Introduction: Tetanus remains a public health problem in developing countries where vaccination coverage is still low, including Madagascar. The aim of this study was to describe the epidemio-clinical aspect of tetanus in children.
Methods: This was a retrospective descriptive study over a 5-year period, including all children aged between 1 month and 15 years hospitalized for tetanus in the Pediatrics Department of University Hospital Professeur Zafisaona Gabriel (PZaGa) Mahajanga.
Results: Over a 5-year period, 30 cases were identified. The median age was 7.9 years [2-14 years]. Male predominance was noted, with a sex ratio of 6.5. Only 10 children (33.3%) had been correctly vaccinated according to Madagascar's Expanded Program on Immunization. The median incubation period was 7.1 [2-21 days]. Parents came for consultation with an average delay of 3 ± 2.5 days. Neglected plantar wounds were the most frequent portal of entry at 63.3% (n = 19), followed by circumcision at 20% (n = 6). According to the Dakar prognostic score, group I predominated, at 43.3% (n = 13). Median hospital stay was 11.8 days [1-57 days]. More than half the patients (60%, n = 18) died within 72 hours of admission. Incubation of less than 7 days was associated with death (p = 0.02).
Conclusion: Prevention is essential, and this involves increasing vaccination coverage. Practitioners need to be made aware of the need for optimal wound management and systematic verification of vaccination status.
Child, Mortality, Prognosis, Tetanus, Vaccination
Tetanus is an acute toxic infection caused by an exotoxin secreted by Clostridium tetani under anaerobic conditions, particularly in wounds with tissue necrosis or in wounds with soiled foreign bodies [1]. It is a potentially serious and fatal infectious disease once declared. Tetanus is a completely preventable disease, and has been virtually eliminated in developed countries thanks to widespread vaccination and rigorous post-exposure prophylaxis [2]. However, it remains a public health problem in developing countries. In Madagascar, despite the enormous efforts made by the Ministry of Public Health in the fight against vaccine-preventable diseases, tetanus remains one of the most deadly diseases, and poses a problem for hospital management. Its epidemiology is poorly understood in older children, where surveillance is mainly focused on maternal and neonatal tetanus [3]. Hence the need for this study, the general aim of which was to describe the epidemio-clinical character of tetanus in children in the Pediatrics department at University Hospital PZaGa Mahajanga Madagascar.
This was a retrospective descriptive study over a 5-year period from January 1er 2016 to December 31 2020. All children aged between 1 month and 15 years hospitalized in the Pediatrics Department of CHU PZaGa Mahajanga for tetanus were included. The diagnosis was based on clinical arguments associating the presence of a portal of entry associated with trismus and/or contractures. The variables studied were:
• Socio-demographic data (age, gender, parental education and occupation);
• The child's vaccination status is defined as follows:
• Completely vaccinated: When the child has received all the vaccines recommended by the Expanded Program on Immunization (EPI).
• Incompletely vaccinated: When the child has received only part of the vaccines recommended by the EPI.
• Unvaccinated: if it has not received any EPI vaccine
• Unknown: If parents or careers do not know their child's vaccination status.
• Clinical aspect (time to consultation, duration of incubation phase, clinical signs);
• Treatments received;
• Evolution (deceased or alive);
• Length of hospital stay
The data collected were entered and analyzed using Epi info 7 software. Statistical analysis was performed using the chi-square test to look for an association between independent variables and death. A value of p < 0.05 was considered significant.
Authorization was obtained from the Director of the establishment and the Head of Department to consult the medical files and the register. Patient anonymity was preserved using a computerized encoding system.
Out of a total of 5383 patients admitted, 30 cases of tetanus were recorded, representing a hospital frequency of 0.6%. A clear increase in annual frequency was noted in 2020 (Figure 1). The median age was 7.9 years [2-14 years]. The majority of children were over 5 years of age, i.e. 73.7% (n = 23). A clear predominance of males was observed, with a sex ratio of 6.5. Over half the children (60%, n = 18) had not been vaccinated. Only 7 children (23.3%) were correctly vaccinated according to the EPI (Figure 2). The plantar wound was the most common route of entry at 63.4% (n = 19), followed by the post-circumcision wound at 20% (n = 6) (Figure 3). Table 1 shows the distribution of patients according to clinical signs.
