To put an end to preventable newborn deaths, quality care must be provided throughout the continuum of care, i.e. during labor, at the time of delivery, during the first week of life and when newborns are ill or low birth weight. The aim of this study was to evaluate the neonatal unit in the context of newborn care according to WHO standards.
Methods: We carried out a cross-sectional, observational, descriptive study analyzing the premises, staff and equipment of the neonatology unit. The structure was evaluated according to WHO standards.
Results: For all criteria combined, we obtained an overall score of 57%, including 62% for infrastructure, 50% for equipment and supplies and 66% for the technical quality of care offered to newborns. 14.3% pediatricians, 9.52% general practitioners, 33.33% nurses and 19.05% housekeepers staffed the neonatal unit. There was no equipment needed to care for newborns with pathologies of any severity. With regard to the technical quality of care, we gave the highest score to routine care (100%).
Conclusion: Assessment of the neonatal unit revealed shortcomings in terms of premises, staff and equipment, making it difficult to care for newborns. This lack of equipment and staff has an impact on the quality of care.
Assessment, Care, Newborns
In 2019, 2.4 million children worldwide died in their first month of life. There are approximately 6,700 newborn deaths per day, which represents 47% of all deaths of children under 5-years-old, an increase compared to 1990 when it was 40% [1].
The proportion of neonatal deaths among children under 5 years of age is still relatively low in sub-Saharan Africa (36%), which remains the region in the world with the highest mortality rate among those under 5 years of age [1]. In Guinea, according to the Multiple Indicator Cluster Surveys (MICS) 2018, the neonatal mortality rate is 32% live births and infant-juvenile mortality is 111% [2]. Children who die within the first 28 days of life have conditions and illnesses associated with lack of quality care at birth or lack of skilled care or treatment immediately after birth and in the first days of life [1]. In 2012, an integrated tool to support quality improvement in maternal, newborn and child health services in hospitals was developed to help assess the quality of care provided to mothers, newborns and children in hospitals, reference centers and hospitals. The tool is based on standards from the WHO Pediatric Hospital Care Pocketbook, the Safer Motherhood Program Assessment Tool and other relevant WHO materials [3]. The WHO Regional Office for Africa, in collaboration with the Department of Maternal, Child and Adolescent Health at WHO Headquarters in Geneva, strengthened the capacity in October 2014 of countries Francophones including Guinea to improve the quality of care for newborns and children in reference health centers or hospitals. It is in the desire to understand the problems of newborn care at INSE and to have precise and objective information that we undertook this study, the general objective of which was to evaluate the unit of neonatology as part of the care of the newborn according to WHO standards.
The study was carried out at the neonatology unit of INSE, a reference structure (level 3) of the Guinean health pyramid. The neonatology department with a capacity to accommodate 77 newborns is the only neonatology center in Guinea. Its vocation is to provide training and applied action research in the field of neonatology, to respond to emergency situations of newborn pathologies and to offer nutritional advice to mothers for the feeding and nursing of their child. This system, set up by a multidisciplinary team, offers 24-hour reception for all newborns living in the city of Conakry and throughout Guinea.
This is a cross-sectional, observational study with a descriptive aim which took place from November 2 to 17, 2022. The survey was carried out mainly by a doctor specializing in pediatrics, assisted by the Institute's statistics officer child nutrition and health. The annual hospital statistics report (year 2022), hospitalization records, neonatal emergency department registers as well as interviews with staff on technical and practical knowledge on the care of newborns, information on infrastructure, human resources (numbers, function), availability of medicines, equipment and materials and products were used. Three (3) pediatricians, two (2) general practitioners, and three (3) nurses were interviewed and monitored in their practices. We assessed the neonatal unit according to standards based on the Standards for Improving the Quality of Maternal and Neonatal Care in Health Facilities and the Standards for Improving the Quality of Care for Children and young adolescents in health care settings [4,5]. For each piece of information collected, scores from 5 to 1 were assigned; 5:100% indicates good practice respecting standards of care; 4:80% showing little need for improvement to meet standards of care; 3:60% means some need for improvement to achieve standards of care; 2:40% indicating considerable need for improvement to meet standards of care; 1:20% showing that services are not provided, that care is totally inadequate or that practices present a fatal risk. To estimate the final quality score using the same tools, an average was calculated for each criterion. To estimate the final score, an average was calculated for each criterion. For the final score we added the intermediate (average) scores then divided by the number of criteria. Means with decimal places were rounded up or down. Data were entered and analyzed using Epi info version 6 software.
