To investigate and summarise the available literature on the effectiveness of acupuncture stimulation on enhancing muscle strength in humans.
A systematic literature search was performed on electronic databases from inception to 2020. The risk of bias was assessed by two reviewers (SB and BL). The PEDro scale was used to assess the methodological quality of the RCTs and the standards for reporting interventions in clinical trials of acupuncture (STRICTA) was used to assess the quality of the acupuncture intervention. This systematic review is reported according to the PRISMA guidelines.
A total of 27 RCTs were retrieved from our search and following further assessment 20 RCTs covering 737 participants met the inclusion criteria. The overall score on the PEDro scale for risk of bias was moderate-high with five studies scoring low. A meta-analysis was not possible due to the incomparability of the study characteristics such as outcome measures, treatment intervention, patient population and the methodological rigour. Seventeen studies compared the effects of acupuncture with a control group. Twelve (71%) of the studies found that acupuncture was significantly more effective than the control group in enhancing muscle strength. Twelve studies compared the effects of acupuncture with a sham acupuncture group. Seven (58%) found that acupuncture was significantly more effective that sham acupuncture and 5 (42%) of the studies found no significant difference between the acupuncture and the sham intervention on enhancing muscle strength.
The overall finding indicates that there is strong evidence that acupuncture is more effective than control and there is some evidence that acupuncture is more effective than sham acupuncture in the enhancement of muscle strength. Further studies are required with a clear evidence-based justification for the choice of acupuncture and sham points and the use of the STRICTA in the enhancement of muscle strength.
Acupuncture is a clinical intervention that is becoming more popular in sports medicine and exercise rehabilitation [1]. A number of studies have shown acupuncture to be effective at reducing spasticity [2] and enhancing muscle strength [3] following stroke. A systematic review was undertaken by Bailey [4] to investigate the effectiveness of acupuncture in enhancing human performance and to evaluate the methodological quality of the investigating Randomised Controlled Trials (RCTs). Eleven RCTs covering 321 participants met the inclusion criteria. Four studies [5-8] assessed the effects of acupuncture in enhancing muscle strength in the lower limbs. The results from the four studies investigating the effects of acupuncture on muscle strength were conflicting. The studies by Hubscher, et al. [6] and Hubscher, et al. [9] presented negative (insignificant) results and the studies by Huang, et al. [7] and So, et al. [8] presented positive results. Three of the studies were of a high methodological quality with one study scoring low. Since the last systematic review in 2012 [4], there have been several additional RCTs that have assessed the effect of acupuncture on enhancing muscle strength in humans. The author is not aware of any recent systematic reviews or meta-analysis that have assessed the effect of acupuncture on muscle strength in humans. It is important that the quality of available RCTs and the acupuncture intervention be thoroughly assessed to determine whether acupuncture is a valuable treatment to enhance muscle strength during rehabilitation or to enhance sports performance. The aim of this study is to investigate and summarise the available literature on the effectiveness of acupuncture point stimulation compared with sham acupuncture and control on enhancing muscle strength in humans.
This review is reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [10].
A systematic literature search was performed by SB and BL on the following databases from their inception to 2021: MEDLINE, Embase, SPORT Discus, CINAHL, AMED, ProQuest nursing journal, PubMed, ScienceDirect, the Cochrane Central Register of Controlled Trials, PEDro, Google Scholar, specialized registry of the Cochrane Musculoskeletal group and the Cochrane field of Physical and Related Therapies. The keyword search was: Acupuncture, auricular acupuncture, laser acupuncture, TENS/electro-acupuncture or acupoint, which were combined with: ‘Muscle’ and‘Strength’. The bibliographies and references of published studies and reviews were scanned for other possible RCTs. The reviewers (SB and BL) determined the studies to be included based upon the inclusion and exclusion criteria. The titles and abstracts of each study were screened. If any of the studies met the inclusion criteria, the full text was obtained and reviewed by both reviewers. The two reviewers would then meet to discuss and mutually agree on any differences.