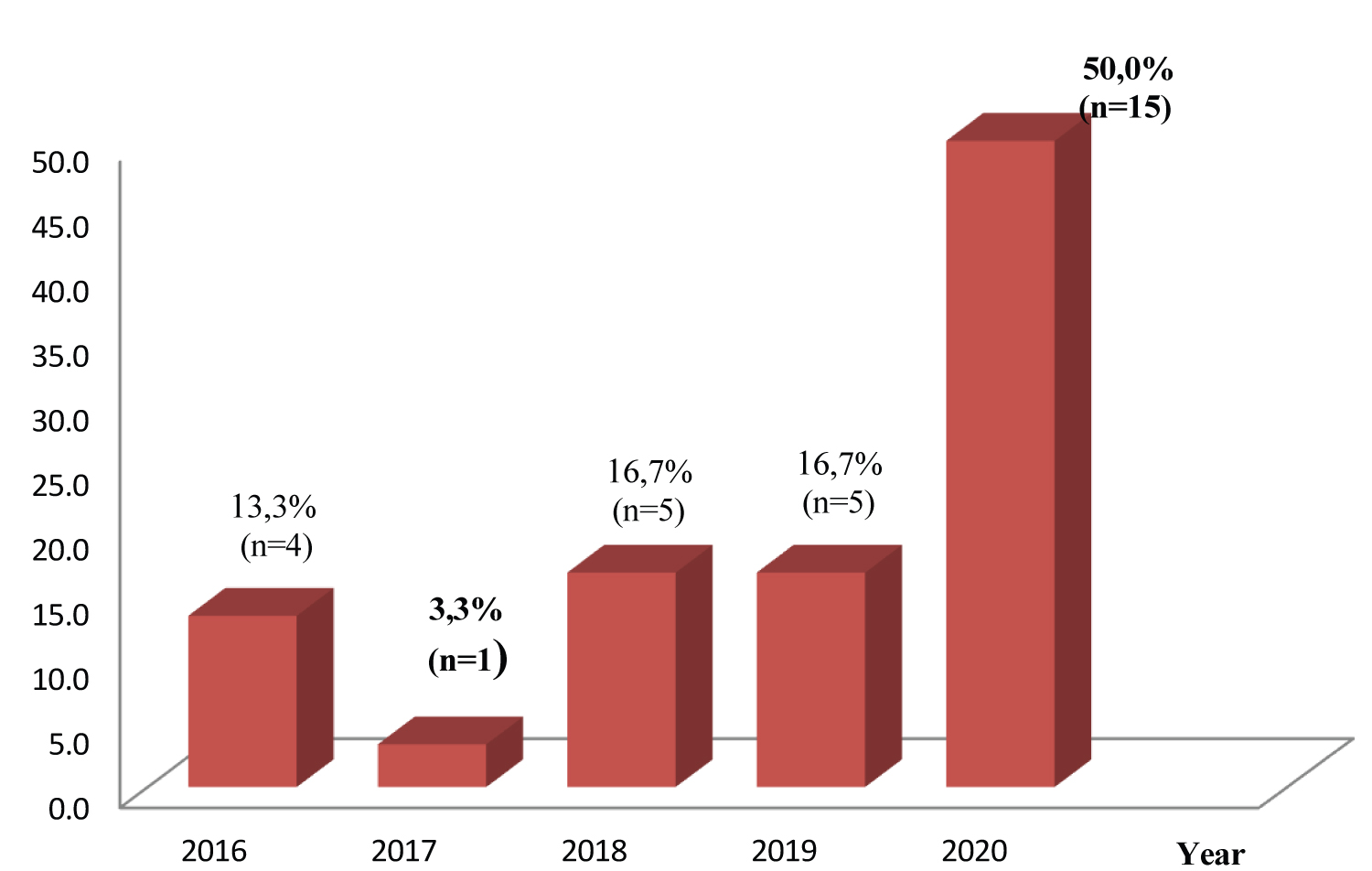 Figure 1: Annual case frequency for the period 2016-2020.