The results cover the technical quality of care offered to newborns, infrastructure, equipment and supplies and human resources. The overall score obtained for all performance criteria was 57%.
As shown in Table 1, the performance criteria with the highest scores are: availability of electricity and running water, availability of transportation, and availability of toilets. The lowest scores were attributed to the availability of suggestion boxes, the existence of a policy of free provision of medicines to newborns, and the availability of safety boxes in all treatment rooms.
Table 1: Status report of the neonatal unit infrastructure. View Table 1
The staff of the neonatology department consisted of: 2 general practitioners acting as pediatricians, 3 pediatricians, 7 nurses including the general supervisor and 4 non-professional health workers. During the day, the service operates with 15.4 beds per doctor and 11 beds per nurse, while at night; the service operates with 38.5 beds per general practitioner and 15.4 beds per nurse (Table 2).
Table 2: Human resource situation during main working hours and after working hours at the neonatal unit. View Table 2
Basic equipment and supplies essential for routine care and detection of complications are insufficient. However, the department is equipped with a significant quantity of incubators and phototherapy lamps (12 and 10 respectively). On the other hand, equipment such as: Stethoscope, Timer or stopwatch, Glucometers, connection sheet, Continuous positive pressure ventilation systems, Children's beds with heated mattresses and thermometer are not available. The average score given to equipment availability is 50%.
The performance criteria with the highest scores are: Routine neonatal care (100%), supportive care and monitoring (80%), medical records (80%). Poor scores were attributed to the availability of essential medicines (40%), the neonatal health service (60%) and the care of sick newborns (60%). The overall score for all performance criteria is 66%.
In 2022, 2,885 newborns were admitted to the neonatology unit, including 1,068 cases of death, or 37%. The main admission diagnoses in order of decreasing frequency of pathologies are: perinatal asphyxia (38.51%), prematurity (22.77%), intrauterine growth retardation (15.94%), sepsis (15.94%), jaundice (4.94%) and congenital malformation (1.94%). Newborns affected by prematurity are the most likely to die (44.14%) followed by perinatal asphyxia (37.71%) and IUGR (33.48%).
During this study, we made a general assessment based on standards from the WHO Pocket Book on Pediatric Hospital Care and the WHO Guidelines on Integrated Management of Pregnancy and Childbirth [5]. It made it possible to determine the quality of care provided to newborns at the INSE neonatal unit. The main limitation of this study is that in Guinea, there are no regulatory texts (standards) which govern the organization of perinatal care. However, the standards of care for sick and small newborns in health establishments define and standardize hospital care for these newborns and give them a central place based on essential newborn care and ensuring their consistency with the WHO quality of care framework [6,7]. This study aimed to help the management of INSE and health personnel directly involved in the process of improving the quality of care given to newborns. This is ultimately to help identify gaps and strengths in key areas of neonatal care that require improvement.
The overall score for infrastructure, equipment and supplies and technical quality of care offered to newborns was 57%, indicating some need for improvement to reach WHO standards of care. According to Bohren, et al. high-quality care requires appropriate use of available infrastructure, personnel and products to ensure effective case management [8].