To be included in this review, a study had to meet the following criteria: RCTs that have used acupuncture to enhance muscle strength in humans; no language restrictions were imposed, and translations were sought where necessary; published and unpublished reports of completed randomised controlled trials, in English or translated into English were included. Papers were excluded that were not original descriptions of a clinical study on humans, that described a single case, or where the points used are not recognised as classic acupuncture points.
The risk of bias was assessed by two reviewers (SB and BL). The PEDro scale [11] was used to assess the methodological quality of the RCTs and the standards for reporting interventions in clinical trials of acupuncture (STRICTA) [12] were used to assess the quality of the acupuncture intervention.
A total of 27 RCTs were retrieved from our search and following further assessment 20 RCTs covering 737 participants met the inclusion criteria. A PRISMA (Preferred Reporting Items for Systematic Reviews and Meta- Analyses) flow diagram is shown in Figure 1.
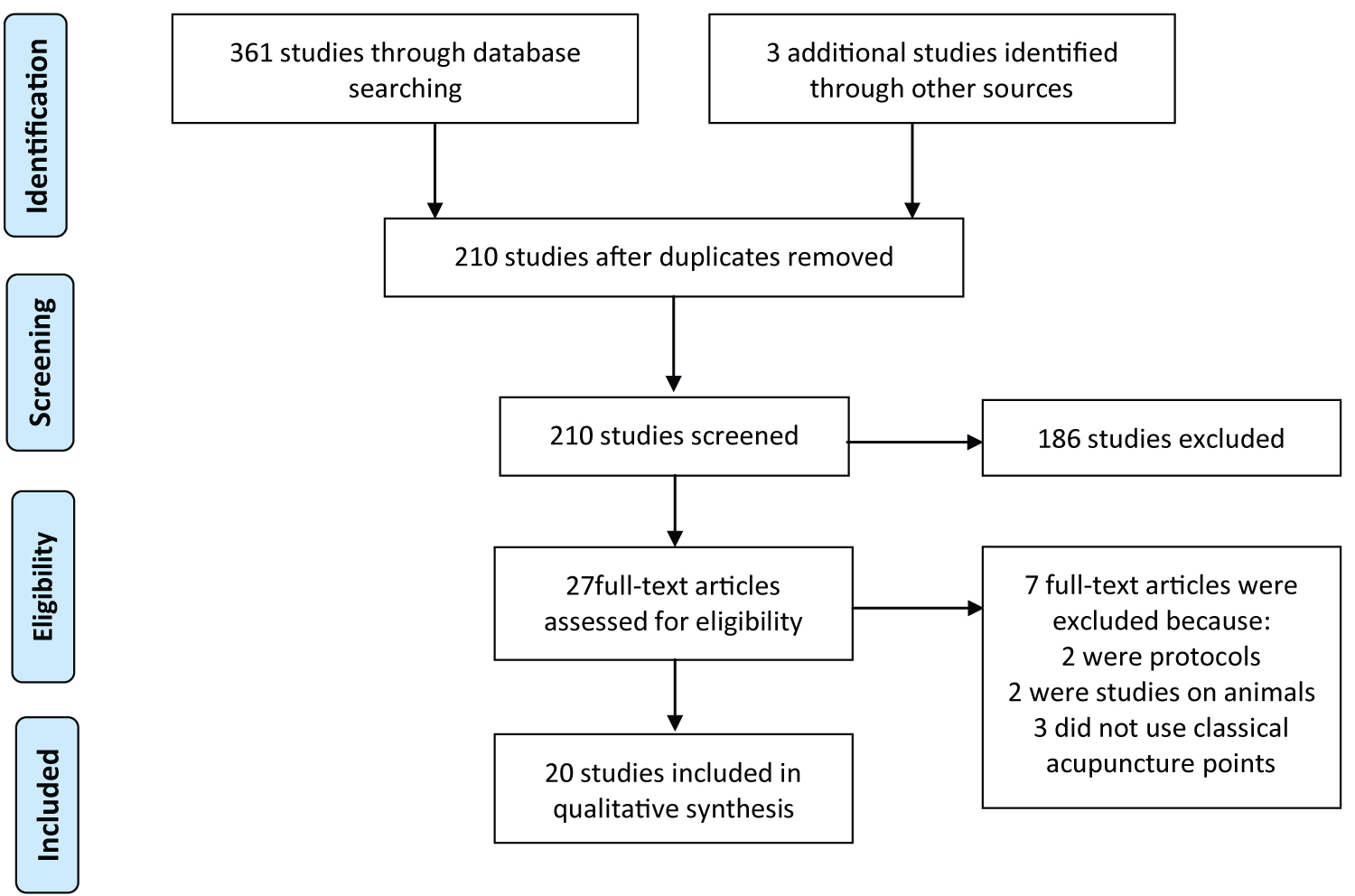 Figure 1: A PRISMA flow diagram of study selection.
