Background: The two most common autografts for anterior cruciate ligament (ACL) reconstruction (ACLR) are bone-patellar tendon-bone (BPB) and semitendinosus-gracilis (STG). There is currently no consensus on the optimal graft choice. The type of graft chosen for ACLR is often made by the physician with minimal input from the patient. The primary aim of this study was to review the current literature and examine differences in post-operative care, time to discharge, and clinical outcomes between the two procedures. Secondarily, we examined the results of the current literature pre- and post-assessments for patients' initial treatment and rehabilitation using the autograft surgical technique.
Methods: Following the PRISMA method, a comprehensive electronic search was performed using the terms "anterior cruciate ligament" OR "ACL" AND "bone patellar tendon bone graft" OR "BPB" then "anterior cruciate ligament" OR "ACL" AND "semitendinosus gracilis graft" OR "SGT". A systematic electronic literature search was performed using specific search terms in PubMed and Google Scholar databases to identify relevant publications. The search terms used were "anterior cruciate ligament" OR "ACL" AND "bone patellar tendon bone graft" OR "BPB" then "anterior cruciate ligament" OR "ACL" AND "semitendinosus gracilis graft" OR "SGT". Additional search criteria included publication date after January 1, 2000. Following the initial identification based on search terms, 76 articles were selected using inclusion criteria from the title and abstract. A secondary inclusion/exclusion criterion of the full articles yielded the remaining 20 articles that comprise this review. A detailed description of inclusion and exclusion criteria may be found in the methods section of the manuscript.
Results: Of the 20 articles that constitute this review, five reported on BPB, nine on STG, and six both STG and BPB. Fixation type and graft specifications varied between the studies reviewed. The predominant fixation type was a form of the bioabsorbable screw or interference screw. The second most common fixation technique was a form of the Endobutton on the femoral side and the bioabsorbable screw on the tibial side of fixation. The predominant STG graft specification was the four-stranded. BPB graft specifics were not identified, and it was assumed the graft was a bone end of tibial tuberosity-tendon-bone end of the inferior pole of the patellar. The findings indicated similarities in patient clinical outcomes and time to recovery, such as the time to begin rehabilitation, achieving full knee extension, time to treadmill straight-line running, and time to sport-specific or pivoting exercises, were all similar between BPB and SGT.
Conclusion: Even though outcomes were similar between the two surgical approaches, SGT appears to be preferred more than twice as often and was predominantly used on population groups returning to non-contact sports. Perhaps this finding might be described as a starting point to further explore factors affecting physician decision-making. BPB is also associated with anterior knee morbidity, so patients participating in contact sports or jumping/power athletes should consider STG as the better option. Likewise, given previous evidence suggesting that STG may not be as stable due to the lack of boney fixation, athletes engaged in substantial pivoting and change of direction may want to consider BPB.
ACL reconstruction, Knee ligament surgery, Post-operative knee rehabilitation
The anterior cruciate ligament (ACL) is one of the primary stabilizing ligaments within the knee joint [1,2]. Its purpose is to stop anterior and rotational movement of the tibia over the femur, and it is responsible for about 85% of knee stability [2,3]. The ACL is susceptible to injury in pivoting, jumping, and cutting maneuvers as it endures significant rotational stress [4]. Given its extensive use, it is the most torn ligament within the knee joint [5]. In the United States, ACL rupture occurrences range between 100,000 to 250,000 cases annually [4,6,7], and roughly 70% occur due to non-contact injuries [4]. Non-contact injuries predominately occur during field sports such as soccer or football [8,9]. Most non-contact tears occur near the femoral attachment site [10], with females experiencing a higher injury rate than their male counterparts [5,7,10,11]. This is due in part to multi-dimensional biomechanical characteristics, specifically, but not exclusively, weaker hamstring to quadricep strength ratio, weak external rotator musculature of the femur, hormonal influx (such as Relaxin) during the menstrual cycle, and wider pelvic bone structure increasing the potential for an increased Q-angle [12,13]. Given the importance of the ACL in knee stability, injuries of ten result in subsequent meniscus tears and other cartilage and ligamentous damage [1]. Cartilage injuries are a common co-occurrence with ACL tears, with up to 65% of all ACL injuries coupled with a meniscus tear [14]. ACL reconstruction is commonly performed on active individuals who intend to return to athletic activities that require cutting and jumping and to restore joint stability and function [3,7].
ACLR is a complex procedure encompassing many techniques, including graft choice, drill angle and site, use of regenerative agents (platelet-rich plasma), and bone cement or fixation. There is substantial variability between approaches regarding patient outcomes and re-tear rates. Graft selection is a significant component of this surgery and may affect patient outcomes. Both autografts (the use of one’s own tissues) and allografts (the use of cadaver or synthetic tissues) are utilized for reconstruction in this procedure. The two most common autografts for ACLR are bone-patellar tendon-bone (BPB) and hamstring (STG; semitendinosus and gracilis tendons) [1,15]. Less frequently used is quadricep tendons (QT), another autographic procedure [16]. The literature indicates that QT grafts have knee stability outcomes and graft survival rates comparable to BPB and STG [16,17]. Common allografts used in ACL reconstruction arise from a chilles tendon, tibialis anterior, or tibialis posterior tendons [1]. Allografts are reported to have a much higher rupture rate compared with autografts, especially in young patients returning to competitive sports [17,18]. In other words, allografts in younger active populations may result in re-tear more often than that of autografts.
BPB autografts are widely accepted as a standard, and their effectiveness is often compared to that of other grafts [15]. The BPB graft involves the central third of the patellar tendon. It includes removing a small portion of the tibial tuberosity and the patellar’s inferior pole, allowing for bone plugs at either end to help with fixation [15]. However, BPB is known to result in harvest site morbidity and other complications, such as pain when kneeling, patellar fracture, and anterior knee pain [15,18].
The STG autograft has less donor site morbidity, with some research suggesting regeneration of the tendons [15]. The major criticism of hamstring autografts is that their strength and stiffness are not equal to that of the native ACL or other potential grafts with a bone plug; however, this is attenuated by a quadruple technique that helps strengthen the graft [15]. SGT autografts are fed through a tunnel in both the tibia and femur and secured using multiple techniques [19]. The grafts are also often fixed using screws and/or bone cement mixture, allowing for a strong hold and quick graft incorporation [15]. Techniques for graft attachment vary, and common techniques include interference screw fixation and suspensory button fixation [20].
ACLR techniques and their performance have changed drastically in the last several decades, with current practice employing arthroscopy [4]. Surgery is also now the gold standard for younger individuals who intend to return to pre-injury levels and athletic play [4]. Several studies indicate no “best graft” for ACLR [19]. SGT autografts can be preferred in specific cases, such as patients with preexisting patellafemoral problems and previous failed BPB grafts [21]. BPB tends to be favored in athletes who intend to return to competitive sports after reconstruction due to some indication of greater knee stability [19]. Current research indicates surgeons should explain to patients the differences and risks/benefits of each graft before selecting one [19].
