Pyomyositis is defined as a bacterial infection of striated muscle. It is endemic in tropical areas of Asia and Africa, hence it is often referred to as “tropical pyomyositis” [1]. There is an increasing incidence being reported in temperate locations.
Commonly involved sites include the pelvis and lower limbs. Neck pyomyositis is a rarely involved site. In this report, we present a child who presented with pyomyositis causing abscess in the sternocleidomastoid (SCM) muscle. Written consent has been obtained from the patient’s parents to present this case.
A 12-year-old female presented to hospital with a 3 day history of headache, sore throat and right neck swelling. She had pain with neck rotation. She denied dyspnea, dysphagia, dysphonia, or cough. The GP had treated with oral amoxicillin for 2 days. She had been horse riding before becoming unwell. No exposure to sick contacts. No previous episodes of similar illness. COVID-19 test negative. She was normally fit and well. She was up to date with her immunisations.
On examination, she appeared alert but was febrile 38.7 °C. She had no stridor or increased work of breathing. She had right side torticollis, but maintained reasonable range of neck motion. There was a firm erythematous swelling over the right neck 8 × 6 cm that was tender to palpation. Oral cavity showed grade 1 tonsils without erythema or ulceration. The rest of the exam was normal. Blood tests showed elevated WBC (13.96 × 10E9/L) and CRP (81 mg/L).
She was admitted to the ward and treated empirically for right neck lymphadenitis with overlying cellulitis. She was started on antibiotic treatment with IV augmentin with some initial benefit in neck comfort. However after 48 hours, her clinical progress had plateaued and she had ongoing fevers on the ward.
The decision was made to investigate with an ultrasound of the neck (Figure 1). This showed a markedly thickened sternocleidomastoid (SCM) with irregularly shaped infiltrative areas with complex fluid. There were multiple surrounding enlarged lymph nodes in level 2 and 3. This was suspicious for suppurative pyomyositis. Given this finding, a computed tomography (CT) neck was performed (Figure 2). This confirmed a loculated rim enhancing abscess in the right SCM, measuring 38 × 23 × 20 mm with surrounding fat stranding and reactive lymphadenopathy.
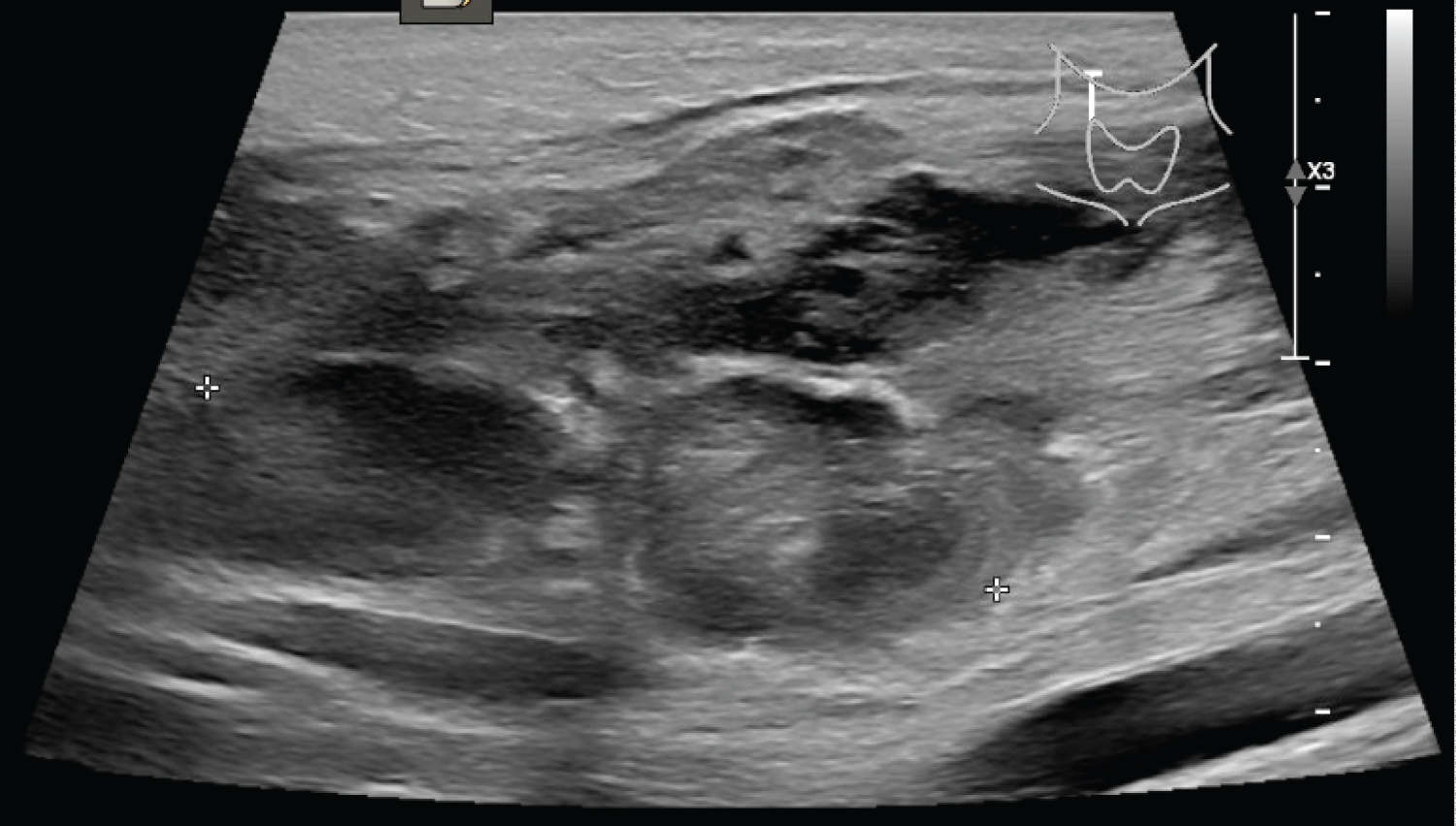 Figure 1: Ultrasound showing irregularly infiltrative areas within the thickened sternocleidomastoid.
