Futsal has become an important form of "campus football". It can provide important supports to sustainable development of "campus football" by studying injuries futsal players. In this study, the injured position and causes of futsal players were analyzed through questionnaire survey, comparison and literature review. It concludes that ankle is the most vulnerable position of futsal players to injuries, followed by waist, knee joint, head and face, hip and thigh successively. Waist is the most vulnerable position of goalkeeper, followed by hand, head and face, ankle and shoulder successively. Unreasonable body contact, inaccurate technical movement and poor physical strength preparation are main causes of injuries, which have some similarities and differences with causes of injuries in standard football games. Finally, different prevention measures were proposed to different injury positions.
Futsal, Undergraduates, Sport injury, Prevention
With increasing popularization of the futsal in China, it is appreciated more and more by teenagers. In particular, futsal which is characteristics of low requirements on playground, low competition cost and strong interesting becomes very popular in all kinds of schools as a response to the strong implementation of China's policy of "campus football". However, some violent actions, such as sprinting, sudden stop, turning, turn-back, jump and changing speed, in a relatively small space often may cause some injuries to athletes. How injuries occur during futsal? Is there any difference of injuries with those in standard football games? How to prevent them? These problems have been hardly discussed. Existing associated studies mainly focus on injury mechanism of athletes in standard football games. Hence, it is necessary to further study injury positions and causes in futsal to provide references for sustainable development of "campus football".
Undergraduate athletes and coaches from Hubei University, China Three Gorges University, Shanghai University of Engineering Science, Beijing Sport University and Guangzhou Sport University which are engaged in training and competition of futsal were chosen as the research objects. Injury positions and relevant causes in futsal were analyzed.
Questionnaire survey: A Questionnaire for Injuries of Undergraduate Futsal Players was formulated with reference to relevant studies. It was sent to 78 futsal players from Hubei University, China Three Gorges University, Shanghai University of Engineering Science, Beijing Sport University and Guangzhou Sport University. The average age of these 78 research objects was 22.32 years old and the average number of years in futsal training was 3. Among them, there were 53 level-1 or higher players (Table 1), 25 level-2 players. Besides, there were 12 goalkeepers and 66 players at other positions (there's no evident positions for futsal players). A total of 84 questionnaires were sent and 81 were collected. Besides, there were 3 invalid questionnaires and 78 valid questionnaires.
Table 1: Basic statistics of futsal players. View Table 1
Interview and diagnosis: Interviews to coaches and athletes about injury positions and causes were carried out. Meanwhile, sports medicine specialists were invited to for diagnosis of injuries (including, the extent of the injury, the disposal method, and the reventive measures).
Comparison: Causes of injuries to futsal players were compared with reported injuries of standard football players to distinguish the injury mechanism.
Futsal belongs to a whole-body contact sport of technical confrontation. Due to small site and strong confrontation, players are asked to accomplish technical movements at a high speed while changing body positions. Muscle injuries are easy to occur upon any poor preparation of technical actions or affecting by external forces. Ankle is the most vulnerable position. There are 37 cases of ankle injury, accounting for 47.4%. Waist injury ranks the second position and there are 27 cases, accounting for 34.6%. Knee joint is in the third position of injury and there are 20 cases, which accounts for 25.6%. The following positions of injury are head and face (20.5%), feet (16.7%), hip and thigh (12.8%), hand (10.3%), back (9.0%), neck (7.7%), leg (6.4%), shoulder (2.6%), chest and arm (1.3%). The most vulnerable position of goalkeeper is waist, which reports 6 cases (50%). Hand is the second injury position, which reports 4 cases (33%). Head and face and ankle are the third injury positions, which have 2 cases respectively (17%). Moreover, injuries are observed in shoulder, back, feet, hip and thing (Figure 1).
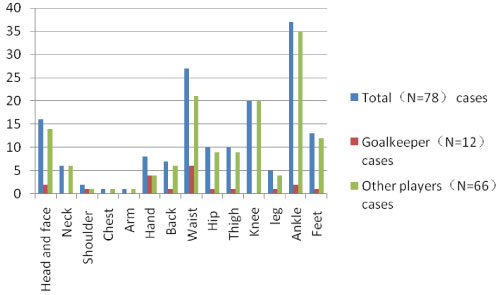 Figure 1: Injury positions of futsal players (N = 78). View Figure 1
Figure 1: Injury positions of futsal players (N = 78). View Figure 1
Wei Ming has investigated injury positions of standard football players and he concluded that ankle, tibia, musculus gastrocnemium and knee joint were vulnerable positions to injuries [1]. Lee, et al. found that lower limbs are the most common injury position of professional football players. Specifically, ankle injury, thigh injury and leg injury were top three injuries [2]. In a word, ankle and knee joint are the most vulnerable positions of futsal and standard football players to injuries, which are related with same technical principles.
