Tendinopathies especially that of the Achilles account for a significant amount of overuse injuries in sports that could hinder optimal performance in sport, might lead to permanent physical damage or disability, and it's epidemiology is not extensively documented in our clime. Therefore, this study aimed to determine the prevalence and risk factors associated with Achilles Tendinopathy (AT) among university soccer players.
A cross-sectional survey of 210 soccer players, where 79.5% of the participants were male purposively sampled from two universities. Data on selected anthropometric indices and socio-demographic characteristics of the participants was ascertained. Royal London Test and Victorian Institute of Sports Assessment-Achilles Questionnaire were used to assess AT. The inferential statistics of Spearman rank order correlation and chi square were used for data analysis at an alpha level of 0.05.
The prevalence of AT was 21.9 per 100 persons. The mean AT score, age, height, weight, and Body Mass Index (BMI) of the participants were 92.29 ± 15.89, 22.46 ± 1.47 years, 1.74 ± 0.13 meters, 68.90 ± 7.46 kg, 19.73 ± 1.80 respectively. Significant correlation exists between AT score and the following variables: age (p = 0.018), weight (p < 0.01), height (p < 0.01), BMI (p < 0.01). There was no significant correlation between sex and AT score (p = 0.215).
The prevalence of Achilles tendinopathy in university soccer players was high. Age, height, weight, BMI except sex correlated with AT. The results depicts that the higher the BMI, the likelihood of having AT.
Achilles tendon, Anthropometry, Prevalence, Soccer, Tendinopathy, University
BMI: Body Mass Index; AT: Achilles Tendinopathy; VISA-A: Victorian Institute of Sports Assessment-Achilles Questionnaire
Sports injuries have been found to inhibit optimal sports' performance and these injuries, which can have both long and short term harmful effects, causes lasting physical damage or disability [1], affect quality of life, thus could result in reduced physical activity participation. Every sport comes with risk of injury that is peculiar. The occurrence of sports injuries and its associated problems are on the increase [2]. In association football, commonly known as soccer, injuries have been identified to result from multiple risk factors and ankle injuries are one of the most common injuries [3]. Ankle injuries in soccer may give rise to problems like reduced performance, time away from competition and possibly disability [4]. The bones that make up the ankle joint are a regular site of injury and often times, bending and twisting forces can precipitate these injuries [5], with the most common being ankle sprain, fracture, and tendinopathy. Tendinopathy happens when the tendon is forced to endure high or peculiar load, presents as pain in the tendon and impaired performance sometimes accompanied by swelling [6].
Achilles tendinopathy is a clinical condition characterized by pain and swelling in and around the Achilles tendon, mainly arising from overuse [7]. It is often a result of increase in training load. The Achilles tendon is the strongest tendon in the body serving both the gastrocnemius and soleus muscles originating near the mid-calf and inserts posteriorly at the calcaneus [8]. Achilles tendinopathy commonly happens in the mid-substance of the tendon or less commonly at its insertion in the calcaneus [8]. Previous observational studies have proved that competitive athletes have a 24% lifetime incidence of Achilles tendinopathy [9]. One study in the Netherlands reported the annual occurrence of symptoms characteristic of Achilles tendinopathy in the general population as 2.01/1000 people [10]. There are certain risk factors associated or that makes one susceptible to Achilles tendinopathy. Identifying them is important in prevention and treatment of Achilles tendinopathy [11,12].