Built in 1988 with a capacity of 12 beds, the infrastructure and equipment of the neonatology unit no longer meet standards. The service currently has 77 beds distributed in 11 hospitalization rooms. This result in a load compared to the capacity of the unit. Electricity was available in all rooms thanks to Guinea's electrification networks, solar panels and generators. Running water (without microbiological quality control) was also available to meet the needs (personal hygiene, medical procedures, cleaning and drinking), but without water supply in all rooms (Table 1). Essential to the proper functioning of hospitals, water is subject to numerous uses requiring specific qualities. Rigorous management is essential because, in the event of contamination, water can be the cause of serious infections, particularly among the most vulnerable patients [9]. According to WHO standards, we observed that the neonatology department does not have the necessary equipment to properly care for newborns presenting with serious or minor pathologies (Table 3). Being the only public neonatal hospitalization unit in Guinea, it takes care of all referred newborns, regardless of the severity of the clinical condition. This shortage of equipment can affect the quality of care for hospitalized newborns and lead to high neonatal mortality as evidenced by the statistics for 2022 (Figure 1). To prevent a massive flow of sick newborns from arriving at the INSE neonatology unit, it would be interesting to train and strengthen the capacity of providers and to provide care premises for newborns. so that a minimum of emergency care is possible in peripheral maternity wards. In Senegal, for example, a space called a “newborn corner” is set up in most health centers to improve care for newborns [10]. A study carried out in Tanzania showed that there was a significant relationship between a delay in initiating mask ventilation and admission to neonatal hospitalization and/or death. The risk of death and morbidity increased by 16% for every 30 seconds delay in initiation of mask ventilation up to six minutes, and more than two-thirds of deaths occurred when ventilation was administered beyond four minutes [11]. In this study, the lack of a hygiene kit, a container for sharps and soiled objects, a device for sorting, collecting, eliminating waste and washing hands were highlighted by the healthcare staff, of whom approximately more than half were dissatisfied with the medical products available to them. This is a weakness of the system because poor waste management can put healthcare workers, employees dealing with medical waste, patients and their families, and the entire population at risk [12]. In our context, it is possible to significantly reduce the risks linked to hazardous medical waste through simple and appropriate measures (e.g. hand washing and disinfection of equipment).
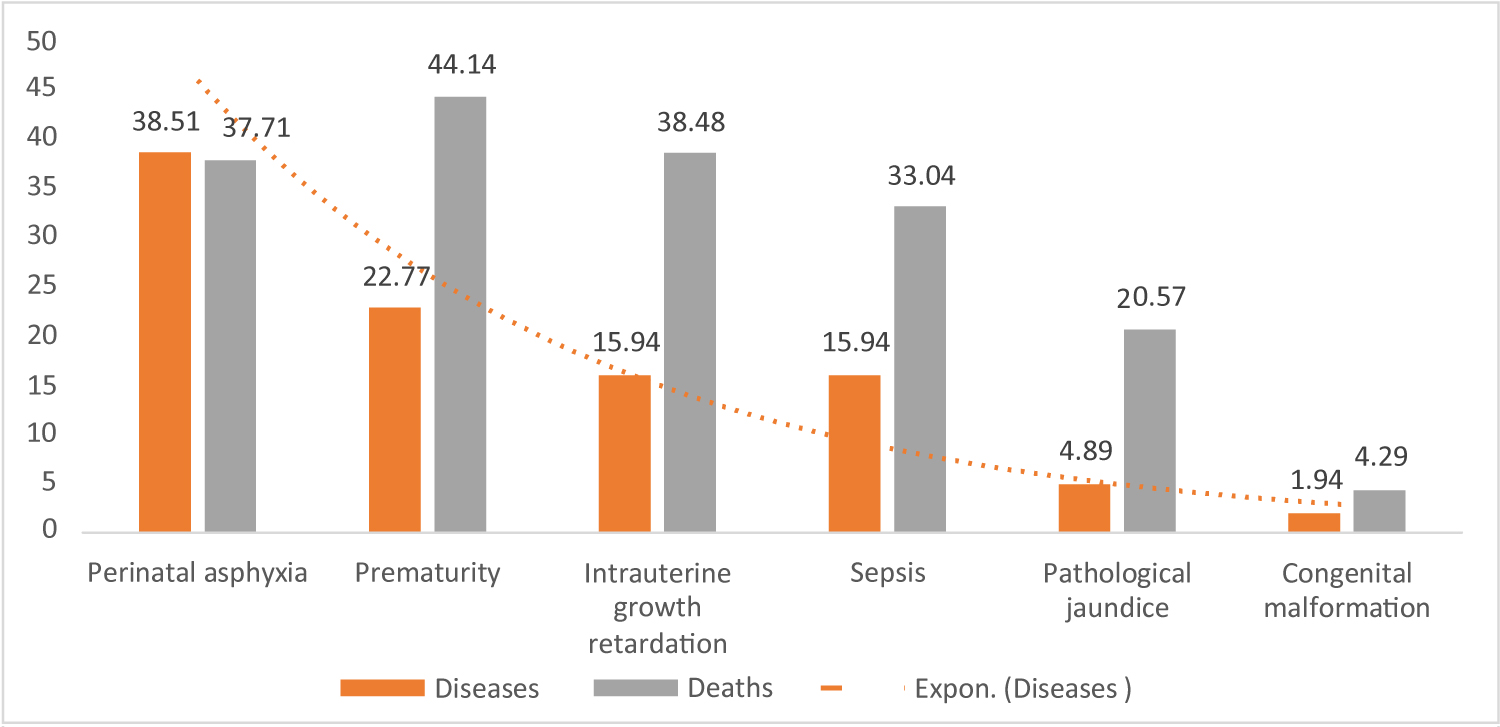 Figure 1: Hospital statistics (year 2022).
View Figure 1
Figure 1: Hospital statistics (year 2022).
View Figure 1
Table 3: List of equipment and their availability in the INSE neonatology department. View Table 3