View Figure 1
Figure 1: Annual case frequency for the period 2016-2020.
View Figure 1
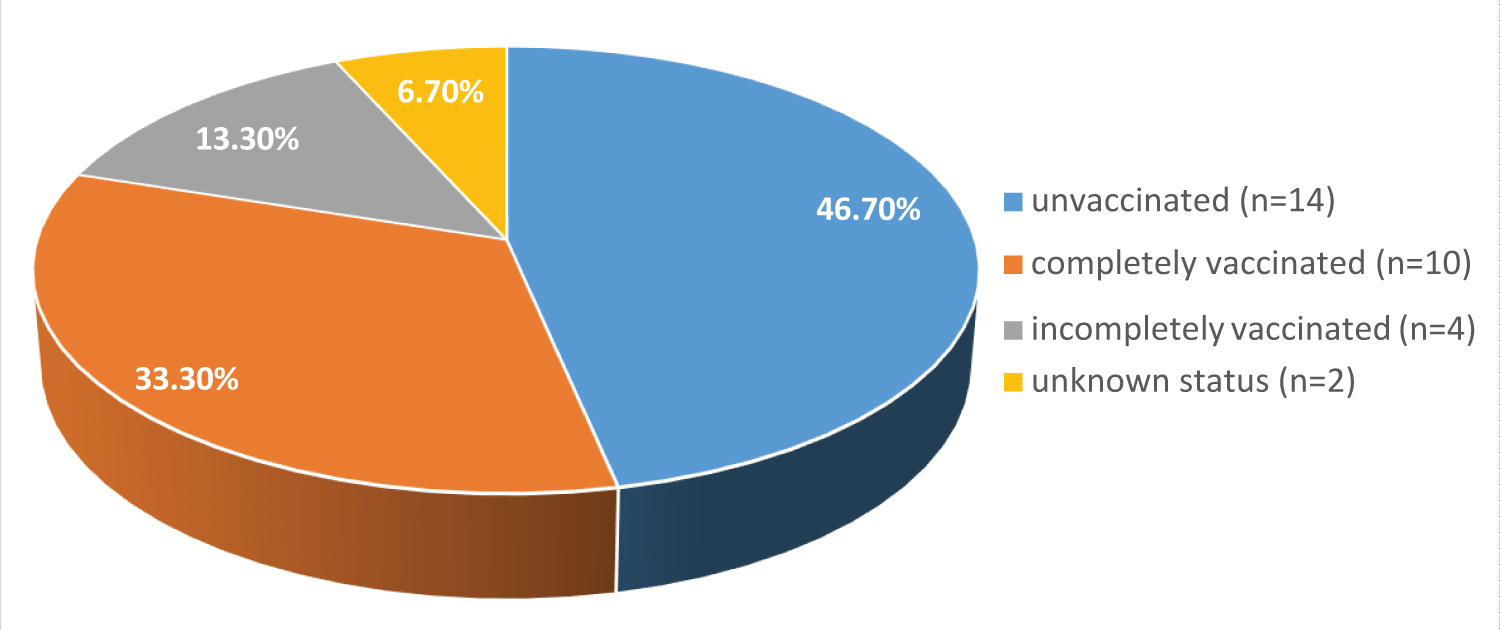 Figure 2: Distribution of patients by vaccination status according to the Expanded Programme on Immunization.
View Figure 2
Figure 2: Distribution of patients by vaccination status according to the Expanded Programme on Immunization.