Ankle: Ankle is one of the most important joints in movement of human body. It bears weight of the whole body. Due to anatomical biomechanical characteristics (poor stability, few muscles in the lateral ligament and weak muscle protection), ankle is easy to be injured due to impact and unreasonable technical actions [1].
Among 78 futsal players, there are 37 cases of ankle injury (47.4%), the highest compared with other injury positions. External ligamentous injury and traumatic osteoarthritis at ankle are two main injuries of goalkeeper. On the contrary, other players are easy to suffer external ligamentous injury and internal ligamentous injury of ankle (Table 2).
Table 2: Statistics of ankle injuries of futsal players. View Table 2
Futsal players have to make sudden stops, change direction and turn body while jumping by using surrounding ligamentous power. The feet stop, while leg and knee joint move forward continuously for inertia. As a result, ligament at fibula side is stretched excessively. Three external ligaments are independent and without protection by muscles and fats, and muscles are stretched excessively. Finally, players suffer external ligamentous injury of ankle.
The incidence of internal ligamentous injury of ankle is explained as follows. In sudden accelerating movement, players move one leg firstly, so that the internal ligament of the other ankle is stretched excessively. The front and back capsula articularis of ankle without protection by muscles and fats are relatively slack, while internal ligament of ankle is relatively tight, thus inducing internal ligamentous injury.
Obviously, futsal players get hurt for excessive bending and stretching of ankle by vibration at shooting, body impact and stretching at feet moving. This is generally consistent with ankle injury in standard football games.
Waist: Waist is the main action position of human body and it serves as the connection between upper and lower bodies. Waist bears great loads throughout the training and competition. Due to long-term high-strength uneven loads in training and competition, waist muscles and ligaments of players undertake uneven stresses. Players are easy to have waist injuries together by long-distance stretching. According to survey and statistics (Figure 1), waist injury account for 34.6%, only next to ankle injuries. Lumbar muscle strain and acute lumbar muscle sprain are dominant waist injuries (Table 3). Other players are suffering more serious lumbar muscle strain than goalkeeper.
Table 3: Statistics of waist injuries of futsal players. View Table 3
Lumbar muscle strain is a chronic waist injury. Due to long-term training under heavy loads, waist muscles undergo high-strength static contraction to generate fatigue injuries. In addition to sports training, athletes also may have lumbar muscle strain for long-term inaccurate sitting posture in daily life.
Acute lumbar muscle sprain ranks the second in waist injuries. Compared with the chronic lumbar muscle strain, acute lumbar muscle sprain is a sudden injury. In sports activities, acute lumbar muscle sprain is caused by inappropriate preparation for confrontation with external stress. For instance, players may overestimate external stress and make waist muscles in strong contraction, or they may underestimate external stress and fails to contract waist muscle fibers properly. Players may turn and sag with enough preparations and thereby suffer waist injuries upon slight external impacts [2].
Compared with standard football games, Futsal requires a smaller site, fewer players, and quicker attacking paces. Hence, the whole team consumes physical strength quickly and easy to feel fatigue. Futsal players are more vulnerable to lumbar muscle strain than standard football players. However, standard football players make more actions of tackling in air and produce violent body confrontations. According to data in Types of Sports Injuries in Beijing College Football League.
There are 5% waist and abdominal injuries in futsal players. Among them, 77.5% are acute injuries and 22.5% are chronic injuries. Obviously, there's a large proportion of waist and abdominal injuries in futsal players, most of which are lumbar muscles strain. On the contrary, waist and abdominal injuries in the standard football game are mainly acute lumbar muscle sprain [3].
Knee joint: Knee joint is often kept slightly bending to maintain gravity of body in futsal game. Therefore, knee joint bears very large loads in one competition, which is easy to cause knee injuries [4]. Knee meniscus injury is the dominant knee injuries, followed by tibiofibular collateral ligament injury, soft tissue contusion and patella cartilage fracture at knee joint
The proportion of knee meniscus injury in knee injuries of 78 futsal players is the highest (Table 4), which reports 2 and 17 cases (16.7% and 22.7%) in goalkeeper and other players. Since futsal players make violent outward or inward rotations of legs when they are running with balls, turning or stopping suddenly, the meniscus may make paradoxical movement (twist or inward or outward turning of knees while bending). Moreover, futsal site has hard floors which provide poor vibration buffering effect. All of these factors lead to knee meniscus injury.