There is little consensus on optimal rehabilitation following ACLR, but most agree that physical therapy is a critical component of recovery [4,22]. The purpose of rehabilitation programs is to rebuild muscle strength with an emphasis on the quadriceps and hamstrings, to reestablish joint mobility, to prevent knee extension deficits, and to allow patients to return to their pre-injury activity levels [4,22]. Rehabilitation from this surgery tends to be a lengthy process, between 6 and 12 months [23]. Approximately 40% to 95% of athletes return to their previous level of play after surgical intervention and extended rehabilitation [23]. An important note in rehabilitation protocols is how graft selection may affect recovery. For instance, BPB grafts often result in anterior knee morbidity, and these patients may require altered rehabilitation protocols. Additionally, STG grafts may require special attention to improve hamstring strength and often do not have restrictions or limitations with anterior knee rehabilitation exercises [19,21]. Rehabilitation protocols are a delicate balance between preventing re-rupture of the repaired ACL tendon and reestablishing strength with minimal loss of muscle mass and mobility [4,24]. There are large variations in rehabilitation programs, but most are moving toward accelerated protocols that encourage early movement and strength recovery [25]. Preoperative rehabilitation (prehab) is indicated to improve post-surgery results, with patients having higher post-operative knee muscle strength, reaching milestones quicker, gaining higher scores on functional performance tests (FPTs), and a higher likelihood of returning to pre-injury sports [4].
Revised American Physical Therapy Association (APTA) guidelines indicate immediate mobilization of the knee within one week following ACLR [4]. This contributes to an increased range of motion and a reduced risk of damage to surrounding soft tissue structures [4]. Revised guidelines also focus on earlier weight-bearing incorporated with a step-up approach to non-weight bearing and weight-bearing activities and early achievement of full knee extension [4]. Many studies indicate that reestablishing quadriceps strength is vital to rehabilitation and contributes to lower extremity stability [4,24]. FPTs are often used at the end of rehabilitation to determine a patient’s ability to return to play [4,23,26]. This test often includes single leg hop or squat, in-line lunges, and other sport-specific movement tests [23].
The purpose of this study was to review current literature (published after January 1, 2000) relative to patients ≥ 13 years of age who underwent autographic ACLR by BPB or SGT. Specifically, the primary aim was to compare the following outcomes: Post-op care, time to discharge, and time to recovery between surgical techniques by surgical technique. Further, the researchers reviewed the selected studies pre-and post-assessments for patients’ initial treatment, rehabilitation, and provided the total number of cases for each surgical technique.
This review followed there commendations and structure of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) checklist.
A systematic electronic literature search was performed using specific search terms in PubMed and Google Scholar databases to identify relevant publications. The search terms used were “anterior cruciate ligament” OR “ACL” AND “bone patellar tendon bone graft” OR “BPB” then “anterior cruciate ligament” OR “ACL” AND “semitendinosus gracilis graft” OR “SGT”. Additional search criteria included publication date after January 1, 2000.
Studies in which patients underwent an initial ACLR using either BPB or SGT autografts for an isolated ACL rupture were eligible for inclusion. In addition, specific clinical outcomes such as post-op care, time to discharge, and time to recovery were potentially eligible for inclusion.
Studies were excluded based on any of the following criteria:
- Revision surgery
- Allografts: Cadaver or synthetic grafts
- Quadricep tendon graft
- Multi-ligament reconstruction
- No rehabilitation discussion
- Animal or cadaver studies
- Meta-analysis research studies
The initial selection of articles based on the abstract and title was performed by a single reviewer using the inclusion and exclusion criteria. All selected articles were in English and published between January 1, 2000, and January 31, 2023. Next, full-text articles were reviewed for inclusion/exclusion using the established criteria. The authors reported no conflicts of interest relative to the selected studies.
A standard spreadsheet was built prior to data extraction using Microsoft software. Four reviewers independently extracted study data, with disagreements resolved by consensus. The following data were extracted: Author name and publication year, patient demographics (number, gender, age, activity type), pathologies, methods and surgical information, time from tear to surgery, clinician type, pre-rehabilitation assessments, intra-intervention assessments, post-intervention assessments, rehabilitation technique information, rehabilitation milestones and goals, timeline for milestones and goals, results of Return to Play (RTP) or Active Daily Living (ADL) assessments, time to discharge, and any other notable findings or results.
A review based on the clinical outcomes previously mentioned and ordinal categorical variables was conducted to compare results between BPB and SGT.
The authors conducted a comprehensive literature search and identified 76 potentially eligible research studies in the abstract, first-round review. Of these, 30 were case studies, 9 were reviews or meta-analyses, and 37 were retrospective reviews. The second round of review resulted in the exclusion of 56 studies based on the criteria identified above. The remaining 20 studies were deemed eligible for comparative review. Figure 1 denotes the search procedure and basis for inclusion/exclusion.
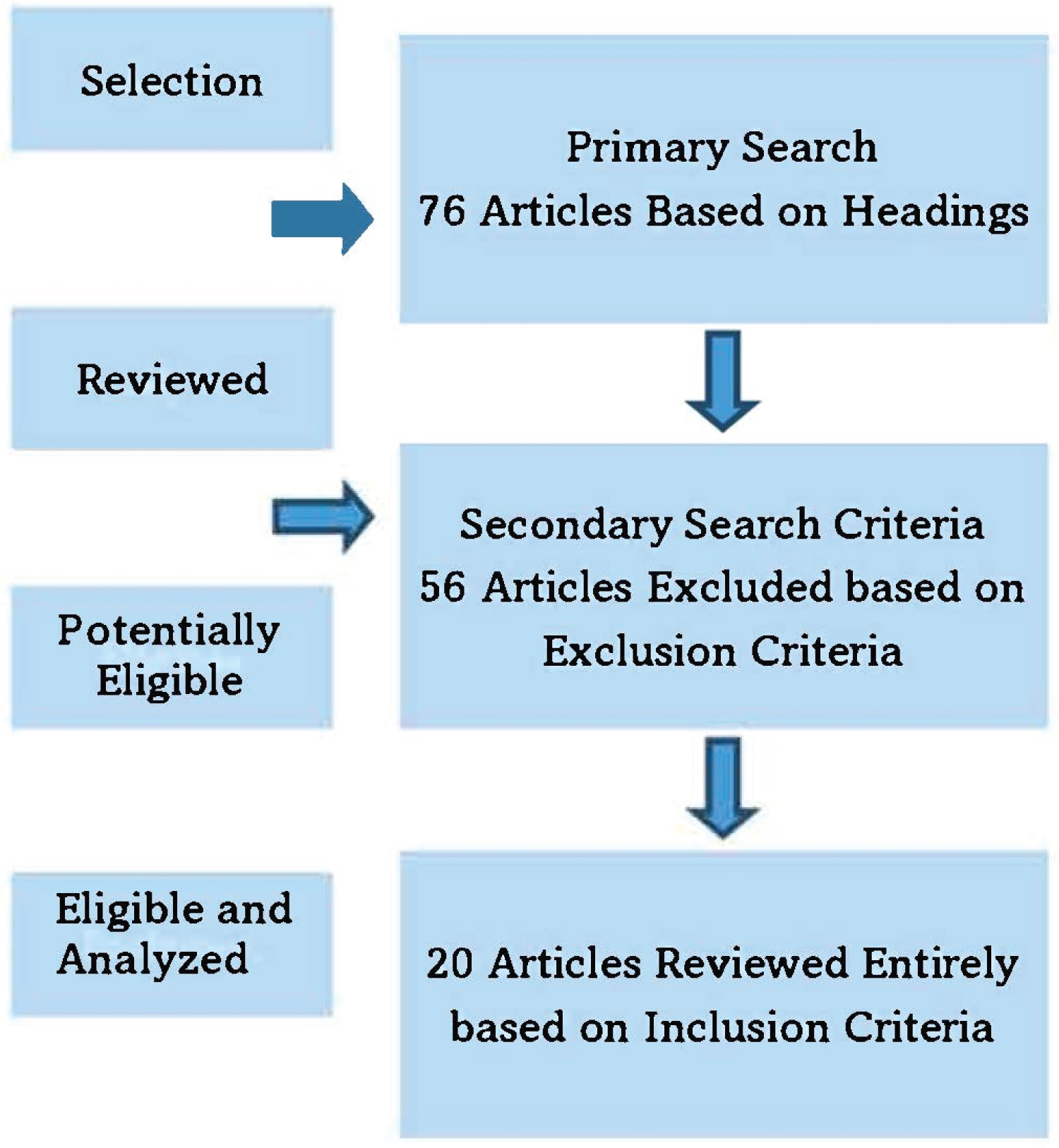 Figure 1: Flowchart for the systematic review of the literature.
