Introduction: In this study, it was aimed to evaluate the pathological parameters in cases with bladder urothelial carcinoma diagnosed in our department, and to investigate the relationship between the cases in the literature and age, gender correlation.
Material and methods: In our Faculty of Medicine, Department of Pathology, 68 bladder biopsy cases diagnosed with urothelial carcinoma between 2018-2019 were included in the study. The pathology reports of the cases were evaluated retrospectively.
Results: According to the one-way chi-square test, extension of invasion in malignant patients was observed as pTa 51.5%, pT1 19.1% and pT2 29.4%, respectively and this proportional difference was found to be statistically significant (p = 0.004). While the pTa rate was high in patients aged below 65 (53.8%) and aged 65-74 (61.9%), pTa and pT2 rates were equal (38.8%) in patients aged > 74 years. However, in the chi-square test, the pathologic stage did not change according to age groups (p = 0.548). In our study, urothelial carcinoma cases were observed more frequently in males and the rate of pTa stage was found to be higher in male patients (53.1%). The findings in this study were found to support the literature. In our study, 51.5% of the cases were found in pTa. The rate of developing life-threatening muscle invasive disease (pT2) was 29.4%, which was similar to the rate of 20-30% in the literature.
Conclusion: The high rate of detection of our cases in the noninvasive category showed parallelism with the literature findings and was considered very positive in terms of prognosis.
As a result, accurate and early diagnosis of this tumor is very important.
Before reaching the advanced stage, patients are required to be diagnosed and followed up properly in order to provide early curative treatment.
Bladder, Urothelial carcinoma, Pathological stage
Urothelial carcinoma (UC) of the urinary tract is the fourth most common type of malignancy in the world [1,2]. The bladder is the most common pathological site for UC, it is followed by the renal pelvis, the upper urinary tract, and the lower urinary tract urethra [3].
Tobacco smoking is responsible for 50% of all urothelial carcinomas, and is at the top of the risk factors. Other risk factors include genetic predisposition, pelvic radiation and occupational exposure to carcinogens (including chlorinated hydrocarbons, aromatic amines, and polycyclic aromatic hydrocarbons) [4].
Urethelial carcinoma of the bladder is classified as non-muscle invasive disease (Ta, T1 and Tis), muscle invasive disease (T2), metastatic disease. Additionally each clinical situation differs in prognosis, treatment strategy and management. pTa is noninvasive urothelial carcinoma and is the group without lamina propria invasion. There is microinvasion/invasion of the lamina propria in pT1. Invasive foci can be single or multiple foci. However, there is no muscle invasion. pT2 is the group with muscularis propria (MP) invasion [3].
Histologically, there are smooth muscle regions (muscularis mucosa) in the lamina propria.
When there is invasion of the lamina propria, these smooth muscles may appear hypertrophied and thus the differential diagnosis of the muscularis propria and muscularis mucosa may be difficult. It is important to identify pT1 and pT2 in the pathology routine.
70% of UC’s are non-muscle invasive, and local treatments can be useful in these. However, between 15% and 20% of nonmuscle invasive patients will progress to muscle invasive UC. At the time of diagnosis, 25% to 30% of patients present as muscle invasive [5].
The majority of bladder cancers exist as non-muscle invasive low-grade papillary carcinomas characterized by a good prognosis. Unfortunately, muscle-invasive bladder carcinoma shows a poor prognosis [2]. High intravesical recurrence rates and risk of disease progression in cases with non-muscle-invasive UC require follow-up at regular periods (every 3-6 months for the next few years).
Generally, traditional treatment options for muscle-invasive and metastatic disease include radical cystectomy, chemotherapy and radiation therapy [2].
Therefore, detection of muscle invasion is important for treatment. Mortality after diagnosis and treatment is importantly related to pathological tumor stage (Ta-1, T2, T3, and T4, representing five year survival rates of 92.1%-97.8%, 74.7%-84.1%, 54.0%-56.3%) %, and 0%-12.2%, respectively) [6-8].
