Cutaneous myxoma is an uncommon soft tissue lesion associated with Carney Complex (CNC). In this case report, we present a 33-year-old male with a soft tissue mass that was found to be a cutaneous myxoma after excision. It was initially thought to be a cyst during a visit to a nearby emergency department, at which point, the patient was referred to our surgical clinic for further management. He hoped to have the mass removed as he was concerned about cosmesis and the possibility of neoplasia. The patient underwent excision, and pathology revealed cutaneous myxoma, which carries an association to CNC. The purpose of this report is not only to discuss an interesting case but to demonstrate that dermatologic conditions can indicate more deleterious systemic issues and to emphasize the importance of physical examination with the knowledge that not all skin lesions are typical.
Cutaneous myxoma, Carney complex, soft tissue lesion, Case report
With just over 750 cases reported, Carney Complex (CNC) is a rare multiple endocrine neoplasia (MEN) syndrome characterized by myxomatous and endocrine tumors as well as lentiginous skin and/or mucosal lesions [1]. The presence of one or more of these findings in combination raises suspicion for CNC. Cutaneous myxoma is a benign skin lesion that may be the first sign of CNC, however, its presence alone is not enough to make the diagnosis; at least one other major criterion is necessary [2]. Cases may be seen as early as the second year of life and as late as the fifth decade with a median age of 20 [1]. When discovered, they are typically asymptomatic and less than 1 cm in diameter [1]. Because cutaneous myxomas can appear similar to other common skin lesions on the surface, namely sebaceous cysts; epidermal inclusion cysts; and, lipomas, they can only be diagnosed after excision by histopathologic analysis [2]. While the myxoma itself is not fatal, some conditions comprising CNC are life threatening. This case report discusses cutaneous myxoma, its implications, and the importance of CNC surveillance.
A 33-year-old male with no significant past medical history presented to our general surgery clinic with a mass on his left shoulder that was first noticed by a friend and initially diagnosed as a cyst during a visit to the emergency room for pain at the site. On our evaluation, he denied pain, discoloration, drainage, bleeding, or change in size of the lesion since it was found 8 months prior. The patient had no family history of similar appearing masses or skin abnormalities. On physical examination, a soft, rubbery, mobile, nontender mass, measuring approximately 2.0 × 2.0 cm in dimension was appreciated on the posterolateral aspect of the patient’s left shoulder. He was deemed a candidate for surgical intervention and eventually underwent excision of the mass. At the time of operation, it appeared cystic. Pathology revealed cutaneous myxoma. Due to its association with CNC, the patient was advised to follow up with a cardiologist to rule out cardiac myxoma. Screening echocardiography performed by a local cardiologist was unremarkable. The patient currently feels well, has no complaints, and the surgical site has healed completely.
Carney Complex is a rare condition that develops over many years. The nature of the disease process as well as the variability of its components makes the diagnosis challenging. The diagnostic criteria of CNC include (1) At least two of the following major criteria: spotty skin pigmentation with typical distribution, myxoma (cutaneous and/or mucosal), breast myxomatosis, paradoxical positive response of urinary glucocorticoid excretion to dexamethasone administration during Liddle's test (PPNAD), acromegaly as a result of growth hormone producing adenoma, large cell calcifying sertoli cell tumor, thyroid carcinoma, psammomatous melanotic schwannomas, blue nevi, breast ductal adenoma, or osteochondromyxoma; or (2) One major criteria in addition to supplemental criteria of an affected first degree relative: Activating pathogenic variants of PRKACA or inactivating mutation of PRKAR1A [2]. Cutaneous manifestations, in particular, are key in contributing to the diagnosis [3]. Cutaneous myxomas are found in 30-55% of all patients with CNC; historically, those associated with CNC arise on the eyelids, genitalia, and external ear canal whereas sporadic cutaneous myxomas are more commonly found on the trunk and neck [1,4]. A 29-year-old woman was once reported to have a cutaneous myxoma on her eyelid that was not associated with CNC [5]. Based on previous studies, the presence of the myxoma on her eyelid places her at a higher risk for developing CNC compared to a similar patient with a myxoma on his or her trunk. Nevertheless, a patient with or without CNC could have a cutaneous myxoma appear on the trunk. As such, it is important to maintain an index of suspicion for CNC regardless of the location of a myxomatous lesion.