View Figure 1
Figure 1: Flowchart for the systematic review of the literature.
View Figure 1
Of the 56 articles excluded, 21 were BPB, 12 were STG, and 29 were BPB and STG due to revision exclusion criteria. Table 1 provides information on the number of articles excluded by category, identifying the exclusion criteria.
Table 1: Study exclusions. View Table 1
Of the 20 articles that constitute this review, five reported on BPB, nine on STG, and six both STG and BPB. Patient demographics are provided in Table 2. The total number of patients included in the BPB and STG studies were 665 and 1634, respectively. Figure 2 illustrates the percentage of total patients by surgical type. The biological sex and gender breakdown for both BPB and STG was not recorded in all the cases. Of the cases that recorded biological sex or gender, the breakdown was BPB- 253 males, 128 females; STG- 772 males, 386 females. The age ranges were: BPB, 18-30; STG, 18-35 years. Figures 3 and Figure 4 illustrate the percentages for the gender breakdown between BPB and STG for all participants recorded in the studies.
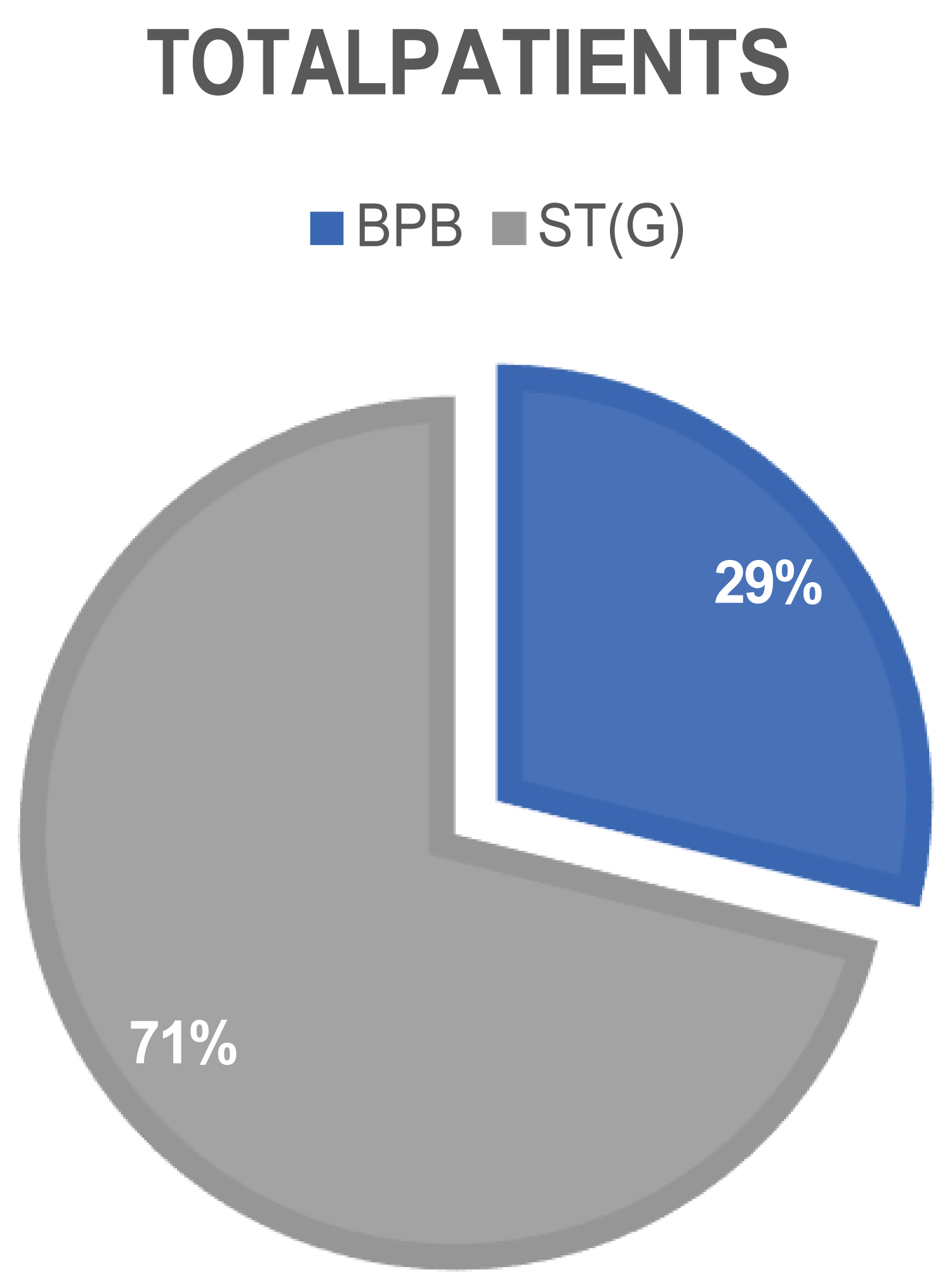 Figure 2: Percent of total number of patients (n = 2299) by procedure type.
View Figure 2
Figure 2: Percent of total number of patients (n = 2299) by procedure type.