Early diagnosis of primary and recurrent UC is essential for a favorable clinical course. Our aim in comparing the retrospectively scanned cases in our department with the literature data was to understand the position of the patients in our hospital in terms of detection.
Before starting the study, permission was obtained from the Clinical Research Ethics Committee (Ethics Committee Number: 2020/170).
Pathology reports of 68 bladder biopsy cases diagnosed with urothelial carcinoma in Ordu University, Faculty of Medicine, Department of Pathology between 2018-2019 were retrospectively reviewed. The distribution of UC cases was evaluated in terms of age, gender, and pathological tumor stage.
Frequency analysis was performed on categorical variables. The mean ± standard deviation and minimum-maximum values were calculated for age. Two-way chi-square test was used in the analysis of the data. Calculations were made with SPSS v26 (IBM corp, Chicago, IL, USA).
Of the 68 patients included in our study, 38.2% were under 65-years-old, 30.9% were between 65-74 years-old, and 30.9% were over 74-years-old. 94.1% of the patients were male, 5.9% were female, and the mean age was 68.06 ± 11.65 years.
In our study, Transurethral Resection (TUR) material was the most common sampling method (82.8%). The rate of patients who were sampled by biopsy was 14%, and the rate of patients sampled by radical cystectomy was 3.2%. The pathologic stage was determined as