The evaluation of the theoretical and practical knowledge of staff on the management of the main illnesses of the newborn showed an average score of 66% for all performance criteria (Table 4). According to our observations, almost all of the newborns hospitalized in the neonatology unit benefited from routine care immediately after their admission. Monitoring newborns during routine postnatal care helps identify complications requiring treatment. Each admitted newborn was entered in the reception room register. Parameters such as: weight, temperature, head circumference were checked every day by the nursing staff. Knowing the weight of a newborn at birth or upon arrival at the health facility helps improve care decision-making [7]. Weighing also makes it easier to calculate doses of medications and fluids administered intravenously. All newborns referred by primary health structures or by municipal health centers are subject to triage intended to quickly assess emergency signs or trauma and determine if resuscitation was necessary. Those needing supplemental oxygen therapy receive the treatment with modest equipment, namely nasal prongs, flow meters, oxygen extractor, pulse oximeter suitable for newborns. Neonates with respiratory distress were not treated with continuous positive airway pressure as soon as the diagnosis was made, according to WHO guidelines. This is due to the lack of a continuous positive pressure ventilation system in the department (Table 3). Premature newborns who appear to have surfactant deficiency were also not receiving exogenous surfactant treatment within two hours of birth according to WHO guidelines. However, the deficiency is responsible for respiratory distress called hyaline membrane disease (HMM) [13]. Its administration prevents alveolar collapse and also reduces the work of breathing [14]. All newborns with unknown gestational age are assessed using an adapted tool to determine gestational age. For this, the pediatricians of the neonatology unit used the most used method (Ballard score), which combines morphological and neurological criteria. Premature babies and cases of intrauterine growth retardation weighing less than 2000g whose clinical condition was stable benefited from the “kangaroo mother” method after one week of initiation of the mothers by the staff on said method. Meta-analyses show that the “kangaroo mother” method reduces neonatal mortality, halving the number of deaths in infants weighing less than 2000g [7]. According to the same source, it also reduces the rate of infections and septicemia by almost 60%. Premature newborns whose condition is unstable are placed in a clean incubator, and their temperature is regularly monitored. As shown in this article, all newborns with clinical signs associated with serious bacterial infections are clinically examined for premature rupture of membranes in the mother occurring more than 6 hours before birth or at the presence of a urinary tract infection or fever in the mother at any time between the start of labor and three days after birth. In the presence of a history of this type in addition to the clinical signs, the doctor may suspect a neonatal infection and prescribe a probabilistic antibiotic treatment composed of three (3) molecules (Gentamycin, Ampicillin and Cefotaxime) while awaiting the results of the routine biomedical analyzes (NFS, CRP, blood sugar, hepatic transaminases and bilirubinemia or transcutaneous bilirubin). It should be noted that the department's laboratory does not perform blood cultures. However, blood culture is the most widely used diagnostic tool to detect bacteremia and fungemia. A positive blood culture establishes or confirms the presence of an infectious etiology in the patient's illness [15]. It also