View Figure 2
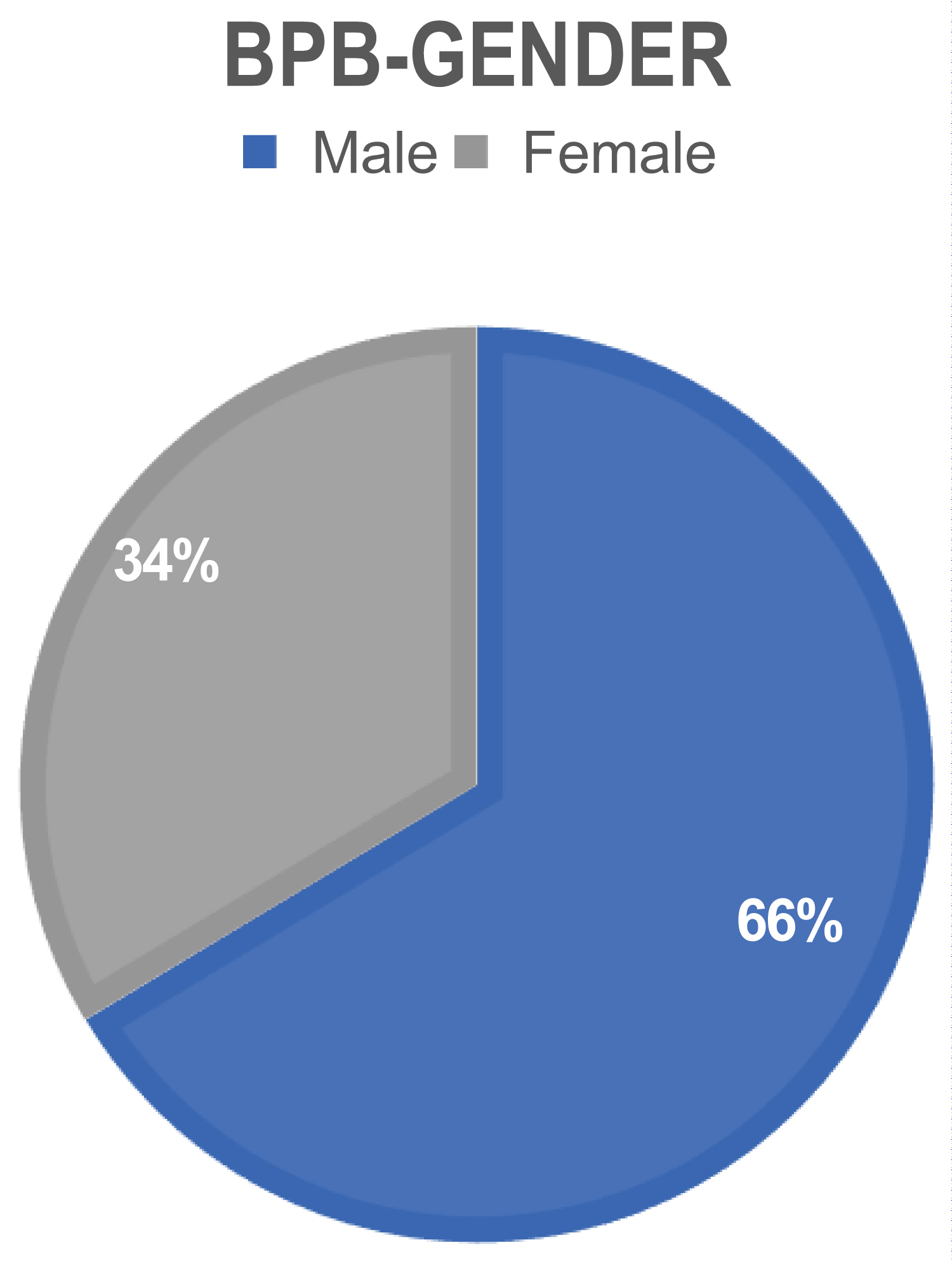 Figure 3: Percent of total number of BPB patients (n = 665) by biological sex or gender identified in the studies.
View Figure 3
Figure 3: Percent of total number of BPB patients (n = 665) by biological sex or gender identified in the studies.
View Figure 3
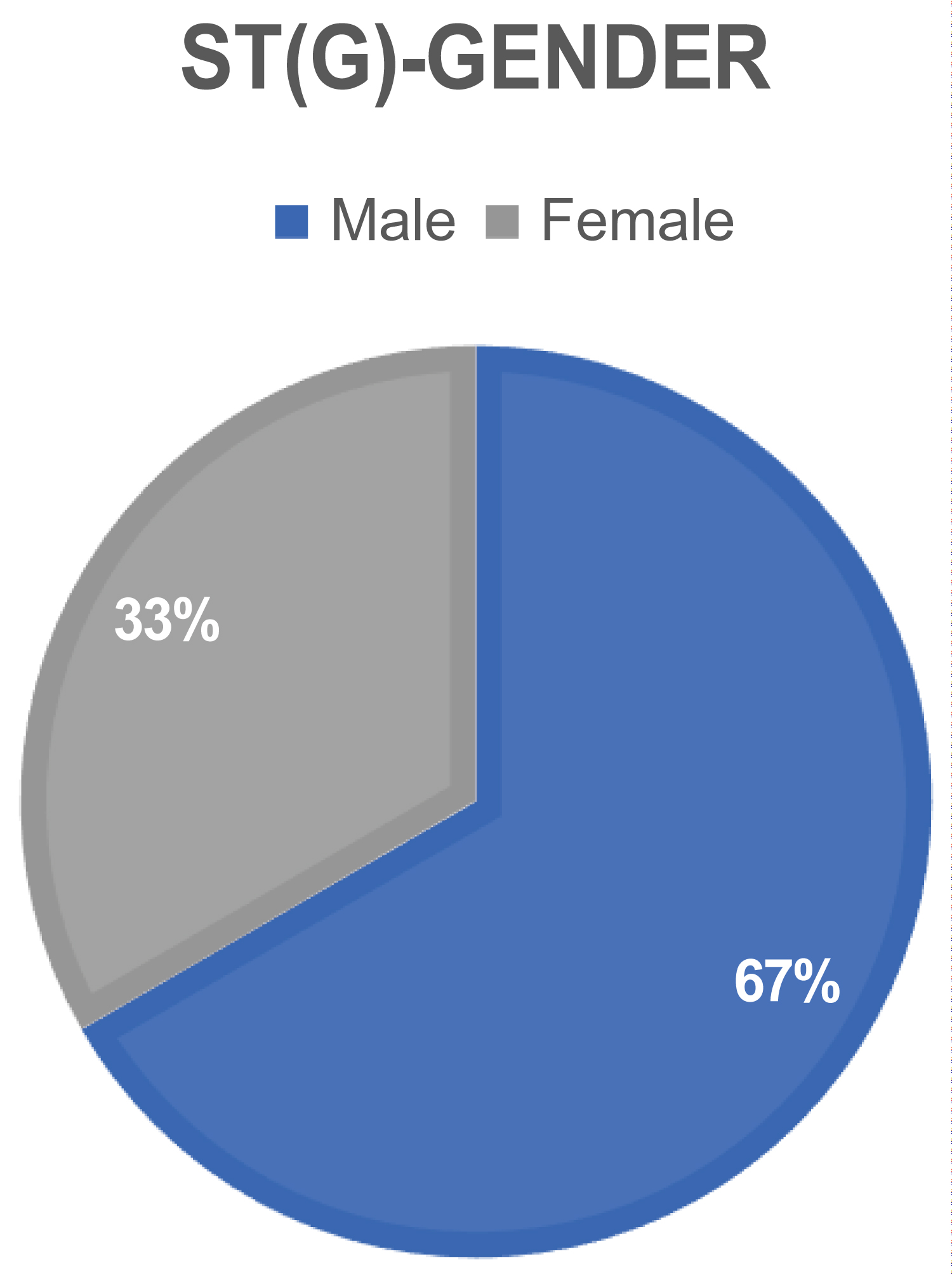 Figure 4: Percent of total number of STG patients (n = 1634) by gender.