While initially described in the late 1950s, cutaneous myxomas remain poorly recognized on a gross level because they often mimic cysts and lipomas [4]. Isolated cutaneous myxomas are benign but can harbor serious medical conditions, and suspicion for these conditions should arise as soon as the diagnosis is made. We excised an oval mass measuring 2.0 × 1.5 × 1.0 cm. Upon sectioning, a unilocular cyst was identified with pale yellow gelatinous material and a tan-white, smooth inner lining. Further examination demonstrated a lobulated and fairly circumscribed mass within the mid and deep layers of the dermis (Figure 1) as well as focally in the subcutaneous tissue composed of bland spindled to stellate cells within a myxoid stroma associated with a network of arborizing thin blood vessels and few scattered mast cells and neutrophils (Figure 2). Pleomorphism or mitotic activity was not identified in our specimen. Lastly, there was evidence of cyst formation. These findings are consistent with those found in a recent study of 54 samples from patients with cutaneous myxoma [4]. Additionally, the lesions carry a risk of recurrence with a rate of 30-40%, which is largely due to incomplete excision [5-7].
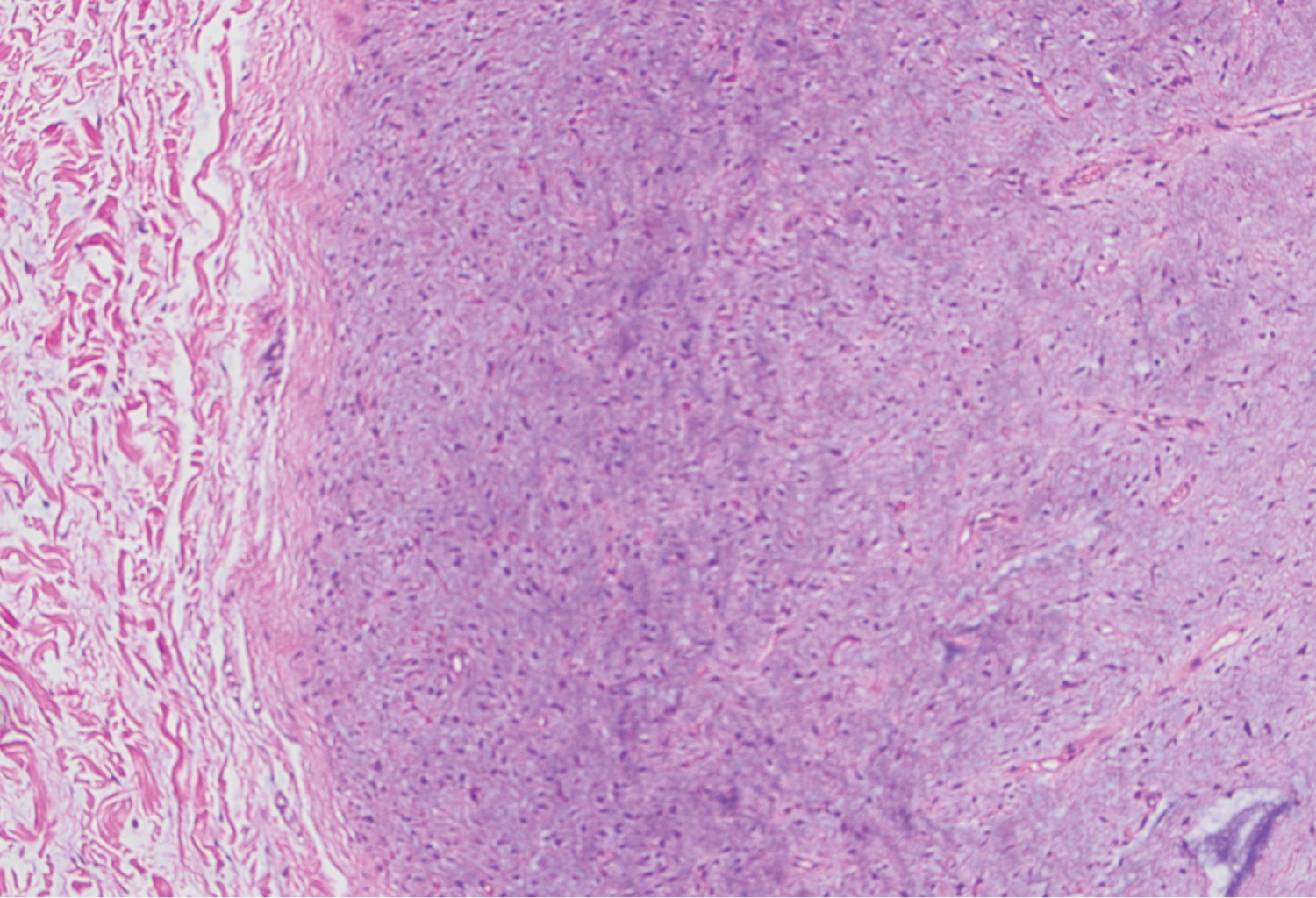 Figure 1: Cutaneous myxoma in cross-section within the dermis and subcutaneous tissues (H&E).