Table 4: Statistics of knee joint injuries of futsal players. View Table 4
There are five cases of tibiofibular collateral ligament rupture and shin collateral ligament rupture in futsal players, ranking the second position (Table 4). Internal and external collateral ligamentous injuries of futsal players are caused by technical actions such as sudden stopping, changing direction and surpassing in competition or training. Compared with sudden stopping, bending angle of knee joint at fast surpassing is smaller, accompanied with larger counterforce of ground, smaller anteversion of tibia, higher myoelectricity of musculus gastrocnemius. As a result, knee stretching torque is increased during fast surpassing. These differences in biomechanical parameters of lower limbs between surpassing and sudden stopping also imply the greater possibility of knee injury at turning and surpassing [5].
Futsal is a crazy and high-speed sport. Futsal players are kept highly nervous in more time compared with standard football games. Futsal game requires continuous movement, short-distance sprint, transverse movement and frequency changing of direction. Means of passing, shooting, catching, dribbling, tackling and heading are 22.8, 5.2, 23.1, 17.9, 8.5, 15.9 and 0.6 (times) in a futsal competition, but they are 13, 1.5, 11, 19.7, 5, 6.9 and 3 (times) in a standard football competition [6]. Obviously, futsal requires significantly more passing, shooting, catching, interception and tackling than standard football game, but fewer dribbling and heading. The incidence of knee injury of futsal players is higher than that of standard football players due to the frequent contact with the football with feet.
Head and face: The proportion of head and face injuries in futsal players is 20.5%. Head and face are the fourth position which is easy to be injured in futsal games. Head and face injuries are mainly caused by following two reasons: firstly, players dribble the football in air and goalkeeper catches the ball. During dribbling, players of two teams have to fight for the advantageous positions and make high-strength body confrontation, so they are easy to have head and face injuries. In this process, trapezius is stretched excessively due to excessive head shaking, which may induce muscle strain and cervical vertebra injury. Players may swing arms for inertia during heading. They may hit head of the other players with a fist or elbow joint, causing slight concussion of brain and even fracture of nasal bone or teeth injuries. Due to short and quick shooting action, goalkeeper may be unable to make correct judgment on movement direction of the football when there are many players in front of the gate. Hence, goalkeeper may have concussion of brain or face scratches caused by football attacking. Secondly, head and face injuries are caused by impacts of football. In a futsal competition, the football is moved, passed and shot quickly. However, players have limited space for movement, and it is evitable for quickly moving football to attack head and face, causing fracture of nasal bone, teeth injury or face scratches (Table 5).
Table 5: Statistics of head injuries of futsal players. View Table 5
"Futsal" competition witnesses fewer heading techniques, because the narrow and small gate is easy to hold, but it is hard to attack. This differs significantly from that in the "standard football" game (P < 0.01) [7]. This is mainly because the playground for standard football game is large and players often makes technical actions combining heads, such as dribbling, corner kicking and heading. Therefore, standard football players are easier to have head and face injuries than futsal players.
Legs and feet: Feet injuries are common in futsal games. In this study, there are 13 leg and feet injuries, which account for 16.7% and rank in the fifth position (Figure 1). Specially, toe joint injuries and strephexopodia are the dominant leg and feet injuries, which report 10 cases including goalkeeper (Table 6). As a trochoid, toe joint often bends and stretches. Football players generally are trained since childhood. Vibration and impact force accumulated by kicking for more than 10 years of training may cause great injuries to toe joint of the primary touching point. Moreover, stamping and collision in competition both will cause certain damages to toe joint and even cause strephexopodia.
Table 6: Statistics of leg and feet injuries of futsal players. View Table 6
Strain of musculus gastrocnemius, fracture of bones of foot and soft tissue contusion at feet are secondary feet injuries (Table 6). Musculus gastrocnemius injuries at legs can be divided into positive and passive injuries. Passive injuries refer musculus gastrocnemius injury and even fracture of tibia and fibula caused by sliding tackle at lefts. Additionally, leg muscles of players are moving all the time throughout the high-strength training and competition. Running, defense and changing directions all can stimulate legs greatly. These actions can cause fatigue of musculus gastrocnemium and decrease functions and physical strength. Finally, strain of musculus gastrocnemium occurs.
