Nephroenteric fistulas are rare and generally occur as a result of chronic inflammation, ischemia or necrosis. Nephrectomy and primary closure of the fistulous tract currently represent the mainstay of treatment for non-functioning kidneys but kidney preservation should be attempted in cases of traumatic fistulae. The authors report a case of a 69-year-old female with an infected subcapsular renal haematoma and a fistulous tract to the duodenum following ureteroscopic laser lithotripsy of a right proximal ureteral calculus.
Nephroenteric, Fistula, Haematoma
Fistulas between the kidney and the gastrointestinal tract are rare and generally occur as a result of chronic inflammation, isquemia or necrosis. Iatrogenesis has been identified as the third leading cause of duodenorenal fistulas. Subcapsular renal hematoma after URSL using Ho: YAG laser to treat proximal ureteric stones is also an extremely uncommon complication. Nephrectomy and primary closure of the fistulous tract are currently the mainstay of treatment. We report the case of an infected subcapsular renal haematoma with a fistulous tract to the duodenum following ureteroscopic laser lithotripsy of a right proximal ureteral calculus, treated conservatively with antibiotics and kidney preservation.
A 69-year-old female patient with no relevant medical history other than renal stones was admitted to the ER Department with acute right flank pain, fever and nausea. On physical examination, the patient had a positive right Murphy’s sign. Analytically, leukocytosis combined with elevated C-reactive protein and a urinalysis consistent with urinary tract infection were present. Ultrasound was initially performed and was immediately followed by contrast-enhanced Computed Tomography (CT) (Figure 1), which revealed a 6 cm well-defined, right upper renal subcapsular mass with low attenuation, enhancing walls and gaseous content, consistent with an infected subcapsular hematoma. Anteriorly, a continuous irregular gas-containing tract was observed between the hematoma and the second portion of the duodenum, in keeping with a nephroenteric fistula. Contrast-enhanced MRI (Figure 2) was then performed, confirming the fistulous tract with clearly thickened enhancing walls between the haematoma and the gastrointestinal tract.
 Figure 1: Axial-view contrast-enhanced CT in the corticomedullary (A) and nephrographic (B) phases and coronal-view CT in the corticomedullary phase (C) showing a right renal subcapsular collection with enhancing walls in keeping with a subcapsular haematoma (white arrowhead in A, B and C). A fistulous tract between the haematoma and the duodenum with gaseous content can be seen (arrow in A). Just inferiorly, gaseous content can also be seen inside the haematoma (arrow in B). View Figure 1
Figure 1: Axial-view contrast-enhanced CT in the corticomedullary (A) and nephrographic (B) phases and coronal-view CT in the corticomedullary phase (C) showing a right renal subcapsular collection with enhancing walls in keeping with a subcapsular haematoma (white arrowhead in A, B and C). A fistulous tract between the haematoma and the duodenum with gaseous content can be seen (arrow in A). Just inferiorly, gaseous content can also be seen inside the haematoma (arrow in B). View Figure 1
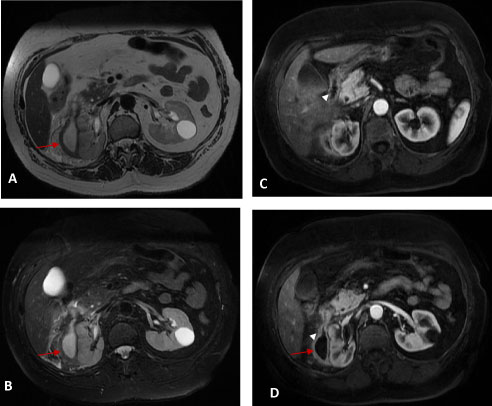 Figure 2: T2W (A), T2W FS (B) and contrast enhanced arterial phase T1W (C and D) MR images clearly depicting the right renal subcapsular haematoma (arrows in A and B) with thickened and enhancing walls (arrow in D) in keeping with an infected subcapsular haematoma. The duodenum can be seen superiorly (white arrowhead in C) and, just inferiorly, a fistulous tract with thickened enhancing walls is seen (white arrowhead in D). View Figure 2
Figure 2: T2W (A), T2W FS (B) and contrast enhanced arterial phase T1W (C and D) MR images clearly depicting the right renal subcapsular haematoma (arrows in A and B) with thickened and enhancing walls (arrow in D) in keeping with an infected subcapsular haematoma. The duodenum can be seen superiorly (white arrowhead in C) and, just inferiorly, a fistulous tract with thickened enhancing walls is seen (white arrowhead in D). View Figure 2