View Figure 4
Figure 4: Percent of total number of STG patients (n = 1634) by gender.
View Figure 4
Table 2: Patient demographics and impacted side BPB (Gender) (STG Gender) BPB (Side) STG (Side). View Table 2
The location or affected limb that underwent surgery was not recorded for each patient in all the cases. In the cases that identified the affected limb that underwent surgery, the breakdown was as follows: BPB, 203 left limbs, and 215 right limbs. Surgical limb side for STG, 357 left limbs and 325 right limbs. Figures 5 and Figure 6 illustrate the percentage of impacted sides, otherwise termed surgically affected limb.
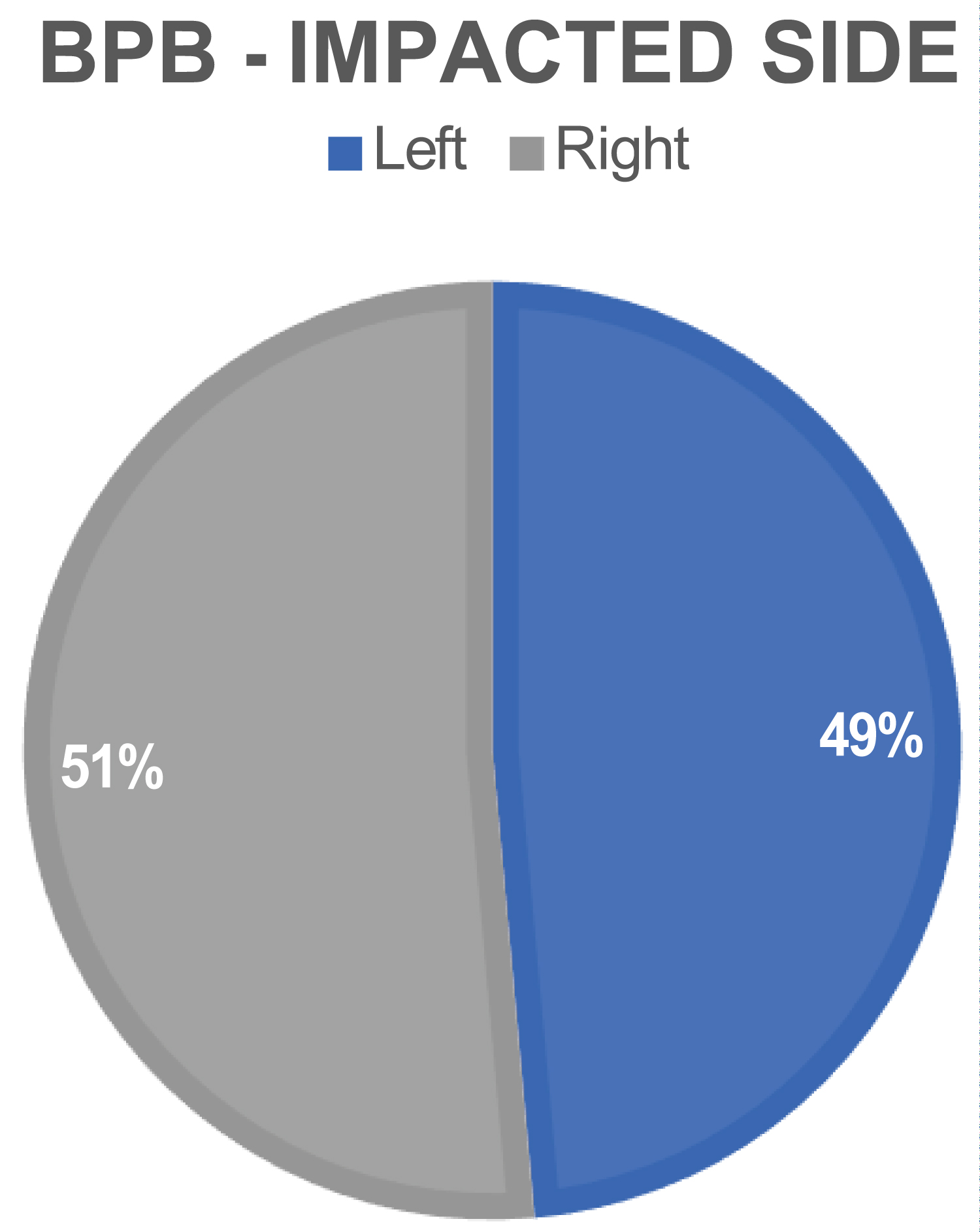 Figure 5: Location of the surgically affected side, BPB (percent).
View Figure 5
Figure 5: Location of the surgically affected side, BPB (percent).
View Figure 5
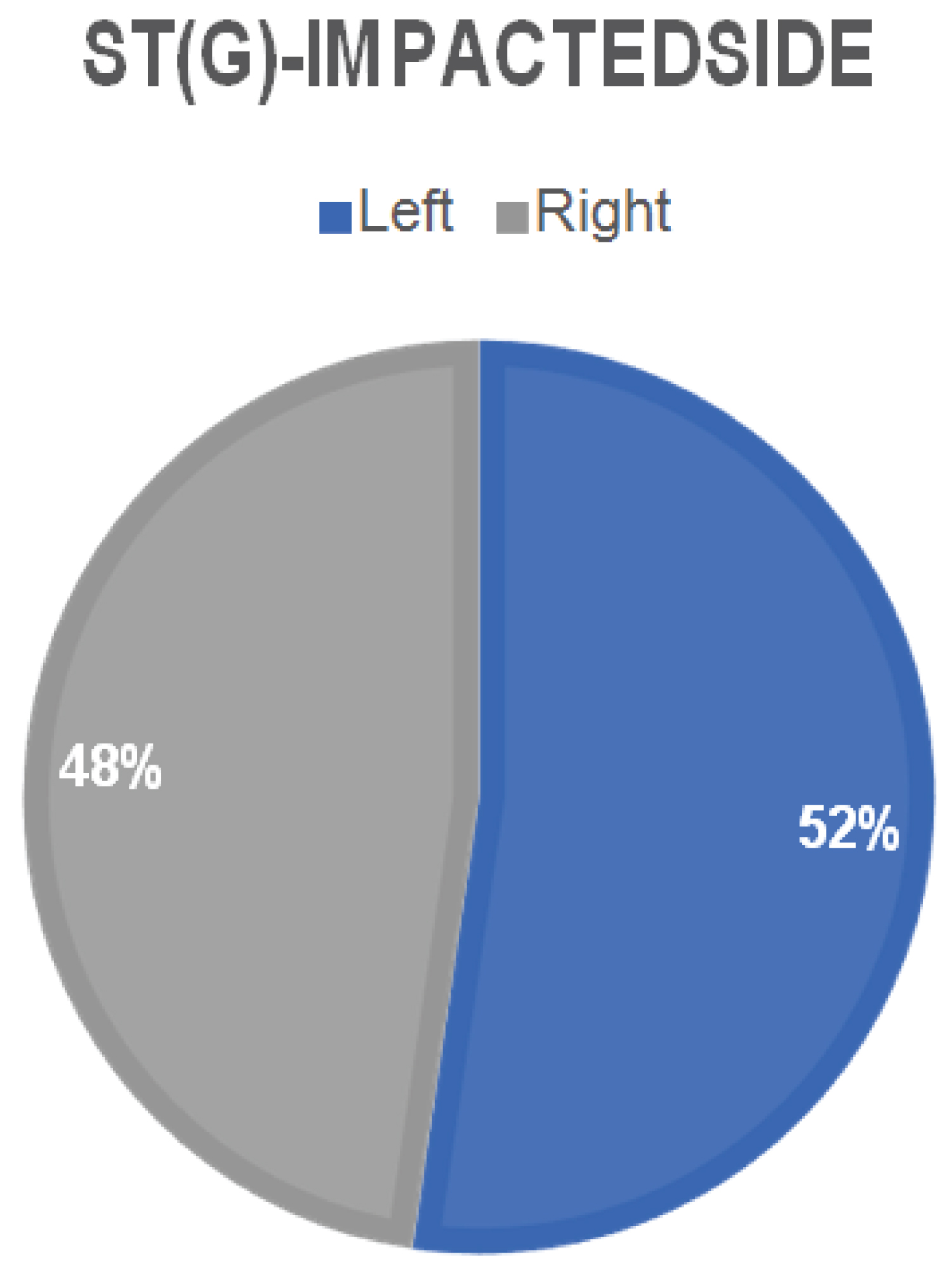 Figure 6: Location of the surgically affected side, STG (percent).