Soccer is widely recognized to be the world's most popular sport [13], and is played at different levels, worldwide, national, state, universities and even secondary schools. It is played by players in over 200 countries, making it the world's most popular sport [14]. Soccer involves several crafts that demand complex movements making the athletes susceptible to injuries, and tendinopathy is one of the most recorded overuse sports injuries in modern societies [15]. Participation in soccer is a worldwide event with tremendous health and economic benefits [16], increased self-esteem, peer socialization, general fitness, as well as reducing various diseases risks, crime rate and poverty [17]. A lot of attention has been given to elite soccer players while in university soccer players, there are higher numbers of participants who began playing early and continue for a longer period. For some of them, their gears are not always suitable for the sport, thereby increasing the threat of tendinopathy [9]. The average university soccer players play soccer at least three (3) times a week, and Achilles tendinopathy occurs as a result of overuse. The increase in the popularity of soccer and expectations from players make meaningful numbers of soccer injuries conceivable. University soccer players also go through rigorous physical training, preparing for inter-club competition, inter-school competition. They are not professionals, so much attention is not given to them, but the trainings and constant field activity also makes them susceptible to sports injuries like Achilles tendinopathy. Also, intrinsic factors inherent in individual's physiology could also influence susceptibility to Achilles tendinopathy [9]. Little or no thorough investigation or study on the occurrence of Achilles tendinopathy on this population has been carried out and we aimed to assess the prevalence as well as factors that would correlate with AT. Therefore, we hypothesized that AT will not be prevalent and also, that age, sex, weight, height, and body mass index would not correlate with AT in university soccer players.
Purposive sampling technique was used to recruit 210 participants from two selected universities in south east Nigeria for this cross-sectional study. Both male and female who have played soccer consistently for at least six (6) months were included and participants who actively engaged in other sports like basketball, sprinting were excluded because these sports could make them prone to Achilles tendinopathy.
Ethical approval was obtained from Ethical Committee of Faculty of Health Science and Technology, of one of the University. A letter of introduction from the Department of Medical Rehabilitation was given to the coaches of the various teams seeking for permission to carry out the research with their teams. Informed consent was obtained from all participants and assuring them of confidentiality of their information.
The Royal London test, a psychometrically sound instrument, was used for assessing Achilles tendinopathy [18,19]. To start the test, the participant lay prone on the plinth with the feet hanging outside the table. The ankle was in neutral position and the Achilles tendon was palpated for tenderness. The participant was asked to dorsiflex and the ankle was palpated on dorsiflexion. Results were classified as tenderness present on dorsiflexion or absent. In patients with Achilles tendinopathy, tenderness was felt on palpation with the ankle in neutral position, but on dorsiflexion tenderness was absent or reduced.
Each participant stood upright on a bathroom weighing scale (with calibration set at 0) with minimal clothing and barefooted. The height was measured with participants standing erect, backing the calibrated part of the stadiometer, and looking straight ahead with both arms by the side and read starting from the vertex of the head to the sole of the feet. After, the Victorian Institute of Sports Assessment-Achilles (VISA-A) questionnaire was administered; it is a valid, reliable, and user-friendly index of the severity of Achilles tendinopathy [20,21], which contains eight [8] questions that covers the 3 domains of pain (questions 1 to 3), function (questions 4 to 6), and activity (questions 7 and 8). Questions 1 to 7 are scored over 10, and question 8 carries a maximum of 30. Scores are summed to give a total of 100. An asymptomatic person would score 100. For question 8 which has three part (A, B, C), participants must answer only one part; A, B, or C that relates to the person's reality. If the participant experiences pain when performing sport, he or she automatically loses at least 10, and possibly 20, points.
Data collected was analyzed using SPSS version 20. Data set was assessed for normality using Kolmogorov-Smirnov and Shipiro-Wilk statistics and some were found not to be normally distributed (p < 0.05). Descriptive statistics was summarized using ranges, mean, standard deviation, percentages and frequency count. Inferential statistics was analyzed using Independent t-test, Pearson square and Spearman rank order test. Level of significance was set at 0.05. Prevalence was calculated using the formula for point prevalence;
A total of 210 soccer players, both male and female within 18 to 27 years of age participated in this study and only two participants were obese and these two have symptomatic Achilles tendinopathy as shown in the Table 1 and Figure 1. They were selected from four campuses of two universities with majority from University A (64.8%); of the 46 that tested positive to Achilles tendinopathy (21.4%), 45 were symptomatic as seen in Table 2.