View Figure 1
Figure 1: Cutaneous myxoma in cross-section within the dermis and subcutaneous tissues (H&E).
View Figure 1
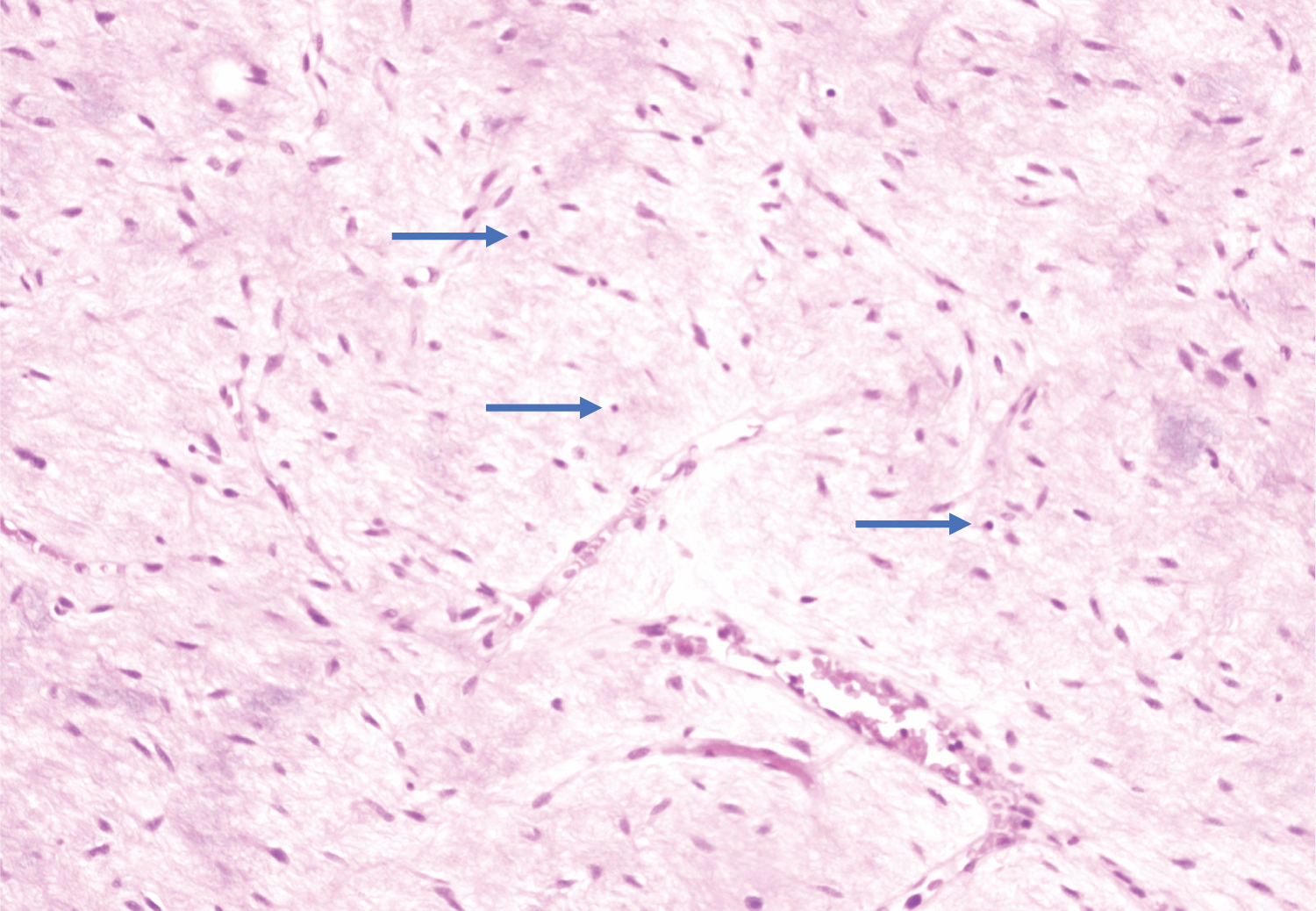 Figure 2: Cutaneous myxoma: spindle and stellate cells in a prominent myxoid stroma with interspersed neutrophils (blue arrows) (H&E).
View Figure 2
Figure 2: Cutaneous myxoma: spindle and stellate cells in a prominent myxoid stroma with interspersed neutrophils (blue arrows) (H&E).
View Figure 2
Despite the fact that Carney Complex follows an autosomal dominant inheritance pattern, approximately 25% of patients with the complex have de novo germline mutations and no family history [8]. Genetic counseling can be offered; however, counseling alone cannot confirm or exclude a diagnosis of CNC. Therefore, annual physical examination and surveillance is of utmost importance. Our patient denied any known family history of CNC when the condition was explained to him. Because he has never undergone genetic testing himself, CNC cannot be entirely ruled out. Aside from annual echocardiography, several other components can guide clinicians toward a diagnosis, including but not limited to regular skin and thyroid examinations as well as measurements of growth hormone, prolactin, and urinary free cortisol [2].
The one condition that can be lethal and accounts for mortality in greater than 50% of CNC cases is cardiac myxoma [8]. It was reported that approximately 30% of CNC patients with cutaneous myxoma developed cardiac myxoma [9]. Early detection through surveillance echocardiography on an annual basis is critical due to the severity and sudden onset of cardiac myxoma.
Cutaneous myxomas alone are benign soft tissue lesions that are diagnosed only after excision. Even though they are similar in appearance to common skin lesions, they can indicate a more serious underlying condition known as the Carney Complex. Surveillance is crucial for early detection and intervention, specifically for cardiac myxomas. The location of a soft tissue mass may or may not play a role in determining whether or not to excise the lesion; yet, it can shed light on a potential diagnosis. What is thought to be a simple soft tissue lesion should not be mistaken for a rarer tumor that can have life altering implications. Although cutaneous myxoma is uncommon, it should still be included in a differential diagnosis given its association with CNC. Patients who have been diagnosed with cutaneous myxoma should be followed closely because this finding places them at risk of developing more serious comorbid conditions.
The authors have no financial relationships or in-kind support to disclose.