View Figure 1
Figure 1: A PRISMA flow diagram of study selection.
View Figure 1
The basic characteristics of the RCTs assessed in this review are presented in Table 1. The studies were published between 2006 and 2021 and included 737 participants aged between 17 and 85-years-old. The sample size ranged between 17 and 73 participants. Fourteen (70%) studies [5,6,13-22] had 30 or more participants, thirteen (65%) studies [6,14-16,18-25] applied a single treatment session and seven (35%) studies [1,3,5,7,8,13,17] applied several treatments over 2 days to 8 weeks. There were at least 162 female and 267 male participants reported to take part in the trials. Six (30%) studies [1,3,14,17,19,24] did not report on gender or indicate the ratio of female to male participants. Seventeen (85%) studies used healthy subjects, one study [16] used healthy and post-stroke patients, another study used post-stroke patients [3] and one study [17] used patients suffering with sarcopenia. Eight (40%) studies [1,3,7,15-17,21,24] compared the effects of acupuncture with a control group, nine (45%) studies [5,6,9,13,14,18-20,23] compared the effects of acupuncture with a control and a sham acupuncture group, and three study [8,22,25] evaluated the effect of acupuncture with a sham group on muscle strength.
Table 1: Characteristics of the studies that assessed the effects of acupuncture on enhancing muscle strength. View Table 1
The overall score on the PEDro scale for risk of bias was moderate-high (Figure 1) with five studies scoring low [8,20-22,25]. The main drawback in these studies were blinding of participants, therapists and assessors. Three studies [6,9,16] (15%) reported that the subjects were blinded to acupuncture; however, they did not use an assessment tool to determine the effectiveness of the blinding. Two studies [3,6] (10%) blinded the therapist and seven [3,5,6,9,17,19,21] (35%) blinded the assessor from subject allocation.
None of the RCTs assessed in this review used the STRICTA checklist as a guide. The main issues were the choice and justification of acupoints, frequency and number of treatment sessions. Generally, it was found that acupuncture was administered by a qualified healthcare professional with at least one year’s experience in the application of acupuncture. Two studies [14,18] chose acupuncture points based on their location and not necessarily on their ability to enhance muscle strength. Hubscher and colleagues [9] chose points based on the finding of an earlier study, which assessed the effects of acupuncture on delayed onset muscle soreness and not on muscle strength enhancement. Damasceno, et al. [17] analysed the effects of acupuncture tonification points; however, there was no supportive evidence on the effect of tonification points on enhancing muscle strength. Tough [20] chose points based on the segmental innervation and not necessarily on their known effects on enhancing muscle strength. The sham points that were chosen in this study coincide with the same segmental innervation as the true acupuncture points which may have impacted the treatment outcome.