specifies the etiological agent for the antibiogram, which makes it possible to target antibiotic treatment [15]. During the evaluation period, we observed that jaundice was also systematically monitored in all newborns; serum bilirubin level was measured in at-risk neonates and those with hyper bilirubinemia (200 µmol) received phototherapy treatment according to WHO guidelines. Newborns whose mothers tested HIV positive received Nevirapine according to the protocol. The same observation was made by Ouédraogo SO, et al. in Burkina Faso, who observed that all newborns born to HIV-positive mothers had received ARVs (111/114) from birth and were placed only on Névirapine syrup according to the protocol [16]. Before leaving the unit, staff advises the mother on possible danger signs (difficulty eating, reduced activity, difficulty breathing, fever, convulsions, and hypothermia) and when to return for Control. The analysis of human resources shows that the number of staff was insufficient in relation to the workload. It was composed of: 9.52% general practitioners acting as pediatricians, 14.29% pediatricians, 33.33% nurses and 20.63% non-professional health workers. During the day, the service operates with 15.4 beds per doctor and 11 beds per nurse, while at night; the service operates with 38.5 beds per doctor and 15.4 beds per nurse. According to the WHO, providing quality care requires investment in sufficient numbers of qualified providers to care for sick and low birth weight newborns, particularly trained and motivated nurses, who works in partnership with parents and families [7]. As for essential drugs used to treat sick newborns, they were frequently out of stock. These are vitamin K1/IM, diazepam injection, caffeine, Cefotaxime 1g, Gentamycin IV/IM, Chlorhexidine solution. However, essential medicines remain one of the fundamental axes of change and development of health systems [17]. They must be permanently available within the framework of operational health systems, in sufficient quantity, in the appropriate dosage form, with assured quality and at an affordable price at the individual level [17].
Table 4: Technical quality of care offered to newborns. View Table 4
It appears from this study that the care of the newborn encounters enormous difficulties. The analysis of human resources shows that the number of staff is insufficient in relation to the workload. During the day, the service operates with 15.4 beds per doctor and 11 beds per nurse, while at night; the service operates with 38.5 beds per doctor and 15.4 beds per nurse. The service does not have the necessary equipment to properly care for newborns with serious or minor pathologies. This deficit in equipment and personnel influences the quality of care for hospitalized newborns and can lead to high mortality (37.02%) as evidenced by the statistics for the year 2022. Any health establishment in care of sick newborns must have a suitable physical environment, equipped with adequate water supply, sanitation, waste management and energy supply systems. He must also have medicines, supplies and medical equipment for routine care and management of complications in sick and small newborns. This assessment made it possible to identify strengths and weaknesses. Better organization of newborn care in the INSE neonatology unit could contribute to reducing neonatal morbidity and mortality, by establishing standards for the organization of perinatal care.