A sedentary lifestyle and physical inactivity affects more than half of the population worldwide. Despite the burdens that obesity and diabetes impose on our society, awareness of the cardiovascular disease as a result, is poor. What about primary prevention of cardiovascular diseases in our population with obesity and diabetes?
To investigate the feasibility in our daily practice of Cardiovascular (CV) primary prevention in Algerian patients without established cardiovascular disease.
A cohort of 517 patients mean age 58.9 ± 12.2 years, of them 318 women (61.5%), was enrolled in an observational prospective multicenter study in 2008. The global cardiovascular risk was assessed according both to the European Score chart low risk and to the risk chart from the European Society of Hypertension. Current situation of the knowledge of the healthy lifestyle was tested.
We have examined these patients within the setting of hypertension, diabetes, valvulopathies, dyspnea, noncardiac surgery cardiovascular assessment, and chest pain. No physical activity in the women. Cardiovascular risk assessment of this cohort showed that European Score low risk underestimates the risk as compared to ESH risk chart and this suggests to use preferably for our patients both European Score chart high risk and the risk chart from ESH.
Given the already increasing numbers of obesity diabetes and hypertension in our country, we should work together with the governments to decrease the aggressive marketing of high-calorie food and to support women for physical activity.
Obesity, Hypertension, Sedentarity, Physical activity, Primary prevention, Euroscore, Framingham score, Left ventricular hypertrophy
A sedentary lifestyle and physical inactivity affect more than half of the population worldwide. Despite the burdens that obesity and diabetes imposes on our society, awareness of the cardiovascular disease as a result, is poor. In Developed countries, public awareness campaigns focusing on these messages have improved outcome of their people. On the other hand, the loss of our culinary landmarks as traditional Mediterranean diet has resulted on an epidemic growth of overweight and obesity among our population. What about primary prevention of cardiovascular diseases in our population with obesity and diabetes?
To investigate the feasibility in our daily practice of Cardiovascular (CV) primary prevention based on the nutritional, physical activity and therapeutic education of Algerian patients without established cardiovascular disease after assessment of their global CV risk.
A cohort of 517 patients mean age 58.9 ± 12.2 years, of them 318 women (61.5%), was enrolled in an observational prospective multicenter study in 2008. Anthropometric indices, office blood pressure fasting blood glucose and lipid profile were evaluated. They all had Electrocardiogram (ECG) and echocardiography examination mainly to assess Left Ventricular Hypertrophy (LVH) and others structural anomalies. The patients were distributed in accordance with their risk factors associated with obesity and metabolic indexes. The global cardiovascular risk was assessed according both to the European Score chart low risk and to the risk chart from the European Society of Hypertension. Current situation of the knowledge of the healthy lifestyle was tested.
We have examined these patients within the setting of hypertension, diabetes, valvulopathies, dyspnea, non cardiac surgery cardiovascular assessment, and chest pain (Figure 1) smoking was found in 36.7% of the men and 1% of the women. Mean Body Mass Index (BMI) 30.3 ± 5.2 kg/m2. Mean waist circumference 104.6 ± 6 cm. Hypertension was found in 87.6% of our patients (pts). Diabetes mellitus in 59.3% of the pts with mean HbA1c 7.77 ± 1.89.
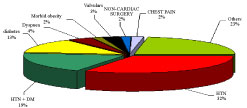 Figure 1: Reason for consultation.
View Figure 1
Figure 1: Reason for consultation.
View Figure 1
Regarding their risk factors, smoking was found in 36.7% of the men and 1% of the women. Mean body mass index (BMI) 30.3 ± 5.2 kg/m2. Mean waist circumference 104.6 ± 6 cm. Hypertension was found in 87.6% of our patients (pts). Diabetes mellitus in 59.3% of the pts with mean HbA1c 7.77 ± 1.89. Regarding dyslipidemia, LDL cholesterol was in the upper limit of the normal range whereas HDL cholesterol level0, 40 ± 0.08 g/l is in the lower limit and triglyceridemia level 1.63 g/l are high (Table 1).
Table 1: Clinical profile of our patients. View Table 1
Regarding their risk factors, 453 (87.6%) of the pts have hypertension, 307 (59.4%) have diabetes mellitus, association of hypertension and diabetes mellitus was found in 266 (51.4%) of the pts; association of hypertension diabetes mellitus and low HDL cholesterol in 37.5% of the pts (Figure 2). We found more left ventricular hypertrophy in echocardiography than in ECG (Figure 3). More than half of the diabetic's pts are on biguanides (Figure 4). Distribution of the antihypertensive, lipid-lowering and ant platelet treatments (Figure 5). Half of the patients are illiterate or have a primary level of education with a low socio-economic level (Figure 6). Their knowledge of nutrition and physical activities is low in third of the patients and in two third they have the knowledge but they can't practice any physical activities regarding socioeconomic status (Figure 7). Dietary habits of our patients concern mainly carbohydrates, saturated fatty acid in contrast with our old habits with olive oil. Consumption of sugar added in coffee and milk is too high.