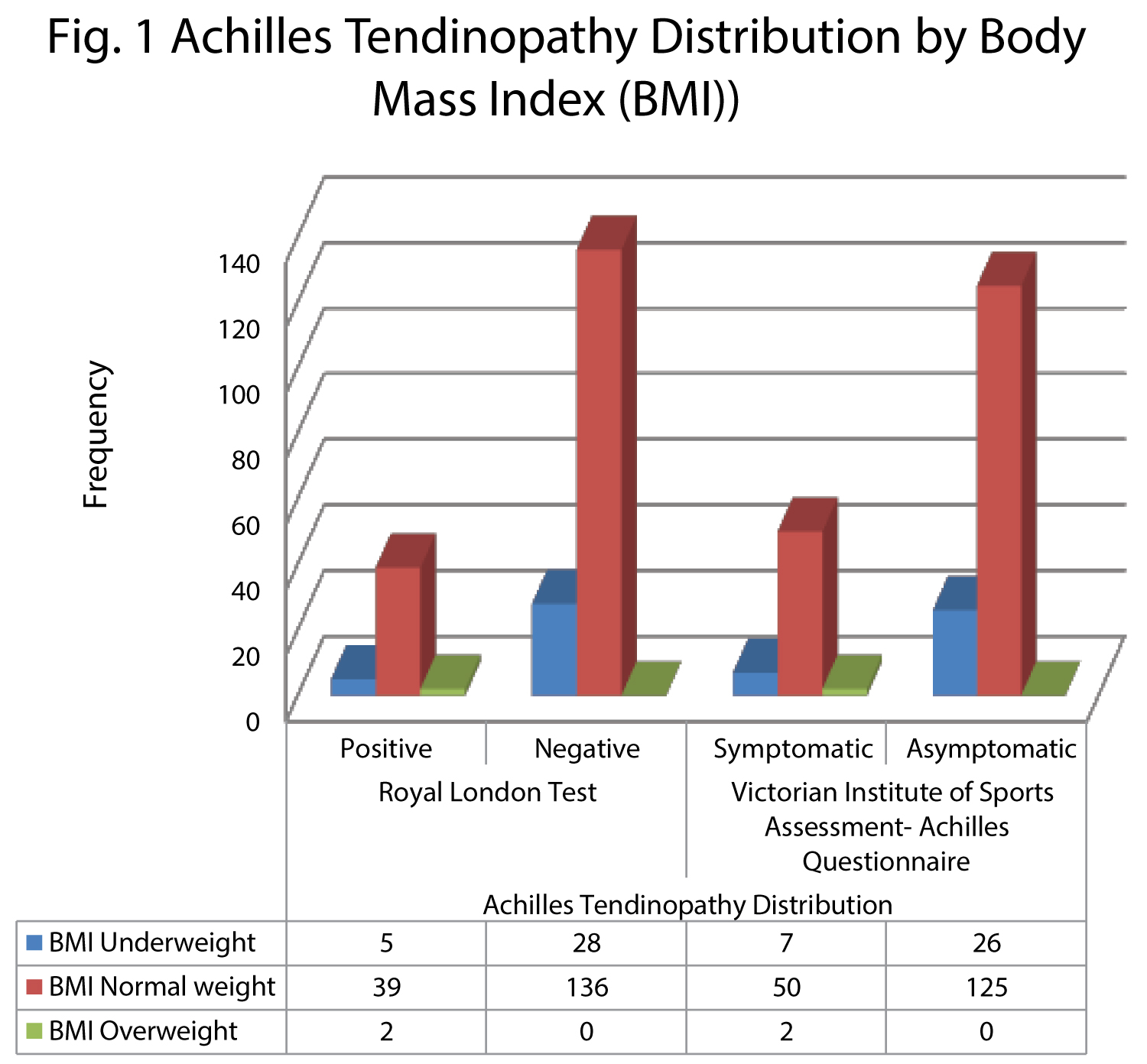 Figure 1: It is a graphic representation of the participants' Achilles tendinopathy score (positive and negative), and it's severity (symptomatic and asymptomatic AT) distribution by their BMI.
View Figure 1
Figure 1: It is a graphic representation of the participants' Achilles tendinopathy score (positive and negative), and it's severity (symptomatic and asymptomatic AT) distribution by their BMI.