View Figure 2
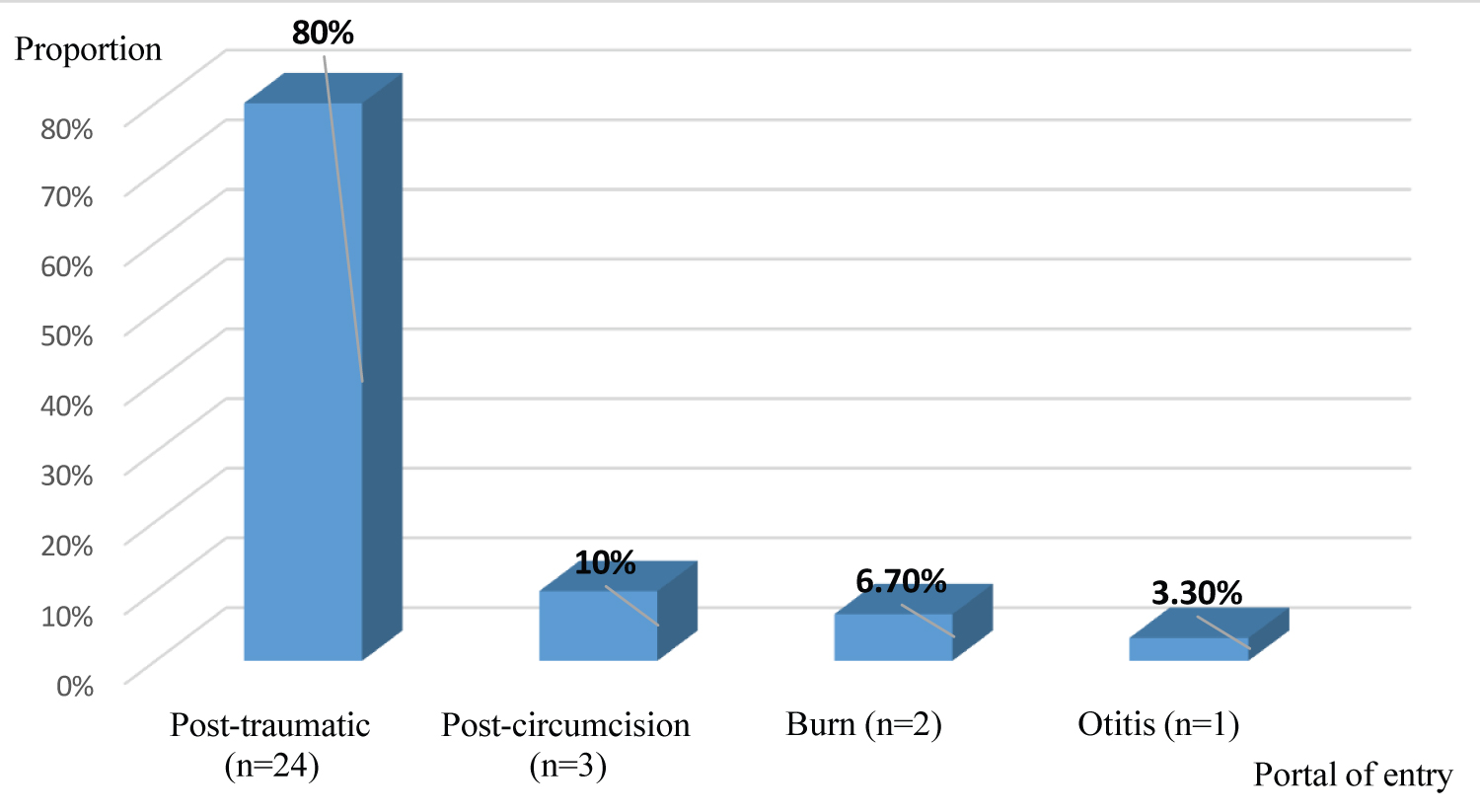 Figure 3: Distribution of patients by portal of entry.
View Figure 3
Figure 3: Distribution of patients by portal of entry.
View Figure 3
Table 1: Distribution of patients by clinical signs. View Table 1
Trismus was present in 86.7% (n = 26). Generalized contracture was observed in 66.7% (n = 20). Half the patients (50%, n = 15) had an opisthotonos attitude. According to the Dakar prognostic score, group I predominated, i.e. 43.3% (n = 13) (Figure 4). Eighteen patients died, representing a case-fatality rate of 60%. An incubation period of less than 7 days was associated with death (p = 0.02), as was a consultation period of less than 2 days (p = 0.02) (Table 2).
