Tools applied today in the Functional Training (FT) have long been used in general fitness programs, but systematic use and scientific interest are recent phenomena. Thus, there are many methodological conflicts and divergences in the prescriptions of this method [1]. For example, some studies have associated FT with the use of instability in many exercises [2,3], while others use unstable bases in a small portion of training [4,5] or simply do not use [6,7]. Thus, there is still an absence of a systematic FT model in the studies available in the literature [1], and for this reason the objective of this editorial was to suggest a functional training protocol that can be tested and applied safely, as well as being effective in increasing performance in daily activities. The information in this manuscript can help guide a therapeutic approach capable of contributing effectively to the treatment of physical disabilities in older people.
In older people, a FT program should focus on improving physical function-related conditioning abilities. Therefore, the perfect manipulation of all the variables necessary to prescribe training combined with the selection of specific exercises is essential, in order to minimize adaptive competition (neuromuscular and/or metabolic) and maximize performance in daily activities. Moreover, when thought to promote multisystem adaptations in senile, it should be composed of multicomponent, multiplanar and multi-joint exercises, combined with acceleration, reduction and stabilization movements, performed at maximum concentric speed in movement patterns similar to those performed in daily activities [7].
The structure of the session in circuit form is essential to reduce fatigue and increase exercise variability. The circuits should consist of 5-10 stations, with strength and muscle power exercises for the main muscle actions, alternating the body segments. For each exercise, a range of 12-15 repetitions using moderate loads (approximately 40-60% of a maximum repetition) is suggested, progressing to 08-12 repetitions with heavier loads (approximately 75-85% of a maximum repetition) [8].
The elderly should be instructed to move quickly from one exercise to another (15-30 seconds of transition between stations), being advised to complete 2-3 passes in the circuit. However, this relationship between execution and rest, named as training density, should be handled from several factors, such as: Level of physical fitness, training phase, presence of pathologies and goals.
Training loads should progress according to the elderly ability and comfort level, and it is recommended to use specific exertion perception scales such as OMNI-GSE [9], which is used to control the overall training intensity, in which participants are instructed to choose a single score that will reflect their degree of fatigue during and after each training set, where zero represents no symptoms (very, very mild) and 10 represents maximum symptoms (very, very difficult).
The sessions should be divided into sets to adjust the intensity and volume for each component of physical fitness to be stimulated (Figure 1), namely: (1) 5 min of mobility for the main joints involved in daily activity (ankle, hip and glenohumeral) and general warm-up exercises that include ten repetitions of squats and jumps; (2) 10-15 min of intermittent activities organized in circuit that should require mainly agility, coordination and muscle power (OMNI: 6-7); (3) 16-24 min of multi-joint exercises for lower and upper limbs, and with intense recruitment of spinal stabilizer muscles, also organized in a circuit (OMNI: 7-8); and (4) 5 min of intermittent activities (OMNI: 8-9) [7].
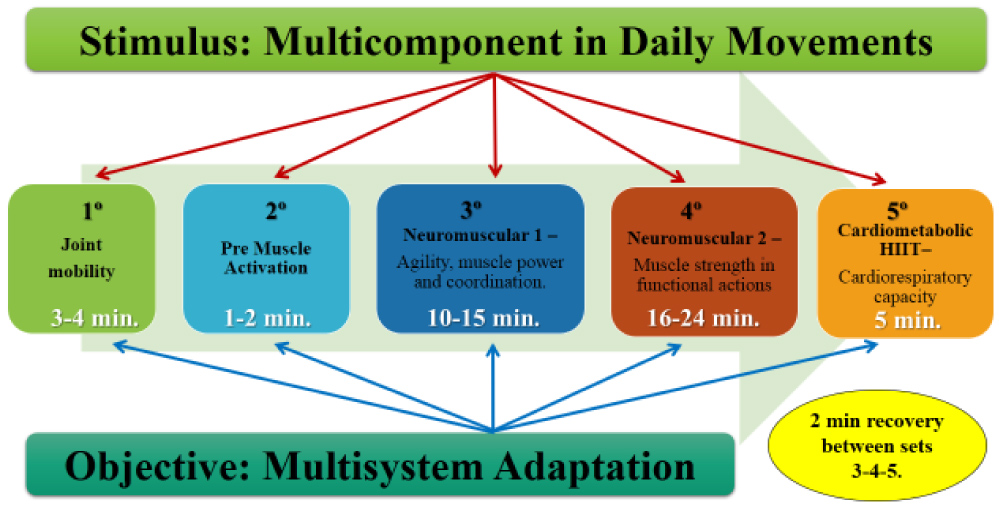 Figure 1: Proposals for structuring functional training for older people.
View Figure 1
Figure 1: Proposals for structuring functional training for older people.
View Figure 1
Next, we present an intervention model with particularities not yet popularized in the current literature:
The purpose of this exercise set is to prepare the musculoskeletal system for the stressful activities that will follow, through significant increases in range of motion and body stability.
Mobility exercises should be applied with emphasis on the main joints related to the functionality of the elderly, with 1-2 sets of eight seconds per exercise and 3-5 exercises per joint, in a total time of 3-4 min. Joint rotation movements are especially requested and are intended to increase the ability to perform movements at large joint amplitudes due to reduced joint stiffness, increased muscle temperature and decreased muscle spindle firing rate [10].
From a practical point of view, after performing mobility activities, muscle pre-activation exercises should be applied, with 1-2 sets of 12-20 repetitions on squats and jumps. The purpose is to improve body stability, provide muscle post-activation, stimulate the central nervous system and prevent injury [11].
The aim of the present set is to optimize muscle activation, improve inter and intramuscular coordination, proprioception, balance, agility and cognition, through activities in circuit, which will primarily require muscle power in a set of complex motor systems [12,13].