pTa in approximately half of the patients (51.5%). The pathologic stage of the remaining patients was observed as pT1 in 19.1% and pT2 in 29.4% (Table 1). In the Hematoxylin & eosin stained sections in the figures, invasion of the lamina propria of urothelial carcinoma (Figure 1) and invasion of the muscularis propra (Figure 2) are observed (Figure 1 and Figure 2).
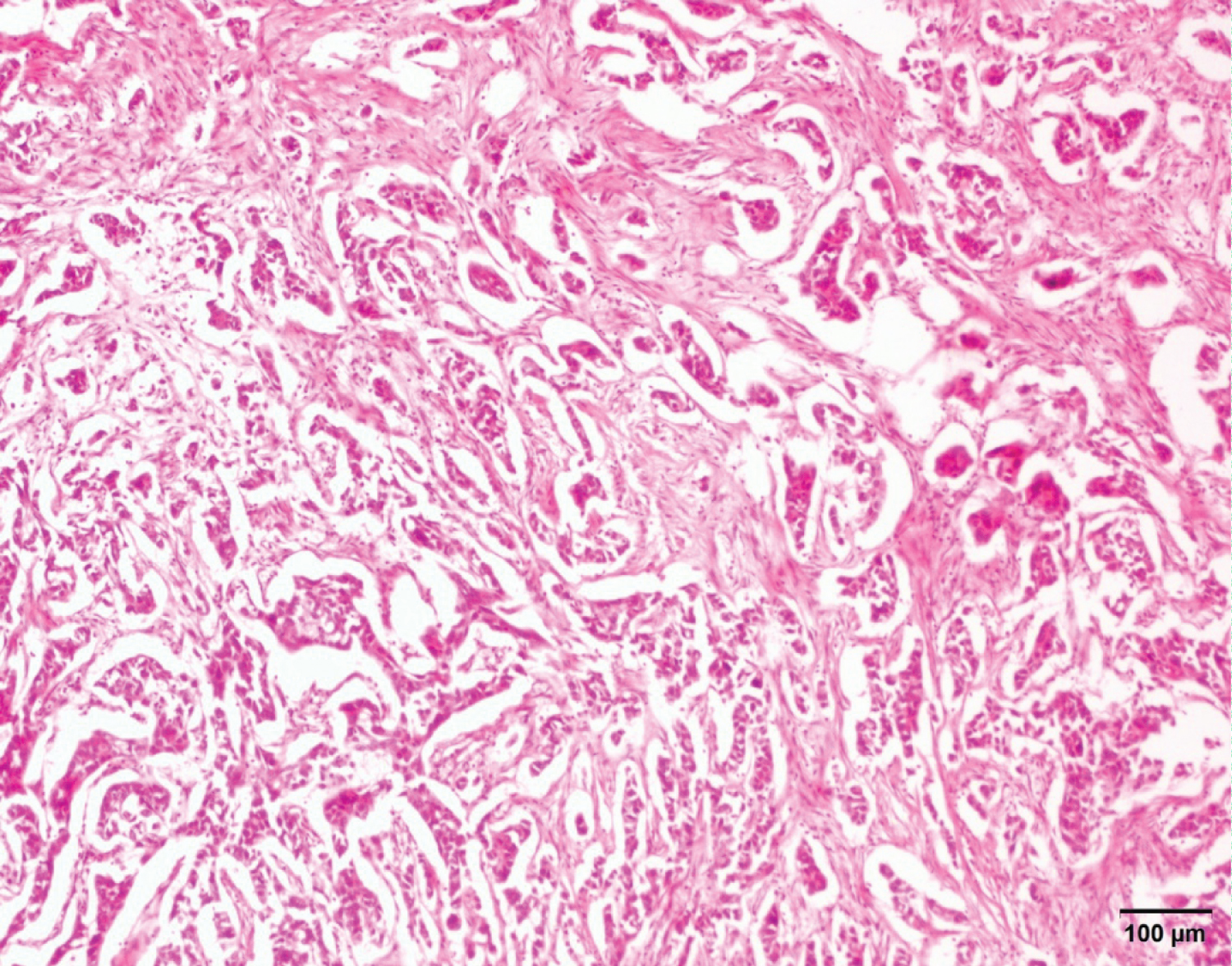 Figure 1: Urothelial carcinoma invading lamina propria (pT1), the neoplasm consists of cords, clusters, or individual tumor cells. H & EX100.
View Figure 1
Figure 1: Urothelial carcinoma invading lamina propria (pT1), the neoplasm consists of cords, clusters, or individual tumor cells. H & EX100.
View Figure 1
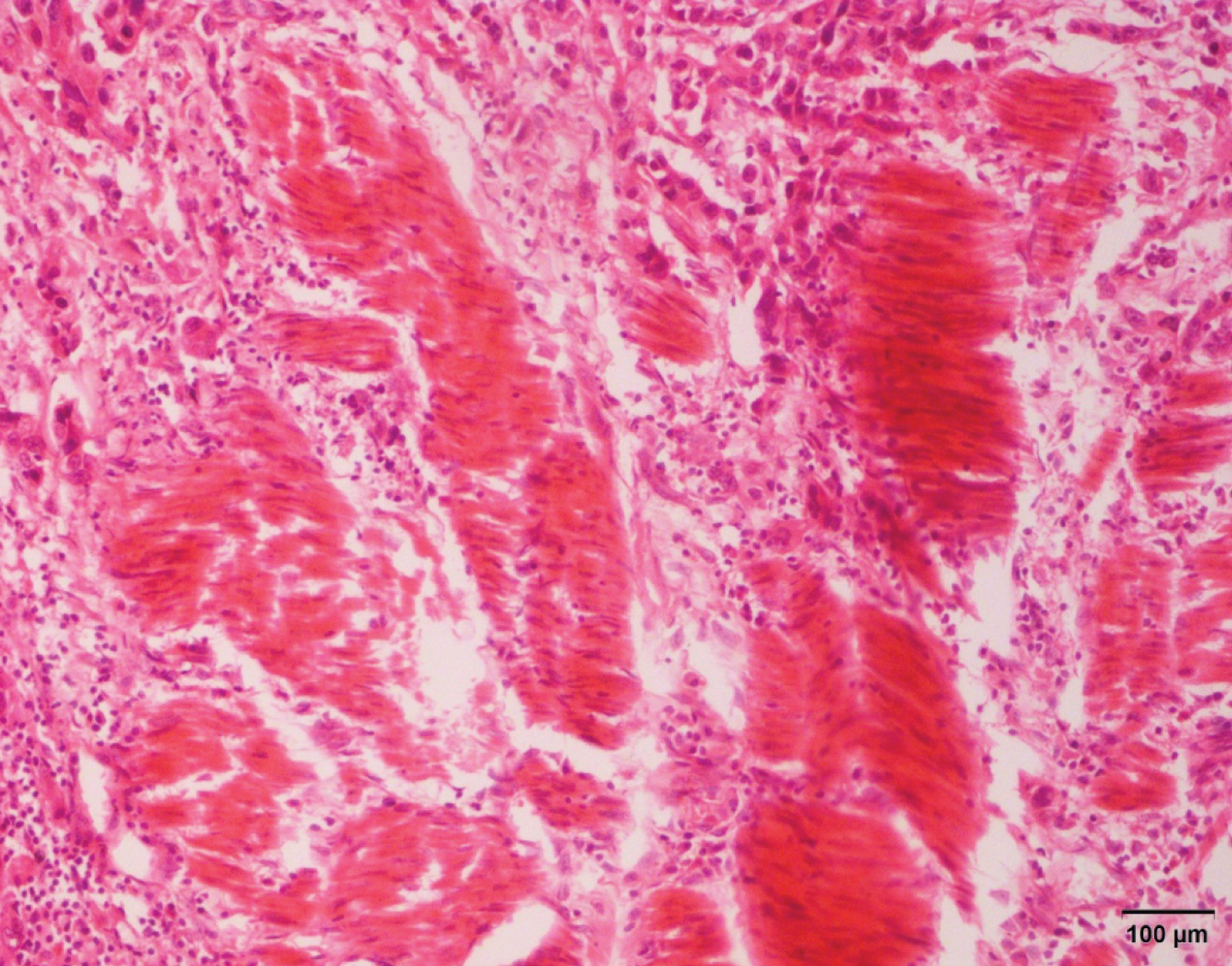 Figure 2: Urothelial carcinoma invading detrusor muscle (muscularis propria) (pT2). H & EX100.
View Figure 2
Figure 2: Urothelial carcinoma invading detrusor muscle (muscularis propria) (pT2). H & EX100.
View Figure 2
Table 1: Distribution of patients according to age, sampling method and pathologic stage status. View Table 1
The variation of the pathological stage of the patients according to gender was examined with the chi-square test (Table 2). Pathologic stage showed a statistically significant difference according to gender (p = 0.026). The rate of those with pTa stage was observed to be higher (53.1%) in male patients. In female patients, the rate of those with pT1 stage was observed to be higher (75.0%).
Table 2: Distribution of patients by pathological stage and gender. View Table 2
The change in the pathological stage of the patients according to age was examined with the chi-square test (Table 3). Pathologic stage pTa was found to be higher in patients younger than 65 (53.8%) and in patients aged 65-74 (61.9%). While pTa and pT2 ratios (38.8%) are equal in patients aged > 74 years, the ratio of those in pT1 stage is lower. However, chi-square test showed that pathologic stage did not change according to age groups (p = 0.548).
Table 3: Distribution of pathological stages of patients according to age groups. View Table 3
The change in the pathological stage of the patients according to the sampling method is given in Table 4. The pathological stage of all patients who underwent radical cystectomy was determined as pT2.
Table 4: Sampling method and distribution of patients according to pathological stage. View Table 4
More than half (57.1%) of the patients who underwent biopsy were at pT2 stage, followed by pTa with 28.6% and pT1 with 14.3%, respectively. It was determined that more than half (59.9%) of the patients who underwent TUR were in the pTa stage. In those who underwent TUR, the rates of those in pT1 (20.7) and pT2 (22.4) stages were observed very close to each other. The chi-square test showed that there was a statistically significant relationship between the sampling method and the pathological stage (p = 0.025).