View Figure 6
Figure 6: Location of the surgically affected side, STG (percent).
View Figure 6
Mechanism of injury (MOI) was not a primary or secondary aim of this study, nor did most studies report MOI. Nonetheless, an interesting note of those who did report MOI was that non-contact injuries were more prevalent than contact injuries. Ten studies mentioned specific activities that resulted in the injury: Soccer, basketball, Amer. football, Aus. Football, and skiing were the most common causes reported.
All studies provided data on surgeries that occurred after the year 2000. Of the 20 studies constituting this review, several identified patients with comorbid pathologies. Specifically, ten articles included patients with meniscal pathology, and one study included other ligament injuries, such as the medial collateral ligament.
Rousseau, et al. [40] reported on 811 ACL reconstruction patients, of which 388 sustained a meniscal pathology and underwent surgical intervention along with the ACL reconstruction. Similarly, Laxdal, et al. [45] reported on 118 patients, 40 BPB and 78 STG. Of the 134 patients, 23 BPB and 46 STG included meniscal surgery. Maletis, et al. [44] reported on 99 total patients, all receiving meniscal surgical intervention in addition to ACL reconstruction. Lastly, Mascarenhas, et al. [41] and Barber, et al. [28] included 38 and 16 patients who received meniscal surgical interventions, respectively. This will be an essential aspect to review within the discussion portion of the paper since it directly affects patient outcomes and may increase time to recovery and range of motion (ROM) deficits between ACL graft types.
Fixation type and graft specifications varied between the studies reviewed. The predominant fixation type was a form of the bioabsorbable screw or interference screw. The second most common fixation technique was a form of the Endobutton on the femoral side and the bioabsorbable screw on the tibial side of fixation. A less used fixation type was herloc device or the suture disc. The predominant graft specification for STG was the four-stranded or quadrupled type. Less used for STG was the double-looped type. BPB graft specifics were not identified, and it was assumed the graft was, as mentioned, a bone end of tibial tuberosity-tendon-bone end of the inferior pole of the patellar. Only one study, Kaneetal [27], mentioned using a central 1/3 rd portion of the tendon BPB tendon graft.
Of the 20 articles, seven studies identified the amount of time the patient waited until surgical intervention. Of these seven studies, the predominant amount of time-to-surgery, injury to surgery, was within three months. The second highest time-to-surgery metric was within a year but greater than three months. Lastly, time-to-surgery, that is longer than a year, was only reported by one study. The time to surgery did not appear to impact the outcomes of the patients reported in the study, as their recovery time was similar to that of the other studies reviewed. Thus, the time to surgery may be of interest as it did not influence the reported outcomes of the patients.
Clinical assessments completed for each study are listed in Table 3. Follow-up data were collected for most articles reviewed, with the average time to initial follow-up 24 months. The number of follow-up visits varied for all studies, but all reported at least one.
Table 3: Clinical assessment data. View Table 3
Of the 20 articles reviewed, six studies identified a rehabilitation protocol type, while the other fourteen articles discussed a variation of the rehabilitation process. The predominant rehabilitation type was the progressive or accelerated rehabilitation protocol. One article reported a patient-directed (home-based) program, another identified a step/wise graduated RTS, and lastly, one article reported an aggressive control rehabilitation program. Most articles reviewed discussed using a post-operative brace, some with a locking hinge, others freely movable. The articles where meniscal surgical intervention was identified included ROM restrictions for their patients. The timeline restrictions varied between articles, potentially suggesting a variance in the optimal time to maintain ROM restrictions for an ACLR with meniscal surgical intervention. Nevertheless, the timeline range and type of ROM restriction was roughly 2-4 weeks long, with a restriction of either full extension or 60-90 degrees of limited flexion. Weight-bearing exercises and gait were restricted for all ACLR and ACLR meniscal patients reported within the studies reviewed. However, time to full weight bearing (FWB) exercises differed for all studies reviewed. Similar to restricted ROM, patients with meniscal surgical intervention demonstrated a longer time to FWB activities. Refer to Table 4 regarding the rehabilitation data examined. Articles reporting no restrictions on weight-bearing exercises, in other words, allowing FWB activities as tolerated, were predominantly reporting on ACLR patients without meniscal surgical intervention.
Table 4: Rehabilitation data. View Table 4
Most articles reviewed provided a timeline of when patients began specific rehab milestones. The milestones mentioned in the articles reviewed include the start of rehab, treadmill, straight-line running, swimming, biking, pivoting exercises, and sport-specific exercises. The milestones are illustrated in Figure 7, Figure 8, and Figure 9; the graphs represent each milestone start point categorized by article type, BPB, STG, and Both. Most articles' average time to begin rehabilitation was the first week of post-operation. Straight-line running start-timelines ranged between 8-16 weeks (about three and a half months), excluding the outliers of 4 weeks for an early start and 20 weeks (about four and a half months) for a later start time. The articles identifying meniscal surgical interventions with ACLR are similar in their reported timeline range for straight-line running compared to straight ACLR. The time to begin sport-specific exercises ranges from 10-28 weeks (about six and a half months). This large differential between start times may be partly due to the sport type and the intensity of the sport-specific exercise. Interestingly, the studies reporting meniscal surgical intervention did not report sport-specific exercises in their findings.