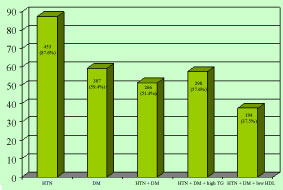 Figure 2: Distribution of the patients in accordance to their risk factors.
View Figure 2
Figure 2: Distribution of the patients in accordance to their risk factors.
View Figure 2
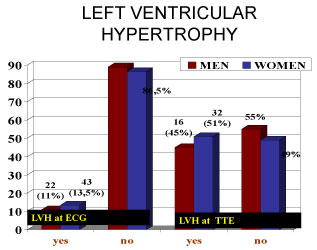 Figure 3: Comparison between LVH on ECG and LVH on echocardiography.
View Figure 3
Figure 3: Comparison between LVH on ECG and LVH on echocardiography.
View Figure 3
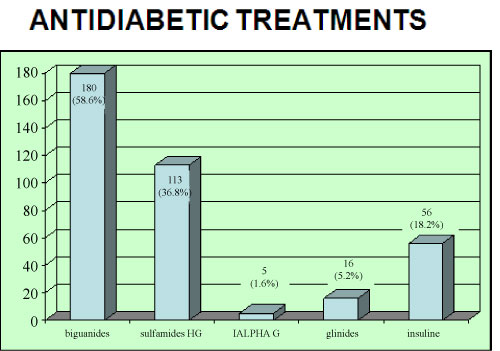 Figure 4: Antidiabetic treatment.
View Figure 4
Figure 4: Antidiabetic treatment.
View Figure 4
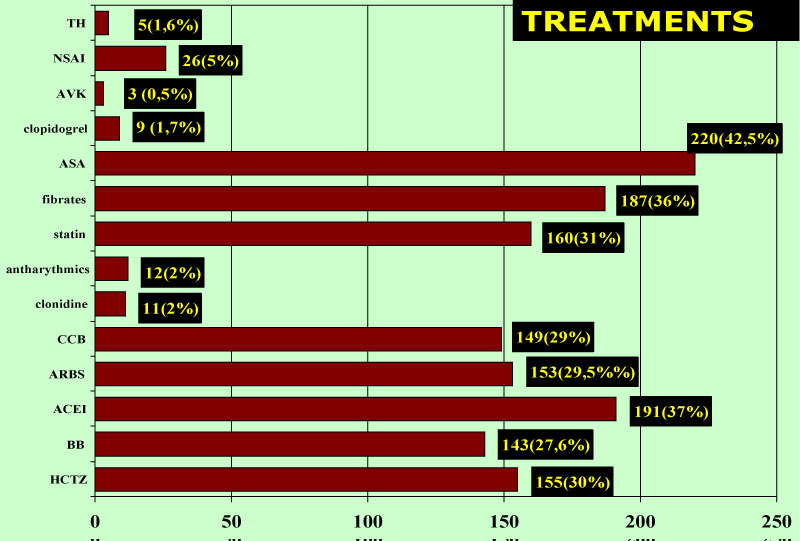 Figure 5: Antihypertensive treatment.
View Figure 5
Figure 5: Antihypertensive treatment.
View Figure 5
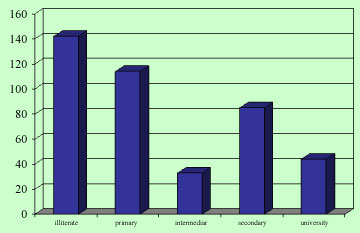 Figure 6: Level of education.
View Figure 6
Figure 6: Level of education.
View Figure 6
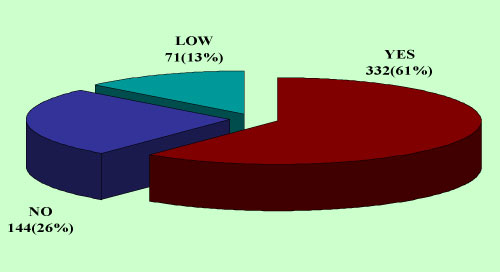 Figure 7: Knowledge of lifestyle recommendations.
View Figure 1
Figure 7: Knowledge of lifestyle recommendations.
View Figure 1
Cardiovascular risk assessment of this cohort showed that European Score low risk underestimates the risk as compared to ESH risk chart and this suggests to use preferably for our patients both European Score chart high risk and the risk chart from ESH (Figure 8).