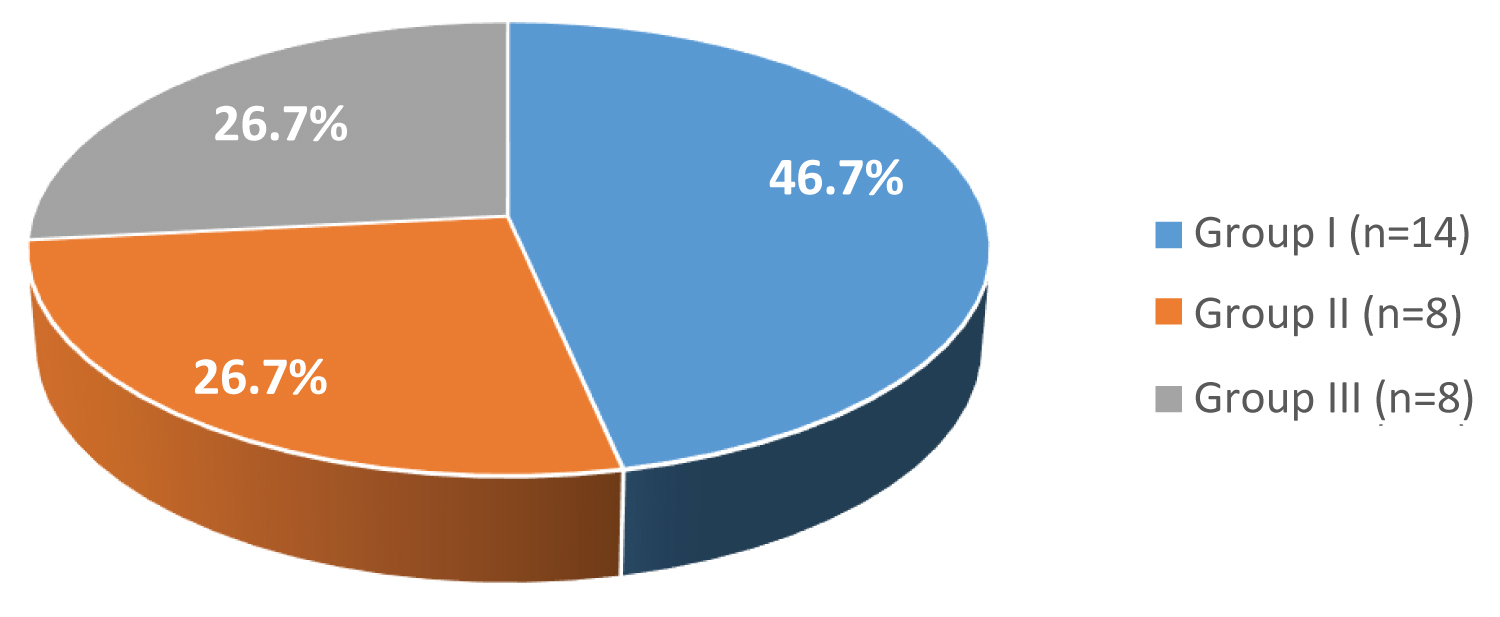 Figure 4: Distribution of patients according to DAKAR prognostic score.
View Figure 4
Figure 4: Distribution of patients according to DAKAR prognostic score.
View Figure 4
Table 2: Variables associated with deaths. View Table 2
Through this study, we were able to determine the hospital prevalence of tetanus in children hospitalized at PZaGa University Hospital. The study of these 30 cases of juvenile tetanus enabled us to obtain several elements to describe the epidemio-clinical aspect, the treatment and the evolution. We were limited by the retrospective nature of the study and the small size of the population. We were also limited by the monocentric nature of our study. However, our data may serve as a reference for future studies.
Over a 5-year period, 30 cases of tetanus were recorded, representing a hospital prevalence of 0.6%. This result is in line with that of a study carried out in Nigeria in 2015, which recorded 49 cases with a hospital prevalence of 0.6% [4]. A study in Dakar found a higher prevalence of 5.3% for juvenile tetanus [5]. In our series, however, a clear increase in frequency was noted during the year 2020. This difference could be explained by the existence of cases of tetanus that did not reach the hospital, but were treated by traditional outpatient methods. There may also be cases that are not diagnosed and reported.