Number and frequency of treatment sessions and delayed effect of acupuncture: 13 studies [6,8,14-16,18-25] used a single acupuncture treatment session and assessed the effects immediately following the withdrawal of the needles. Both human and animal studies have shown that the effects of acupunctures have a delayed onset, with a gradual peak, and a gradual return to baseline [26-28]. Price and colleagues [26] found that following electroacupuncture there was a delayed onset of between 1 and 24 hours to maximum effect, which persists 10-14 days following treatment. Our earlier review4 found that acupuncture was significantly more effective than sham acupuncture and the control group when assessed up to 72 hours after treatment, and not as effective when assessed immediately following treatment. Furthermore, it was found that acupuncture was most effective when several sessions over a number of weeks were employed [4]. Wang and colleagues [29] assessed the effect of acupuncture on the explosive forces generated by the male shoulder joint and found that the effect of acupuncture took approximately 10 minutes to appear. The current review found thirteen studies [6,14-16,18-25] that applied a single treatment of acupuncture and assessed the effect immediately following treatment. Eight of the thirteen studies [8,19,21,22] found that acupuncture was more effective than sham or control, and five studies [6,14-16,20] found no significant difference between groups. Seven studies [1,3,5,7,8,13,17] applied several treatments over 2 days to 8 weeks. Three studies [1,3,7] found a significant difference between groups in favour of acupuncture, two studies [9,17] found no significant difference between groups, and two studies [5,13] found a significant difference between the acupuncture group and control but no significant difference between the acupuncture and sham acupuncture group.
Sham acupuncture intervention: Most of the studies in this review used sham points that did not correspond with a meridian, acupuncture point, or extra points and were between 1 and 2 cm away from the points used in the intervention group. There are non-specific physiological effects of needling that may include local alteration in circulation and immune function [30] and trigger of neural pathways such as those resulting in diffuse noxious inhibitory control (DNIC) of pain [31]. White, et al. [32] stated that it is difficult to find a ‘wrong’ site that is credible to the patient but does not have some effect through segmental analgesia and that the difference between the effects of real and sham treatment could be very small.
It is suggested that the type of sham acupuncture that is chosen for a clinical controlled trial should depend on the research question [33,34] and the type of acupuncture treatment to be tested [33,35]. Birch [35] announced that a pilot study should be conducted to investigate the appropriateness of the non-acupuncture points when using non-acupoints as a sham treatment. If the control treatment is tested first in a pilot study, one can generate data about the relative effectiveness of the sham acupuncture treatment, which will assist in determining if indeed it is an appropriate sham treatment [36]. Another important issue with all sham treatments is to avoid the mislabelling of the sham treatment as a placebo treatment [37]. All of the sham interventions tested so far are thought to activate physiologic non-placebo non-specific effects and some activate specific effects [34,37,38]. In this review none of the studies pre-tested the sham acupuncture points. Two studies used sham EA and placed the electrodes over the nerve trunk/muscle belly [5,13] of the tibialis anterior. The location of the sham points corresponds with the deep peroneal nerve trunk. Neuromuscular electrical stimulation over the nerve trunk or muscle belly have been shown to have a central or a peripheral response to enhancing muscle strength [39-41]. Therefore, it was no surprise that there was no significant difference between the sham EA and EA to ST-36 and ST-39 in the studies by Zhou, et al. [5] and Huang, et al. [13]. Hence, the choice of a sham EA intervention in clinical trials needs to be considered carefully with regards to the placement of the electrodes or the needles when utilising sham electroacupuncture to enhance muscle strength.
Loss to follow-up: When undertaking a clinical controlled trial, plans should be made to minimise any loss of subjects to follow-up. This can be achieved through the implementation of a pilot study to identify and reduce risk factors that may lead to dropouts [36]. The study by Damasceno, et al. [17] started with 53 subjects but only 26 completed data collection. This is quite a high dropout rate which may have had a significant impact on the results.
A meta-analysis was not possible due to the incomparability or availability of the study characteristics such as data, outcome measures, treatment and intervention.
The overall result from the 17 studies that compared the effects of acupuncture with a control group showed that 12 (71%) of the studies found that acupuncture was significantly more effective than the control group in enhancing muscle strength. Twelve studies compared the effects of acupuncture with a sham acupuncture group. Seven (58%) studies found that acupuncture was significantly more effective than sham acupuncture and 5 (42%) studies found no significant difference between the acupuncture and the sham intervention on enhancing muscle strength.
The overall finding of this review is similar to our previous study [4] which indicates that further rigorous studies are required to determine whether acupuncture is an effective treatment modality to enhance muscle strength during rehabilitation and sports.