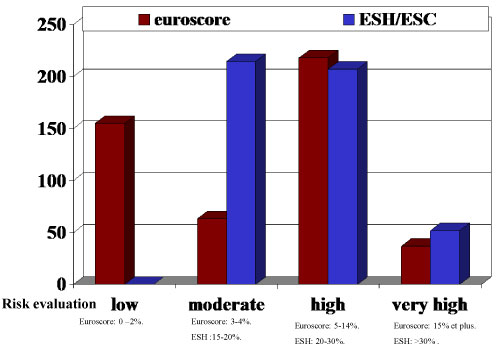 Figure 8: Cardiovascular risk assessment on ESH score and ESC score.
View Figure 8
Figure 8: Cardiovascular risk assessment on ESH score and ESC score.
View Figure 8
More than half of the patients are obese, diabetics and hypertensive and one third of them have low HDL cholesterol levels and high level of triglyceridemia. Cardiovascular risk assessment of this cohort showed that European Score low risk underestimate the risk as compared to ESH risk chart and this suggests to use preferably for our patients both European Score chart high risk and the risk chart from ESH [1]. Association of obesity, diabetes and hypertension is found in more than half of the patients and are associated with an increased risk of cardiovascular disease death and all-cause mortality [2]. We encourage them to achieve at least a reduction of weight to improve the cardiovascular profile as recommended in the recent guidelines of prevention. In our day unit we encourage our patients to walk every day at least 30 minutes and household work in accord with the recent European Guidelines on cardiovascular prevention [2]: Sedentary subjects should be encouraged to start light intensity aerobic physical activity (50-63%) HR max and then to moderate intensity as gardening. If we observe the new guidelines on cardiovascular disease prevention in clinical practice [2], Algeria is amongvery-high-risk countries and present levels of risk that are more than double that of low-risk countries (CVD mortality > 450/100, 000 for men and > 350/100, 000 for women). Additionally, the male: Female ratio is smaller than in low-risk countries, suggesting a major problem for women. The very high-risk countries are Albania, Algeria, Armenia, Azerbaijan, Belarus, Bulgaria, Egypt, Georgia, Kazakhstan, Kyrgyzstan, Latvia, Former Yugoslav Republic of Macedonia, Moldova, Russian Federation, Syrian Arab Republic, Tajikistan, Turkmenistan, Ukraine and Uzbekistan. In high-income regions Age-adjusted Coronary Artery Disease (CAD) mortality has declined since the 1980s, particularly. Coronary arterial disease rates are now less than half what they were in the early 1980s in many countries in Europe, due to preventive measures including the success of smoking legislation [3]. In our country the law on smoking has been activated but concerning the physical activity it is not only to establish legislation but to change attitudes at all levels especially towards women's sports and to give them a safe environment [4]. the 6th Joint Task Force guidelines [2] provide tools for healthcare professionals to promote population-based strategies and integrate these into national or regional prevention frameworks and to translate these in locally delivered healthcare services, in line with the recommendations of the World Health Organization (WHO) global status report on non-communicable diseases 2010 [5] Our challenge now in Algeria is to apply the key words of physical activity of the new guidelines of cardiovascular prevention [2]: Regular physical activity is recommended for all men and women as a lifelong part of lifestyle, with at least 150 min/week of moderate activity or at least 75 min/week of vigorous activity or an equivalent combination thereof. Any activity is better than none and more activity is better than some. Early childhood education in PA and movement should start at preschool/kindergarten. Daily physical activity at school should be at least 30 minutes, and preferably 60 minutes. Good neighborhoods and a safe environment enhance and encourage physical activity in everyday life. Regular PA reduces the risk of many adverse health outcomes over a wide age range: all-cause and CVD mortality are reduced in healthy individuals by 20-30% [6-8]. Physical activity has a positive effect on many risk factors, including hypertension, Low-Density Lipoprotein Cholesterol (LDL-C) and non-HDL-C, body weight and type 2 DM [5]. This applies to both men and women and across a broad range of ages from childhood to the very elderly. A sedentary lifestyle is one of the major risk factors for CVD independent of participation in physical activity [9].
Although the European scales of risk such as euroscore and European society of hypertension or the American scales of risk such Framingham is of a very big help for the stratification of the risk in primary prevention of our patients, and are a great education tool for our students, we have to adapt them to our population. For example the lipid profile of our often obese patients contains raised triglycerides level and reduced HDL cholesterol rather than raised LDL-C levels. Another factor is to prepare guidelines in the spoken languages by our patients in order to increase their compliance to the physical activity mainly. Education and support programme to encourage physical activity and quality nutrition is extremely important to reduce morbidity and mortality due to inadequate monitoring of cardiovascular risk factors. Given the already increasing numbers of obesity diabetes and hypertension in our country, we should work together with the governments to decrease the aggressive marketing of high-calorie food and to support women for physical activity.
I have nothing to declare.
Acknowledgement to the team of the day unit cardiology A1.