The present study shows that children aged over 6 years were the most represented, i.e. 76.7% of cases, with a median age of 7.9 years [2-14 years]. This result is comparable to that of Lawson, et al. in 2020, who found a median age of 7.3 years [15 months-15 years], with a predominance in the 5-10 age group [6]. The EPI in Madagascar includes 3 doses of tetanus vaccine, providing protection against tetanus in early childhood. The level of protection and antibodies decreases beyond 4 years of age in the absence of booster doses [3]. Not all patients had received a tetanus booster. This underlines the need to include booster doses of tetanus toxoid in the EPI for all school-age children. What's more, this age group is more exposed to traumatic wounds during play, providing an entry point for Clostridium tetani .
Despite the enormous efforts made by local health authorities to improve vaccination coverage, the vaccination status of Malagasy children in general is not correct. The majority of patients were unvaccinated in 46.7% of cases. A study carried out in Mumbai in 2020 by Mondkar, et al. showed a very low vaccination coverage compared with our study, with a rate of 60% unvaccinated, 40% partially vaccinated and 0% fully vaccinated [7]. This low rate of vaccination coverage could be linked to parents' insensitivity to the benefits of vaccination, due to their low educational and socio-economic level, fear of complications or belief in non- medical practices. All this underlines the importance of promoting awareness-raising and information sessions to convince parents to adhere to vaccination. Training health-care staff in communication skills would also be fundamental to raising awareness and convincing parents.
This study showed that the post-traumatic cutaneous portal of entry was the most common in 80% of cases (n = 24), followed by the post-circumcision portal of entry (10.0%). This result is comparable to those of African authors [8,9]. These were often neglected plantar wounds. Wound management should include assessment of vaccination status and clinical determination of wound severity. In the case of high-risk wounds, tetanus vaccination is indicated for any child under 6 years of age who has not been properly vaccinated, or anyone aged 7 and over who has received three doses of primary vaccine, the last dose of which was more than 10 years ago. It is also recommended in cases where vaccination status is uncertain [3].
The case-fatality rate was 60%. This result is close to that reported by Imoudu, et al. in Nigeria in 2017, with a case-fatality rate of 61% [10]. On the other hand, this rate is much higher than that reported by studies carried out in Asia. Wang, et al. in China in 2020 in their multicenter studies of all age groups found a low mortality rate of 5.26% of cases [11]. Duggal, et al. in Pakistan in 2019 reported a mortality rate of 21.6% in their series [9]. This high case fatality rate could be explained by the late diagnosis of tetanus and the late referral to our referral center. The management of severe, generalized forms in the local context often does not allow for adequate cardiopulmonary resuscitation when using high-dose diazepam or when resorting to sedation.
A short incubation period < 7 days was statistically associated with the occurrence of death (p = 0.02). A short incubation period and a short invasion phase are associated with high tetanospasmine production. High tetanospasmine levels increase the intensity of spasms and contractures, thus worsening prognosis [12].
In addition, a consultation time < 2 days was associated with the occurrence of death (p = 0.04). A short consultation time could be associated with a short invasion phase. Thus, the rapid generalization over a short period of contractures and spasms could alert parents and motivate consultation of a health center [13].
Tetanus remains a public health problem in many developing countries, including Madagascar, despite the availability of effective anti-tetanus vaccine. Tetanus in the paediatric setting is still a topical issue, with high case-fatality rates linked to the severity of clinical presentations, delayed diagnosis and inadequate technical facilities for the appropriate management of severe forms. In low-resource countries, vaccination is still essential, and this means boosting coverage and including booster doses in the EPI. Practitioners also need to be made aware of the need for optimal management of all high-risk wounds, including systematic verification and updating of vaccination status. Equipped intensive care units also need to be set up to improve management of patients with severe tetanus.
Authors declare no conflict of interest.
I would like to thank all the authors for their collaboration.
Ranaivo NAR contributed to the design of the study and drafting of the manuscript. Rakotohasinoro CA carried out data collection and interpretation. Ranaivoson H contributed to data collection. Rahariniainasoa A contributed to the drafting of the manuscript. Andrianarimanana KD participated in the revision of successive versions and approved the final version.