Hip and thigh: Futsal players often suffer hip and thigh injuries. Groin muscle strain and biceps femoris muscle strain account for the highest proportion, followed by the quadriceps femoris strain (Table 7). Groin muscle strain is a common disease of football players, because groin is an important part that connects abdomen and thigh. Pectineal muscle, breviductor, adductor longus muscle, gracilis and adductor magnus are main muscle groups in groin which contract hip joint. These muscle groups are for adduction or outward extending of thigh. In football game, muscle groups in hip are stretched or contracted at quick starting, sudden changing of direction and violent shooting. Consequently, adductors or tendons in thigh are stretched or torn excessively, which further groin strain.
Table 7: Statistics of hip and thigh injuries of futsal players. View Table 7
Quadriceps femoris covers rectus, medial vastus muscle, vastus lateralis muscle and vastus intermedius. Rectus starts from anterior inferior spine and upper edge of acetabulum, while the rest three muscles start from shaft of femur [8]. Quadriceps which has a large physiological cross section are the strongest muscle in human body and they mainly serve for knee stretching. Rectus is a double-joint muscle that can stretch knee and bend hip [9]. Hip joint of futsal players is bended suddenly at sprint, which can trigger strain of quadriceps femoris at anterior inferior spine. Fracture of Quadriceps femoris is mainly caused by the semi-bending position of knee joint and sudden contraction.
Hip and leg injuries occur in the same position of futsal and standard football players. However, there's still some difference. Futsal site uses indoor suspending floors which have greater frictional force than outdoor natural grassland in standard football games. Besides, players often have scratches at outer side of gluteus maximus for sliding tackle, which occurs less in standard football games. Excessive impact between human body and ground at touchdown is often a major cause of lower limb injuries [10].
Hand: In this study, metacarpophalangeal contusion accounts for the highest proportion of hand injuries. Goalkeeper suffers hand injuries more than other players (Table 8). Goalkeeper in futsal competition is the player who contacts with the football by hand mostly. Due to the high speed and strong impact of shooting, goalkeeper who mainly plays with upper limbs often bears strong impacts at fingers. It may cause lateral or torsional violence by wrong catching actions, which further causes excessive inward and outward extension or rotation of palms and finger joint. As a result, collateral ligaments and capsular ligamentous injuries, or even dislocation and avulsion fracture are produced. Moreover, goalkeepers also may suffer fracture of wrist or elbow joint due to improper landing buffering from instable gravity of body in air or may suffer acromioclavicular dislocation upon lateral landing onto the hard floor.
Table 8: Statistics of hand injuries of futsal football players. View Table 8
Other players mainly suffer wrist joint injury, ulnar flexor tenosynovitis of wrist, metacarpophalangeal joint injuries and acromioclavicular dislocation for loss of gravity in dribbling and landing by hands.
1. Ankle is the most vulnerable position of futsal players. Waist injury ranks the second position. Knee joint is in the third position of injury. The following positions of injury are head and face, feet, hip and thigh, hand, back, neck, leg, shoulder, chest and arm. The most vulnerable position of goalkeeper is waist. Hand is the second injury position. Head and face and ankle are the third injury positions. Moreover, injuries are observed in shoulder, back, feet, hip and thing. But ankle injury, thigh injury and minor leg injury ranked the first three in standard football games.
2. Ankle is one of the most important joints in movement of human body due to anatomical biomechanical characteristics, inculding external ligamentous injury, internal ligamentous injury traumatic osteoarthritis at ankle, subluxation of ankle Ankle fracture. The main reasons are the vibration of feet touching the ball, the collision of players' body against each other, and the drag when the feet move. This is generally consistent with ankle injury in standard football games.
3. Waist injury is next to ankle injuries. Lumbar muscle strain and acute lumbar muscle sprain are dominant waist injuries. Other players are suffering more serious lumbar muscle strain than goalkeeper. Waist injury of futsal player was mainly caused by lumbar muscle strain, while Waist injury of player in standard football was mainly caused by acute lumbar sprain.
4. Knee meniscus injury is the dominant knee injuries, followed by tibiofibular collateral ligament injury, soft tissue contusion and patella cartilage fracture at knee joint. Because the times of passing, shooting, catching, breaking and blocking the ball in futsal is obviously higher than that in standard football, the knee joint injury rate of futsal is higher than that of standard football.