Three studies assessed the effect of acupuncture on elbow flexor muscle strength. Hubscher, et al. [9] investigated the effects of a standardised acupuncture treatment on muscle function of the elbow flexor in the dominant arm following the induction of delayed onset muscle soreness (DOMS) in 22 healthy subjects. They found no significant difference between groups for Maximum Isometric Voluntary Force (MIVF). Following the induction of DOMS, strength values decreased in all groups to nearly the same extent for 24 hours. However, after the first treatment both acupuncture and sham acupuncture appeared to maintain their strength throughout the rest of the experimental period, whereas, further decrease in strength occurred in the control group. Fragoso and Ferreira [16] evaluated the immediate effects of manual acupuncture on myoelectric activity and isometric force of the bicep brachii in 32 healthy and 15 post-stroke patients with chronic hemiparesis. They found no significant difference in EMG activity between LI-11 group and PC-2 (control) group. In contrast to the findings by Hubscher, et al. [9] and Fragoso and Ferreira [16] Zhou and colleagues found that a single 15-minute session of acupuncture significantly increased isokinetic angular muscle strength of the elbow flexors in 16 healthy female students compared to the sham acupuncture group.
Two studies [14,20] assessed the effect of acupuncture on muscle strength of the wrist flexor/extensors. Both studies analysed the EMG activity and strength responses of the flexor muscles of the wrist following stimulation of acupuncture points. They found no significant difference between groups.
Two RCTs assessed the effect of acupuncture on hand grip strength. Damasceno, et al. [17] analysed the effects of acupuncture tonification points of hand grip muscle strength and inflammatory markers of subjects aged over 60 years with sarcopenia. The overall findings of this study indicate that there was no significant difference between the acupuncture group and the other groups regarding the assessed variables (muscle mass, muscle strength, functionality, and inflammatory markers). Silverio-Lopes and da Monta [19] evaluated the immediate response to grip strength gain capacity after a single application of acupuncture in 73 healthy volunteers. They found that the acupuncture group had a significant strength gain, while the sham and the control groups showed no significant gain in handgrip strength.
De Souza, et al. [18] evaluated the effect of acupuncture stimulation of points along the Yang meridian (SI-8 and SI-14) on activation patterns and strength responses of the trapezius muscle. The participants were randomised into four groups; local group received acupuncture at SI-14; the distant group received acupuncture at SI-8; and the control group received acupuncture at the Ki-3. The fourth group was classified as the naïve control group and did not receive any acupuncture. Analyses of SI-14 and SI-8 showed a significant increase in the upper trapezius muscle strength at 20 minutes following acupuncture. The control and naïve control groups did not show any changes.
Six studies assessed the effect of acupuncture on enhancing strength in the rectus femoris muscle. So, et al. [8] evaluated the effects of Transcutaneous Electrical Acupuncture Stimulation (TEAS) on enhancing the rate of muscle force capacity recovery after strenuous knee extension/flexion exercise. A significant treatment effect for peak torque was recorded, indicating that the TEAS group recovered faster than the control group and this positive effect was further enhanced across treatment time. Micalos, et al. [24] observed the effect of acupuncture on peak isometric muscle torque of the knee extensor following fatigue. They found that the control group had a 6.4% loss in strength following fatigue; however, the acupuncture intervention group presented a 1.6% increase in muscle strength. Jang and So [23] investigated the effects of acupuncture on Maximal Voluntary Isometric Contraction (MVIC) and EMG activity of the rectus femoris and tibialis anterior muscles. Participants were randomly assigned to a real acupuncture, sham acupuncture, and control group. The results showed that the real acupuncture group had higher MVIC EMG activities in the rectus femoris and tibialis anterior muscles compared with the control group. Mucha and colleagues [21] assessed the effect of ST-36 acupoint on explosive strength in the lower limb. They found a significant increase in jump hight, speed and level of power in the ST-36 group and no change in the placebo (UB-60) group. Wang, et al. [29] compared the immediate effect of true acupuncture (ST-32, ST-34, ST-36, SP-10 and UB-57) with the effect of sham acupuncture (blunt tip needles) on explosive force production and stiffness of the knee joint. The average maximum torque, average work, average power, average peak power and total work of the true acupuncture group increased significantly after treatment, while there was no significant change in the sham acupuncture group. Hubscher, et al. [6] assessed the immediate efficacy of real acupuncture compared with sham acupuncture and placebo laser acupuncture on rectus femoris muscle strength in 33 recreational athletes. They found that a single treatment session of acupuncture was significantly more efficacious in increasing Maximal Isometric Voluntary Force (MIVF) of the knee extensors than placebo laser. After acupuncture, MIVF increased by 8%, but by only 5% after sham acupuncture and by 3% after placebo laser acupuncture. Although acupuncture was superior to sham acupuncture, the difference did not reach statistical significance.
