blood abnormalities included normocytic normochromic anemia and thrombocytopenia. The research highlighted that Hb, HCT, RDW, TLC, and PC were factors with significant statistical values, while MCV, MCH, and MCHC did not show significant statistical relevance. There was no significant statistical relationship between the levels of blood parasites and hematological parameters. Hyperbilirubinemia was frequently noted as a change in liver function tests, while in renal function tests, elevated blood urea levels were more common than increased creatinine levels. Assessing hematological parameters and understanding their biochemical relationships are vital to the prompt diagnosis and treatment of malaria.
Nil.
Nil.
There are no conflicts of interest.
No : PJR/2022/42
BP and JP have collected the data. SB & AP has done study design. Data analysis was done by JP, BP & SSB. JP, BP & SSB drafted the assay & final approval was done by SB & AP.