5. Head and face are the fourth position which is easy to be injured in futsal games. Head and face injuries are mainly caused by following two reasons, one is the players fighting for the high ball, and the other is the impact of the ball. The head technique is used less often and there are fewer head and face injuries than in standard football.
6. Feet injuries are common in futsal games including the strain of musculus gastrocnemius, rupture of the Achilles tendon, fracture of tibia and fibula, toe joint injuries and strephexopodia, fracture of bones of foot, soft tissue contusion at feet. this is no different from the standard football player.
7. Futsal players often suffer hip and thigh injuries. Groin muscle strain and biceps femoris muscle strain account for the highest proportion, followed by the quadriceps femoris strain. Futsal players are more likely to get hip and thigh injured than the standard players because they must make decisions to shoot, change direction and pass in a short period of time.
8. Goalkeeper suffers hand injuries more than other players, Other players mainly suffer wrist joint injury, ulnar flexor tenosynovitis of wrist, metacarpophalangeal joint injuries and acromioclavicular dislocation for loss of gravity in dribbling and landing by hands.
(1) Futsal players shall make enough warm-up exercises during competition and training to increase muscle temperature and lower viscosity. This has important significance to improve performance and reduce injuries. Muscle strain is easy to occur in winter and special attentions shall be paid to preparation activities [11].
(2) Since there are only few muscles and fats to protect ankle, the ankle can be wrapped with bandage or intramuscular paste before the competition to strengthen stability and decrease incidence of ankle injuries. Intramuscular paste with different techniques and strikes can improve joint activity, anti-inflammation and assisted rehabilitation significantly [12].
(3) Strength training of ankle and surrounding muscles shall be performed, such as heel lifting training, acrotarsium stretching/bending training, ankle abduction training and ankle adduction training.
(4) Please choose shoes appropriate for your feet.
(1) It is suggested to correct wrong body postures and do not keep one body position for a long time to avoid static fatigue injuries [13].
(2) Make full preparation before training and competition. Protective clothing is needed to old waist injuries to prevent secondary injury.
(3) Muscle training of abdominal and back. Abdominal and back muscles, such as rectus abdominis and erector spinae, shall be trained more to prevent waist injuries and waist strength shall be improved [14].
(1) Knee joint shall be prepared fully by strengthening joint activity, improving muscle temperature and lower muscle viscosity. These preparation activities can protect muscles surrounding knee joint better.
(2) Players are recommended to wear protective devices. Players with knee joint injuries can use kneecap and muscle paste.
(3) Stability of knee joint shall be trained. Muscles surrounding knee joint, such as biceps femoris muscle, quadriceps femoris and musculus gastrocnemius, shall be trained more.
(4) Coaches and players with knee joint injuries are recommended to hospital as early as possible. Surgical treatment shall be performed as soon as possible if necessary, to assure sports life of athletes [15].
(1) It is suggested make full preparations to neck muscles. Head and neck are hardly used in futsal game. Therefore, players often neglect warm-up of head and neck positions, which are main causes of cervical muscle strain.
(2) Players with cerebral concussion caused by impact at dribbling shall leave the game to prevent secondary injury.
(1) Players shall take full rest one day before the competition. The futsal site is small, but there are high passing density as well as more contacts with balls, frequency change between attacking and defense. These will consume physical strength of athletes and require athletes to take full rest to keep a good state during the competition. Full warm-up exercises of legs before competition can increase muscle temperature, decrease viscosity. They are of important significance to improve performance and reduce injuries [16].
(2) Appropriate physical strength training is needed. Futsal has characteristics of small site, fierce competition, strong body confrontation, high strength and great energy consumption. This requires athletes to keep full physical strength. Physical training is essential, which is a kind of protection to legs and feet [16].
(1) It is suggested to increase strength training, such as full squat training and step walking training. Muscle strength surrounding joints determines the incidence of sports injuries. For example, knee joint functions are closely related with strength of quadriceps femoris [17].
(2) During training and competition, muscle strain, such as groin strain, shall leave the game and received ice compress. Players can massage with voltaren or seek acupuncture therapy from professional psyciotherapy room after 24h.
(3) Warm-up exercises and stretching exercises of lower limbs are needed before the competition to increase muscle temperature and lower viscosity. These have important significance to improve performance and reduce injuries [18].
(1) Goalkeepers shall adopt a series of hand protection measures and put on gloves [19].
(2) Players shall have a buffering by using inertia to prevent hand injuries at landing.