View Figure 1
Table 1: Characteristics of University soccer players. View Table 1
Table 2: Geographical Characteristics, BMI and Achilles Tendinopathy Distribution of University Soccer Players. View Table 2
Prevalence = 0.219
Therefore, point prevalence of Achilles tendinopathy in university soccer players is 21.9 per 100 persons. Table 3 shows that Age, height, weight, and Body Mass Index significantly correlated with Achilles tendinopathy score (p < 0.05). There was no significant correlation between sex and AT score (p = 0.215 with an odd ratio of 1.942).
Table 3: Correlation Matrix of Age, Weight, Height, BMI with Achilles Tendinopathy Score. View Table 3
In this present study, the prevalence of Achilles tendinopathy in university soccer players is 21.9 per 100 persons. Aiyegbusi, et al. [9] reported a prevalence rate of 15.9 per 100 persons among local soccer players while a higher prevalence of 21.5% among Australian male professional football players was reported by Docking, et al. [22]. In the study by Obst, et al. [23] on recreational athletes in a Sub-Saharan African country, a much lower prevalence rate was recorded. The increased rate in this study maybe due to lack of attending medical team and Physiotherapist for this school teams or neglect by the school body. It may also be attributed to difference in sample population.
The participation rate for both sexes in university soccer has been evaluated with almost 80% dominance by males. This could be as a result of many factors which according to Joshua, et al. [24] in a study conducted in Ilorin includes cultural beliefs, parental influence, religion, peer-group, gender bias (women had been valued so much for their succulent, dedicated bodies and good looks which are assumed to be incompatible with the physical vigor, strength and force supposedly required for sport competitions). In this study, there exists no association between sex and Achilles tendinopathy; although the dataset used was not normally distributed. So, this may affect the generalisability of this result. Longo, et al. [25] previously found no link between sex and tendinopathy with a suggestion that any association between gender differences may simply be the result of differences in reporting of injuries or seeking care. Also van der Vlist, et al. [26] reported that there is conflicting evidence that sex affects the risk for AT; In his review, one cohort study reported that being female is associated with AT [27], while no association was demonstrated in two cohort studies [28,29].
A significant negative correlation between age and Achilles tendinopathy score was observed in this study. This result is in tandem with the finding by Franceschi, et al. [30], where a potential interaction between age and degenerative tendon changes was identified. This associative predisposition to Achilles tendinopathy as one age could be as a result of wears and tears attributed to age and decreased rate of repair as one ages. Surprisingly, these findings are in disagreement with the results of the study by Aiyegbusi, et al. [31], where no association was found between age and AT. This conflicting result could be as a result of the small sample size used in the latter study as the author concluded that a similar study of a larger study is needed for a generalized application.
Weight and BMI significantly correlated with Achilles tendinopathy. This results agrees with the findings of Frey and Zamora [32], which showed that a high BMI (both in overweight and in obese range) significantly increased the chances of Achilles tendinopathy, and this association is also echoed by the report of significant association between obesity and Achilles tendinopathy in the study by Franceschi, et al. Contrarily, the systematic review done by van der Vlist, et al. showed that BMI has no significant association in three cohort studies [33-35]. Also, Taunton, et al. [36] reported no statistically significant association between obesity and tendinopathy. The conflicting result could be as a result the nature of research of the later study as it was a retrospective case control analysis. Therefore, the researcher considers weight as a risk factor for Achilles tendinopathy from the observations made in the current study. The height of the participants significantly associated with Achilles tendinopathy and a cohort study [27] also, reported an increased height in patients with AT. To the best of the researcher's knowledge, there is limited evidence that height does not affect the risk for AT and the researcher concludes that height could be considered as a risk factor for AT.
The prevalence of Achilles tendinopathy in university soccer players was high. Age, height, weight, BMI except gender correlated with Achilles tendinopathy. The results depicted that the higher the BMI, the higher the likelihood of having AT; and of all the participants that were overweight, all had AT. Also, there may be need to encourage female active participation in soccer as the number recruited for this study is low due to reduced number of female turnout for soccer practice during the data collection phase of this study.
This research was funded by the authors.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
UMC and CMA conceived and designed the study while IUO and UNA make a substantial contribution in the implementation phase. All authors were involved in data collection, analysis and interpretation. All authors read and approved the final manuscript.
The authors have no conflict of interest to disclose.