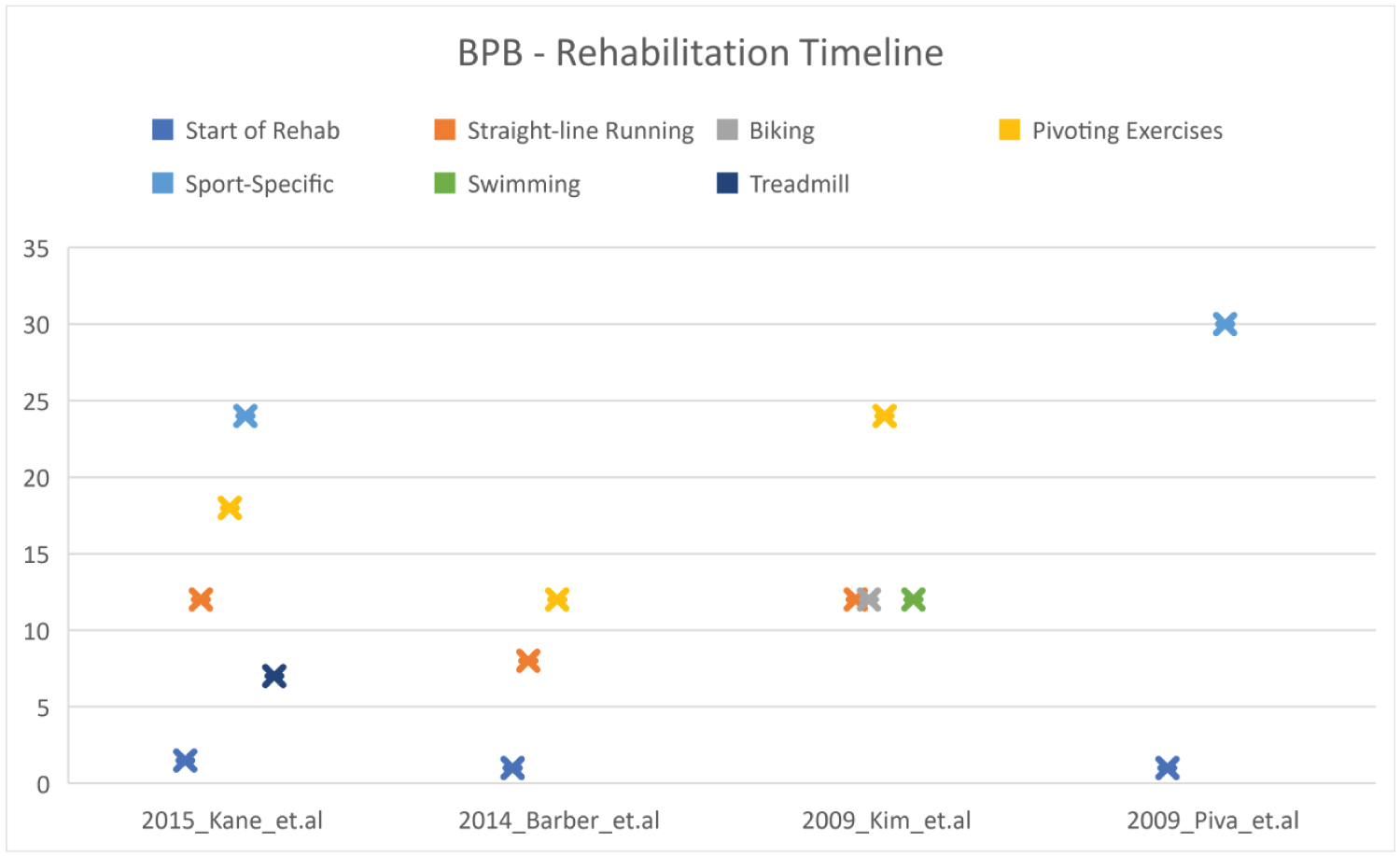 Figure 7: BPB articles milestone rehabilitation timeline.
View Figure 7
Figure 7: BPB articles milestone rehabilitation timeline.
View Figure 7
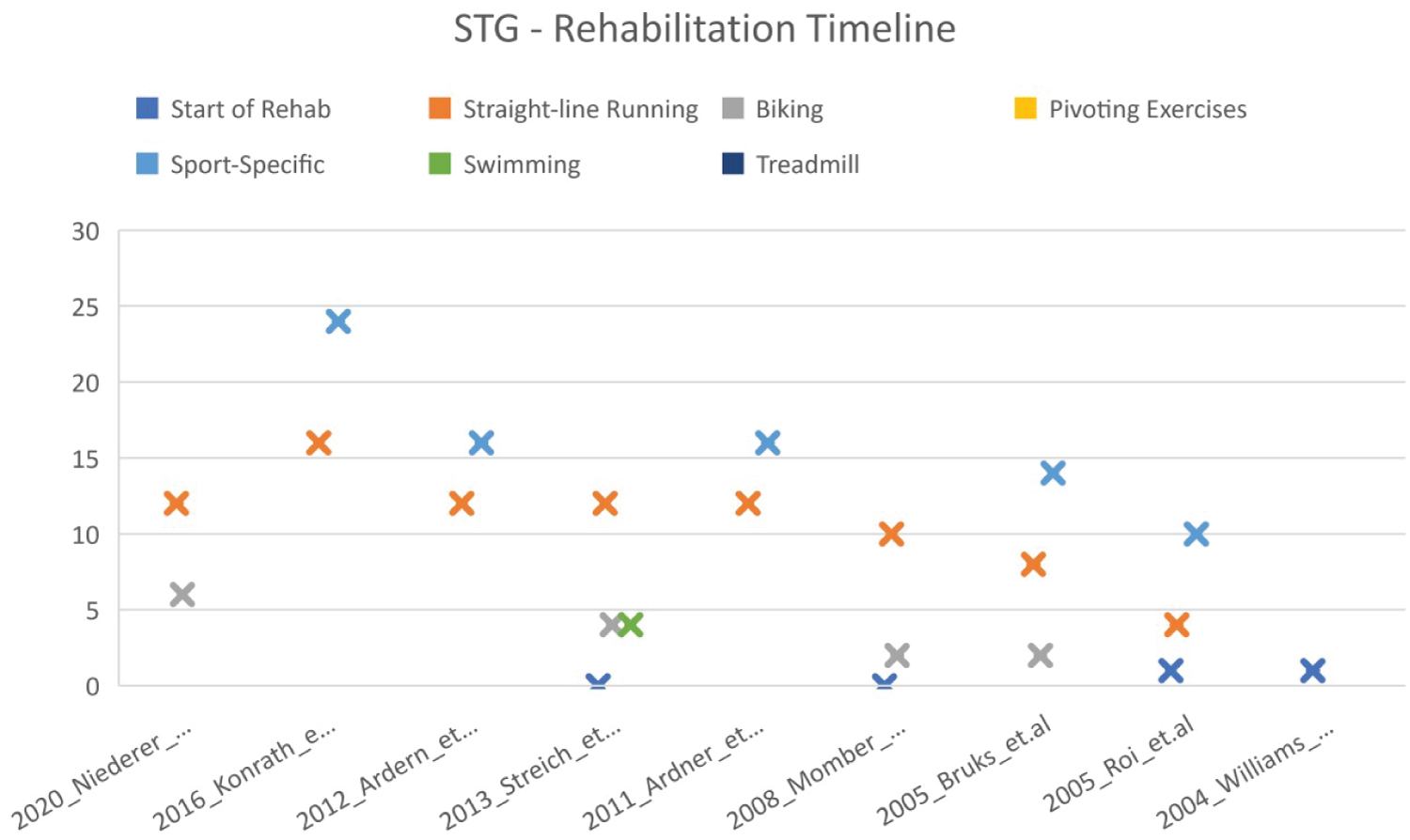 Figure 8: STG articles milestone rehabilitation timeline.