The patient had a history of ureteroscopic laser lithotripsy (URSL) of a right proximal ureteral calculus one month prior. Preoperatively, a ureteral stent had been placed and surgery was carried out with no apparent complications. Cystoscopy and stent removal had been initially performed, followed by insertion of a safety-guide wire. A rigid ureteroscope was then advanced to the uretero-pelvic junction and the 2.5 cm calculus was fragmented with laser lithotripsy using a 270 micron laser fiber with high energy, partially migrating to the lower caliceal pole. A retrograde pyelogram was performed for inspection of all calyces and a second guide-wire was introduced in the upper calyx and a 11/13 access sheath was advanced through the guide wire under fluoroscopic guidance. Flexible ureteroscopy was then performed and complete laser lithotripsy was carried out. The access sheath was removed under direct endoscopic visualization and no lesions to the ureter were observed. A ureteral stent was placed under fluoroscopic guidance and the bladder was emptied. After postoperative observation and evaluation, the patient was discharged home.
Fistulas between the kidney and the gastrointestinal tract (nephroenteric) are rare. They constitute less than one per cent of fistulas between the urinary system and the alimentary canal [1]. Of these, colorenal fistulas are the most frequent subtype, with duodenorenal fistulas being extremely uncommon [2]. A recent systematic literature review identified complicated pyonephrosis as the leading cause of duodenorenal fistulas, followed by complicated nephrolithiasis, iatrogenic causes, malignancy and gastrointestinal causes, infectious disease and trauma and xantho granulomatous pyelonephritis [3]. They generally occur as a result of chronic inflammation, ischemia or necrosis [2] and are more frequent on the right side due to anatomic proximity [4]. Renoduodenal fistulas, as in our case, most commonly involve the second portion of the duodenum not only due to close contact with the anterior kidney, but also due to its relative lack of mobility and absence of posterior peritoneal coverage [5-7].
According to literature, symptoms characteristically range between unspecific epigastric or flank pain, nausea or vomiting, fever, voiding difficulty, weight loss, diarrhoea or constipation and gastrointestinal bleeding [1,5,6]. As in our case, laboratory findings are frequently consistent with leukocytosis and urinary tract infection [5].
Subcapsular renal hematoma after ureteroscopic lithotripsy (URSL) using holmium: Yttium-aluminum-garnet (Ho: YAG) laser to treat proximal ureteric stones is also an extremely uncommon complication. Tao, et al. [8] reported only three cases in a series of 2059 patients and Chiu, et al. [9] reported only 4 cases of subcapsular hematoma in a series on 1114 URSLs performed over a 5-year period. On the other hand, subcapsular hematoma is a well-documented complication of shock wave lithotripsy, renal angiographic procedures [10] trauma, renal masses and anticoagulation therapy [11]. Even though it is still unclear, proposed aetiologies for the development of subcapsular renal hematoma after URSL are trauma to the pelvicalyceal system during guide wire manipulation and an increase in intrarenal pressure causing forniceal rupture with consequent capsular separation from the renal parenquimal [12].
Contrast-enhanced CT is the current method of choice for the diagnosis of subcapsular renal hematomas and nephroenteric fistulas. Imaging should be performed in both the nephrographic and urographic phases.
Nephrectomy and primary closure of the fistulous tract are still the mainstay of treatment when the affected kidney is non-functioning [1,5,6]. Kidney preservation should be attempted for traumatic fistulae. In our case, due to the iatrogenic nature of the fistula and normal renal function, the haematoma was drained and the patient was started on systemic antibiotics, with the kidney being preserved. Kidney function remained stable 4 months later.
All authors have contributed, read and approved this manuscript.
The authors report no conflicts of interest.