The exercises should require a combination of acceleration, reduction, stabilization, force production and manipulation movements, always being performed at maximum concentric speed, with a motor complexity that can be performed by elderly. There should be a gradual progression, starting with two passages in the first weeks to three passages during the final phase of the program [7].
The stimulus/pause ratio (density) is suggested to start at a 1:1 ratio (e.g. 30 seconds of stimulation/30 seconds of pause) and to progress to 3:1 at the end of the program (45/15). Intensity should be progressive 5-7 on a perceived exertion scale or 40-60% reserve heart rate [8].
Following are suggestions for intensity progression and stimulus variation in five main activities:
From the 1st-12th session, horizontal throws should be made at the wall at maximum concentric speed. From the 13th-24th session, vertical throws should be performed as high as possible.
1st-12th session should be performed linear hazing. From the 13th-24th session lateral movements or jumps must be performed.
1st-12th session the step up and down activity should be performed. From the 13th-24th session, vertical jumps should be performed.
From the 1st-12th session, linear movements should be performed (entering and leaving the stairs). From the 13th-24th session lateral movements or jumps must be performed.
Alternate linear movements must be performed with stabilization of the shoulder girdle; every 12 sessions the length of the chord may be increased for intensity progression.
The purpose of this set is to develop strength, increase muscle mass and bone mineral density, reduce body fat, improve body stability and motor efficiency for daily activities through multi-joint exercise, which require intense activation of stabilizing muscles of the spine also performed in circuit form for lower and upper limbs, alternating these body segments [13].
The movements should be similar to the daily activities of the elderly, applying a combination of essential actions such as pulling, pushing, carrying objects, crouching and lifting, always performed at maximum concentric speed, with an executable motor complexity and following a gradual progression, starting with two passages in the first weeks to reach three passages during the final phase of the program [7].
Intensity in this set can be controlled by an effort and progressive scale (70-85% of a maximum repetition) by adding external load to the possible exercises (e.g. front kettlebell squats). In those performed with their own body weight (example: Pulling on suspended tape), modifications should be made according to the elderly's ability and comfort level, to maintain 08-12 submaximal repetitions, respecting a 1-2 second cadence in the phase concentric and 3-4 seconds in the eccentric. The loads should be increased with a self-reported grade 6 (easy) on the OMINI-GSE scale and/or with the number of repetitions performed until voluntary fatigue or inability to sustain quality of exercise, i.e. if the participant performs more than the maximum number of pre-set repetitions (> 12), a 5-15% increase in external load should be performed immediately at the next session [7].
Training density should start from 1/1 and progress to 3/1 at the end of the program. Following are suggestions for progression of intensity and variation of stimuli in eight main exercises:
From the 1st-12th session, the exercise should be performed with an external load of 12-16 kg. From the 13th-24th session, with 16-20 kg.
Four lines should be marked parallel to the hanging tape offset, with a distance of 20 centimeters (cm) between them. The overload will be given with the highest inclination of the body during the sessions.
1st-12th session, exercise should be performed with one's own body weight. From the 13th-24th session, holding at chest height an average external load of 5-10 kg.
From the 1st-12th session, the exercise should be performed on a 60 cm bench. From the 13th-24th session, on a 40 cm bench.
From the 1st-12th session, the exercise should be performed with an external load of 8-12 kg. From 13th-24th to the session, with an external load of 12-16 kg.
Three lines should be demarcated parallel to the fixing point of the elastics, with the first line at a distance of 40 cm and between the others a distance of 20 cm. The overload will be given with the participant positioning in the most distant lines of the fixation point, causing greater tension in the elastic.
From the 1st-12th session, exercise should be performed with one's own body weight. From the 13th-24th session, a pedestal (10-15 cm) should be added to support the feet, increasing the range of motion.
From the 1st-12th session, the exercise should be performed by resting your elbows on a 40 cm bench. From the 13th-24th session, it should be performed leaning on a pedestal (10-15 cm).
The aim of this set is to increase VO2max and the ability of skeletal muscle to resynthesize ATP by oxidative metabolism through intermittent high-intensity exercise [14] and cognitive stimuli in dual-task activities [15].
The elderly, following a gradual progression, should use collective activities with executable motor complexity. Density should start at a 1:2 ratio and progress to 2:1 at the end of the program. It is recommended not to exceed 30 seconds of stimulation, with an intensity equivalent to 8-9 on an effort perception scale [9] or 80-90% of reserve heart rate.
Following is a description of three activities that can meet these requirements:
Within 30 meters, groups of five participants should be separated. For each group, three participants formed a column behind a cone and the other two formed another column at a distance of 20 meters. The working time consisted of traveling this distance at top speed and recovery is taking place while other group members are sprinting. Total volume should be progressive 8-12 sprints per participant.
Using rope-training equipment, participants will be divided into two groups, distributed at the ends of the rope. Activity begins with the groups pulling the rope at full strength. This action of muscle strength will be used how work time. To achieve maximum effort within the estimated time, two coaches positioned in the middle of the rope are required to equalize forces between groups. The total volume is 4-8 10-second of efforts with 20 seconds of recovery.
In this activity, the density is controlled by music bpm - high intensity (150-165 bpm) and low intensity (130-145 bpm). Rhythmic movements of executable complexity should be used, with slight displacements in the recovery phase and quick jumps or movements in the effort phase. The total volume should be five min.
It is noteworthy that the recommendations presented must be adapted to the physical conditions of each individual and are an update of the proposal of Functional Training for Older People, published by Resende-Neto, et al. [7], was elaborated according to the concepts presented by Stenger, et al. [16] and previously tested by Resende-Neto, et al. [17].