In our study, it was thought that it would be useful to emphasize the importance of pathological stage detection in cases with bladder urothelial carcinoma, and to investigate the literature relations with pTa, pT1, pT2 ratios, age, gender correlation. The most important prognostic factor following surgical resection is the pathological tumor stage. In a study by Margulis, et al. 5-year survival was observed as 88-91% in superficial disease (Tis, Ta, T1), 71% in T2, 48% in T3 and < 5% in T4.) [6].
According to Von der Maase, et al. 70% of urothelial carcinomas were non-muscle invasive. At the time of diagnosis, 25% to 30% of patients were presented as muscle invasive [5].
According to our study, 48 (70.6%) of the cases were followed in the noninvasive category (pTa + pT1), and 20 (29.4%) were in the invasive category. Bladder cases with UC, retrospectively scanned in our department, showed parallelism with the literature data, and it was observed that they could generally be detected in the noninvasive category. The high detection of our cases in the noninvasive category is quite positive in terms of prognosis.
Early diagnosis of the cases is very important in terms of survival. The majority of bladder cancers are non-muscle invasive low-grade papillary carcinomas characterized by a good prognosis, while muscle invasive bladder cancer appears to be associated with a poor prognosis [2].
In a study by Lynch, et al. the incidence rates of UC were found to be two to four times higher in men than in women [9].
According to Erdem, et al. malignant bladder cases were observed more frequently in males [10]. According to our results, 94.1% of the patients with UC were male and 5.9% were female. The fact that UC is more common in men supports the literature data. The reason for this is thought to be related to smoking and exposure to occupational agents [9].
In a study in the literature, the mean age in cases with UC was 69 in men and 71 in women [9].
In our study, the mean age was found to be 68.06 ± 11.65, which was interpreted in parallel with the literature data. According to Li, et al. Important prognostic factors for recurrence were tumor grade, tumor size, tumor number, and squamous differentiation [11].
Squamous differentiation was not observed in our cases. Since our study was a retrospective study, recurrence cases could not be evaluated clearly. For this, it was thought that it would be appropriate to conduct a larger study.
It is known that mortality after diagnosis and treatment is importantly related to pathological tumor stage. The important role of the surgical pathologist is to determine the depth and extent of invasion into the subepithelial connective tissue/submucosa/lamina propria (pT1), MP (pT2) or beyond (pT3 or pT4).
Approximately 70% of UC’s of the bladder are superficially invasive or noninvasive, and these tumors are generally papillary and show varying degrees of differentiation.
On the other hand, most muscle-invasive urothelial carcinomas are non-papillary and generally exhibit high-grade cytomorphology.
Such ordinary UC’s are easily diagnosed microscopically and are not a problem for the pathologist [12].
When there is invasion of the lamina propria, these smooth muscles may appear hypertrophied and thus the differential diagnosis of the muscularis mucosa and MP may be difficult. It is important to identify pT1 and pT2 in the pathology routine.
In some cases, the distinction between pT1 and pT2 may not be possible despite re-sampling and immunohistochemical examinations, this should be stated in the pathology report.
In our study, urothelial carcinoma cases were observed more frequently in males and male patients with pTa stage (53.1%) were found to be higher. In addition, 48 (70.6%) of the cases were followed in the noninvasive category (pTa + pT1) and 20 (29.4%) were in the invasive category.
Bladder cases with UC screened retrospectively in our department showed parallelism with the literature data. It has been observed that it can generally be detected in the noninvasive category. The high detection of our cases in the noninvasive category is quite positive in terms of prognosis.
As a result, accurate and early diagnosis of this tumor is very important in terms of providing early curative treatment before it reaches an advanced stage.
MAÇ: Article writing, Material supply, Data collecting; Planning and organization; YKA: Article writing, Data analysis, Statistics.
There is no funding.
None.
Before starting the study, permission was obtained from the Clinical Research Ethics Committee (Ethics Committee Number: 2020/170).