View Figure 8
Figure 8: STG articles milestone rehabilitation timeline.
View Figure 8
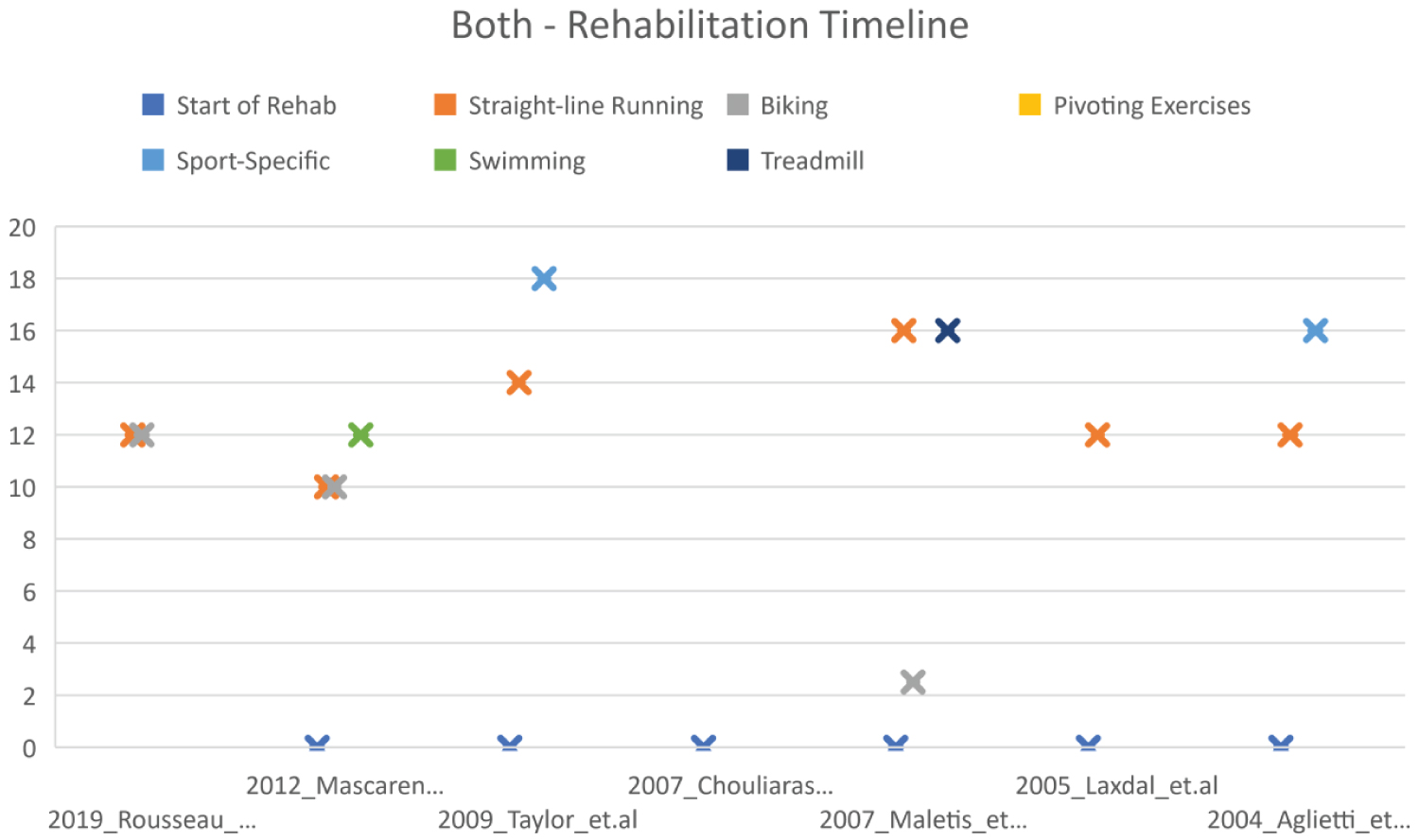 Figure 9: BOTH- Articles including both STG and BPB pts. milestone rehabilitation timeline.
View Figure 9
Figure 9: BOTH- Articles including both STG and BPB pts. milestone rehabilitation timeline.
View Figure 9
Rehabilitation goals and results are provided in Table 5. The predominant reported rehabilitation goal was to return to play (RTP) with a timeline range of 20-36 weeks after removing the outlier, 11 weeks RTP.
Table 5: Rehab results. View Table 5
In this study, patient recovery, outcomes, and time to rehabilitation discharge were consistent between patients who underwent BPB or STG. Interestingly, 71% of patients received STG vs. 29% who received BPB, given that BPB is presented as the standard choice in the current literature [15]. Further, STG was used predominantly on population groups returning to non-contact sports. Variances were seen in assessment techniques and follow-up, presumably based on physician preference. Regarding patient outcomes and the rehabilitation milestones, the review revealed that the choice of surgical procedure (BPB vs. SGT) was not as predictive as whether the patient received a meniscus repair in addition to the ACLR. This finding is consistent with previous literature as the meniscus repair adds to the rehabilitation protocol and increases the number of early restrictions, specifically, ROM, time to weight-bearing exercises, and bracing, among others [14]. Specifically, the time to begin rehabilitation, achieving full knee extension, time to treadmill and straight-line running, and time to sport-specific or pivoting exercises were all similar between BPB and SGT. This finding supports previous literature highlighting both as viable graft choices.
Nevertheless, given the anatomical specifics of each graft, the choice to use either STG or BPB should include the lifestyle goals of the patient, for example, RTP vs. ADL or a wish to return to jumping or power/contact sports. Since BPB is associated with anterior knee morbidity, then perhaps contact sports or jumping/power athletes should consider STG as the better option. Likewise, given previous evidence suggesting that STG may not be as stable due to the lack of boney fixation, athletes engaged insubstantial pivoting and change of direction may want to consider BPB [15]. Nevertheless, these recommendations should be supported by further research. The authors recommend future studies to include a meta-analysis of STG and BPB articles specifically examining the exercises chosen during rehabilitation, timeline to sport-specific exercises, RTP timeline, failure rates, and future lifestyle goals of the patient post-rehabilitation. Concerning the current study, it appears the primary factor affecting recovery was meniscal repair in conjunction with ACLR. Therefore, clinicians should prepare the patient for a longer RTP process when accounting for concurrent ACLR and meniscal repair. Early intervention should focus on achieving ROM milestones that better prepare the patient to progress through the rehabilitation process.
This review study had several limitations. The researchers originally planned to conduct a full meta-analysis and review of specific rehabilitation exercises based on graft choice, but this goal was unattainable due to time constraints. In addition, the sample size (20 articles) was too small; future research should include a larger sample to support a meta-analysis. Lastly, a Risk of Bias assessment is recommended for future e meta-analysis projects to examine the potential for bias in the selection and analysis of publications.
This research was supported through an internal institutional grant.
The authors confirm their contribution to the paper as follows: Study conception and design: F. Davies, A. McDaniel; Data collection: F. Davies; Analysis and interpretation of results: F. Davis, A. McDaniel; Draft manuscript: F. Davies, A. McDaniel, L. Schroeder, A. Berni., D. Cobble.; All authors reviewed the results and approved the final version of the manuscript.