Six studies assessed the effects of acupuncture on ankle dorsiflexion/plantarflexion muscle strength. Costa, et al. [15] compared the immediate effects of local and adjacent acupuncture at ST-36 and SP-9 on the tibialis anterior muscle EMG MIVF. They found a significant decrease in the root mean square values in both the ST-36 and SP-9 groups immediately following acupuncture. Huang, et al. [13] investigated whether unilateral MA at non-acupoints could result in bilateral ankle dorsiflexion strength gain similar to that found in EA at specific acupoints. Fifty healthy volunteers were randomly assigned to four groups: MA or EA at ST-36 and ST-39, or MA or EA at two non-acupuncture points. A fifth group acted as a control and received no treatment. All intervention groups increased in muscle strength; however, there was no significant difference in strength gain between the intervention groups. There was no significant change in the control group from baseline. A similar study was conducted in 2012 by Zhou and colleagues [5]. They also found no significant difference in strength gains between the intervention groups. It is important to note that in the studies by Zhou, et al. [5] and Huang, et al. [13] the sham acupuncture points were placed in the tibialis anterior muscle belly over the peroneal nerve trunk which have been shown that electric stimulation in this location would influence muscle strength gain [39-41]. In 2007 Huang and associates [7] applied EA to ST-36 and ST-39 to determine its effects on ankle dorsiflexion muscle strength in 30 healthy subjects. Their results demonstrated a significant increase in muscle strength in both the stimulated and non-stimulated limb (21.3% in the right and 15.2% in the left limb). Payton and Bailey [1] undertook a similar study to Zhou, et al. [5] and Huang, et al. [7,13] to determine whether six weeks of acupuncture had a positive effect on plantarflexion muscle strength and whether EA had a greater effect than MA. They found that both MA and EA had a significant effect in increasing plantarflexion strength with an average torque gain of 17% (right) and 8% (left) for manual acupuncture, 16% (right) and 25% (left) for EA, and 6% (right) and a reduction of 3% (left) for the control group. In 2009 Yan and Hui-Chan [3] investigated whether TENS applied to acupuncture points in patients after acute stroke decreases spasticity and/or increased muscle strength more effectively than placebo stimulation and standard rehabilitation in 62 post-stroke patients. They found that when compared with standard rehabilitation or placebo stimulation, TENS to acupuncture points significantly increased the percentage of patients with normal tone, increased ankle dorsiflexor strength, and decreased antagonist co-contraction ratio. Patients in the TENS acupuncture group also walked 2-4 days earlier than the patients in the other 2 groups.
There were a number of limitations within this review. There were significant variations in the study characteristics which prevented from pooling the data and conducting a meta-analysis to formulate a meaningful summary of the results. The needle placement of the sham-control groups and justification of points selected with regards to their effect on enhancing muscle strength was inadequate. Due to the lack of use of the STRICTA and poor justification of the chosen acupuncture points in the evaluated RCTs, it was difficult to draw an accurate conclusion on treatment outcome.
The authors declare that they have no conflict of interest and the authors have no financial interest related to the material of this manuscript.
The overall finding indicates that there is strong evidence that acupuncture is more effective than control and there is some evidence that acupuncture is more effective than sham acupuncture in the enhancement of muscle strength. Further studies are required with a clear evidence-based justification for the choice of acupuncture and sham points and the use of the STRICTA in the enhancement of muscle strength.