View Figure 1
Figure 1: Ultrasound showing irregularly infiltrative areas within the thickened sternocleidomastoid.
View Figure 1
 Figure 2: CT showing loculated rim enhancing collection within the sternocleidomastoid muscle (white arrow). (A) Axial slice; (B) Coronal slice.
View Figure 2
Figure 2: CT showing loculated rim enhancing collection within the sternocleidomastoid muscle (white arrow). (A) Axial slice; (B) Coronal slice.
View Figure 2
The patient was taken to theatre for incision and drainage of right neck abscess under general anaesthesia. After dissection through platysma, a multiloculated abscess was found deep in the SCM. A sample of pus and abscess wall was taken for culture and histology. Copious washout with saline and iodine. A corrugated drain was left in the wound.
Histology showed acute inflammation infiltrating between necrotic muscle fibres.
The pus aspirate culture grew streptococcus pyogenes, which was sensitive to penicillin.
Blood cultures taken during periods of fever were negative.
On day 1 post-operation, the patient was feeling better and the drain was removed. She was discharged home to complete a 2 week course of oral augmentin. She was reviewed at 1 month follow up and reported full recovery. The surgical site had healed without residual cervical lymphadenopathy.
This case exemplifies a patient who developed pyomyositis affecting the sternocleidomastoid muscle due to Streptococcus pyogenes . Pyomyositis accounts for 1-4% of hospital admissions in tropical areas including Asia and Africa [1]. Studies from Northern India show peak incidence during months of high humidity (July to October) [1]. Cases have been reported in temperate regions including Australia, the United Kingdom and United States, but again with a propensity to areas with higher temperature [1]. To our knowledge, this is the first case reported in New Zealand which has a temperate climate.
Pyomyositis can affect patients at any age, however it is considered a disease of young adults. Paediatric patients account for a third of cases [2]. The causative organism for the majority (60%) of cases is Staphylococcus aureus [1,2]. Others include Streptococcus pyogenes (5%), and other Streptococci species [2,3].
Pathogenesis is thought to be related to bacterial seeding from transient occult bacteremia [2,3]. However skeletal muscle is inherently resistant to bacterial infection. Local muscle injury, for example from playing sports, at the time of bacterial inoculation is a factor that facilitates infection [1]. Immunocompromised patients are at higher risk including those suffering from diabetes, human immunodeficiency virus (HIV), malignancy, and autoimmune disease [4]. Other risk factors include immunosuppressant drugs such as steroids and concurrent skin infection [1]. Our patient did not comment on recent neck injury, however she did report riding a horse prior to becoming unwell.
An interesting feature in this case is the site of disease. Pyomyositis commonly affects the pelvic (41.6%) and lower limb (31.6%) muscles [2]. It may be multifocal in 20% [1]. A systematic review on paediatric cases by Vij reported on only 1/361 affecting the sternocleidomastoid [2]. This case is the second to report on sternocleidomastoid involvement.
The common presenting symptoms of pyomyositis include localised pain in a muscle group, muscle tenderness and fever [5]. A paediatric patient with an acutely tender neck mass is most likely to have reactive adenitis. Other differentials to consider include bacterial infection (cat-scratch disease, toxoplasmosis, actinomyces), systemic infection (mononucleosis, tuberculosis, HIV), congenital cyst (thyroglossal duct cyst, branchial cleft cyst, sebaceous cyst), pathology of thyroid gland or salivary glands, and other neoplasms [6].
Pyomyositis, particularly of the sternocleidomastoid, is difficult to distinguish from other pathologies based on clinical examination alone. Investigation with ultrasound is considered the first line in paediatric cases given it is non-invasive, easily obtainable and inexpensive [1]. For anatomical localisation of abscess, cross-sectional imaging with either CT or MRI is acceptable. If available, MRI has superior soft tissue delineation with affected muscle showing high signal intensity on T2 weighted imaging along with contrast enhancement [7].
The mainstay of treatment of systemic antibiotics and drainage of abscess. Antibiotics should be directed against gram positive organisms, especially Staphylococcus aureus . Antibiotics alone may be successful in 40% of cases but a prolonged course of 4 weeks is often required [2]. The majority (60%) have antibiotics combined with surgical drainage of abscess [2]. Positive microbial culture of pus aspirates can direct further antibiotic therapy. Failure of treatment can lead to complications including osteomyelitis, septicemia and septic arthritis [1,2].
We present a case of Streptococcus pyogenes causing pyomyositis in a paediatric patient. This led to an abscess in the sternocleidomastoid which is a rarely affected site. Other unusual features include the disease affecting a healthy young patient living in a temperate climate without preceding trauma. Failure to progress with parenteral antibiotics prompted further investigation with radiological imaging. Surgical drainage of the SCM abscess was performed with clinical improvement.
No conflicts of interest to disclose. No sources of funding.
We accept full responsibility for the conduct of the study, had access to the data and controlled the decision to publish.