Background: The injury rate for CrossFit training is relatively low in comparison to other fitness-related sports. Systematic reviews regarding the extent of number of injuries per body part and injury-related exercises in CrossFit training are scarce. The purpose of this study was to determine the injury prevalence and incidence in CrossFit participants, in particular of injured body parts, and to examine injury related exercises in CrossFit.
Methods: In December 2021 a comprehensive search in Embase, PubMed, Cinhal, and Sport Discus databases was conducted using keywords CrossFit, Weightlifting, gymnastics and injuries. Studies investigating injury incidence and prevalence in CrossFit training that specifically reported injured body parts, independently screened by two authors, were included. The NIH Quality assessment tool for observational cohort and cross-sectional studies was used to evaluate the methodological quality and validity of each study.
Results: Eighteen studies were included in this review. The injury prevalence was between 19.4 and 73.5%, the injury incidence between 12.8 and 66.2%. Shoulder injuries, accounting for between 6.7 and 40.6% of all injuries, were found as most common injury location among CrossFit participants. Lower back (12.9 to 36.0% of all injuries), hand/wrist (4.0 to 32.7%), knee (4.7 to 21.4%), elbow (2.0 to 17.9%), foot/ankle (3.0 to 10.2%), hip (1.6 to 13.3%) and neck (2.0 to 7.0%) injuries were less commonly reported. Most injuries were associated with weight lifting or power lifting movements. Lower back injuries occurred more in weight lifting and power lifting exercises. Shoulder injuries were associated with gymnastic exercises such as ring dips, ring muscle ups, and exercises containing kipping movements.
Conclusion: The injury prevalence and incidence in CrossFit participants was between 19.4 and 73.5% and 12.8 and 66.2, respectively. Shoulder injuries were the most common injured body part among CrossFit participants, followed by lower back and hand/wrist injuries. Gymnastic movements as kipping pull-ups, ring dips and muscle ups were reported as exercises with a higher risk for shoulder injuries. Lower back injuries were more commonly reported in association with weightlifting and power lifting movements such as back squat and dead lift.
CrossFit, Injury, Prevalence, Incidence, Gymnastics, Weightlifting
CrossFit is a relatively new and rapidly growing strength and conditioning sport, that defines its program as 'constantly varied, functional movement, performed at high intensity' [1]. Globally there are currently over 4 million participants estimated with over 15.000 affiliated CrossFit gyms [2,3]. The aim of the sport is to forge a broad, general, and inclusive fitness [1]. Research has shown that CrossFit training improves strength and endurance in heterogeneous populations [1,4-7]. CrossFit workouts incorporate a wide range of exercises, including aspects of gymnastics, power lifting, Olympic weightlifting and endurance. These aspects are combined in a daily program, called "Workout of the Day" (WOD). Each WOD can be scaled to allow participation regardless of strength and fitness levels [1].
Participation in CrossFit training has been criticized for having a potential disproportionate risk of musculoskeletal injuries [8,9]. Despite methodological limitations [10], recently published studies that investigated injuries in CrossFit training conclude that the injury rate is between 0.74 and 18.9 injuries per 1000 hours of CrossFit training [11-22]. Three prospective studies have reported injury rates between 2.1 to 18.9 injuries per 1000 hours of CrossFit training [13,23,24]. These rates are comparable or lower than injury rates in other sports like running, rugby, soccer, football and other exercise programs [9,25-39].
Over the last couple of years several studies regarding injuries associated with CrossFit participation and general risks and benefits have been published [12-15,17,20,21,24,40-45]. To date, several systematic reviews have investigated injuries associated with participation in CrossFit training [3,9,46-55]. Most reviews obtained to identify the injury incidence or prevalence of existing literature yet few investigated the injury prevalence or incidence in specific body parts. To expand and update contemporary CrossFit injury related literature, the primary purpose of this study was to review the injury incidence and prevalence in CrossFit trained participants, in particular of the injured body parts. The secondary purpose was to examine injury related exercises in CrossFit. Analyzing such characteristics can support strategies for injury prevention and can determine the focus of future CrossFit injury studies.
A search of the Embase, PubMed, Cinhal, and Sport Discus database was conducted on 13 December 2021 using the search strategy presented in Table 1. The search strategy was created by one of the authors, assisted by a biomedical information specialist. The studies found following the search in different databases were merged and duplicates were removed. The Preferred Reporting Items for Systematic Reviews and Meta-Analyse (PRISMA) was used for the schematic representation of the flowchart of the reviewing process [56].
Table 1: Search strategy. View Table 1
Title and abstract were screened, and full-text articles were read by two authors. If necessary, the third author was consulted to reach consensus. For inclusion, the following criteria were used: (1) injury proportions were reported over the total population and per injured body part, (2) full text article were written in English or Dutch, (3) participants were training at official registered CrossFit affiliates and (4) studies had a cohort, case-control, or cross-sectional study design.
In case no data regarding the number of injuries were reported or could not be calculated, the corresponding authors were contacted by email for additional data. Studies, from which injury prevalence and incidence per injured body part could not be derived, were excluded from this systematic review. Case studies and case series were excluded because of the relatively low level of evidence. Within t4.he search strategy and inclusion, no limit for publication data was used.
Two authors independently scored each included study for methodological quality using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [57]. Prior to the overall quality rating, questions in the assessment tool were prioritized with regard to the research question of this systematic review. Study design, timeframe sufficiency and adjustment for confounders in the statistical analysis were marked as essential points for the overall quality rating (poor, fair and good). The authors compared their assessment results and discussed discrepancies until a consensus was reached. If necessary, the third author was consulted to reach a consensus.
The data extraction was performed by the first author. Demographic data were summarized for each study. The primary variables were the total number of injured athletes, the total number of injuries and the number of injuries specified by anatomical location. If reported in a respective study, the number of injuries specified to associate exercises were summarized.
Depending on methods of data collection the injury incidence or prevalence was reported. The injury incidence was used for studies reporting new cases of injuries over a specific time period. If not reported, injury incidence was calculated as new cases divided by the total population. The injury prevalence, number of cases in a specific time period (point, period or life time), was calculated as the number of injured athletes divided by the total population. The injury registration period for each study is mentioned. Injuries per body part, per study, were summarized with three measures: (1) as actual reported number, (2) as injury prevalence or incidence depending on data collection of each study, and (3) as percentage of all reported injuries.
The literature search yielded a total of 757 studies. A flowchart of the studies that were identified, pre-screened, and selected for analysis are presented in Figure 1. Eighteen articles met the inclusion criteria and were included in this review [12,13,15-18,20-24,40-45,58]. The full overview of characteristics of included studies are included in the appendix. Fifteen out of eighteen included studies had a retrospective study design [12,15-18,20-22,40-45,58] and three studies had a prospective study design [13,23,24]. Sixteen studies [13,15-18,20,21,23,24,40-45,58] have included all body parts in the investigation of injuries, where as Summitt, et al. [22] examined the injury characteristics of only shoulder injuries and Tawfik, et al. only examined the hand and wrist injuries [42]. An overview of included studies and the injury characteristics are presented in Table 2 and Table 3.
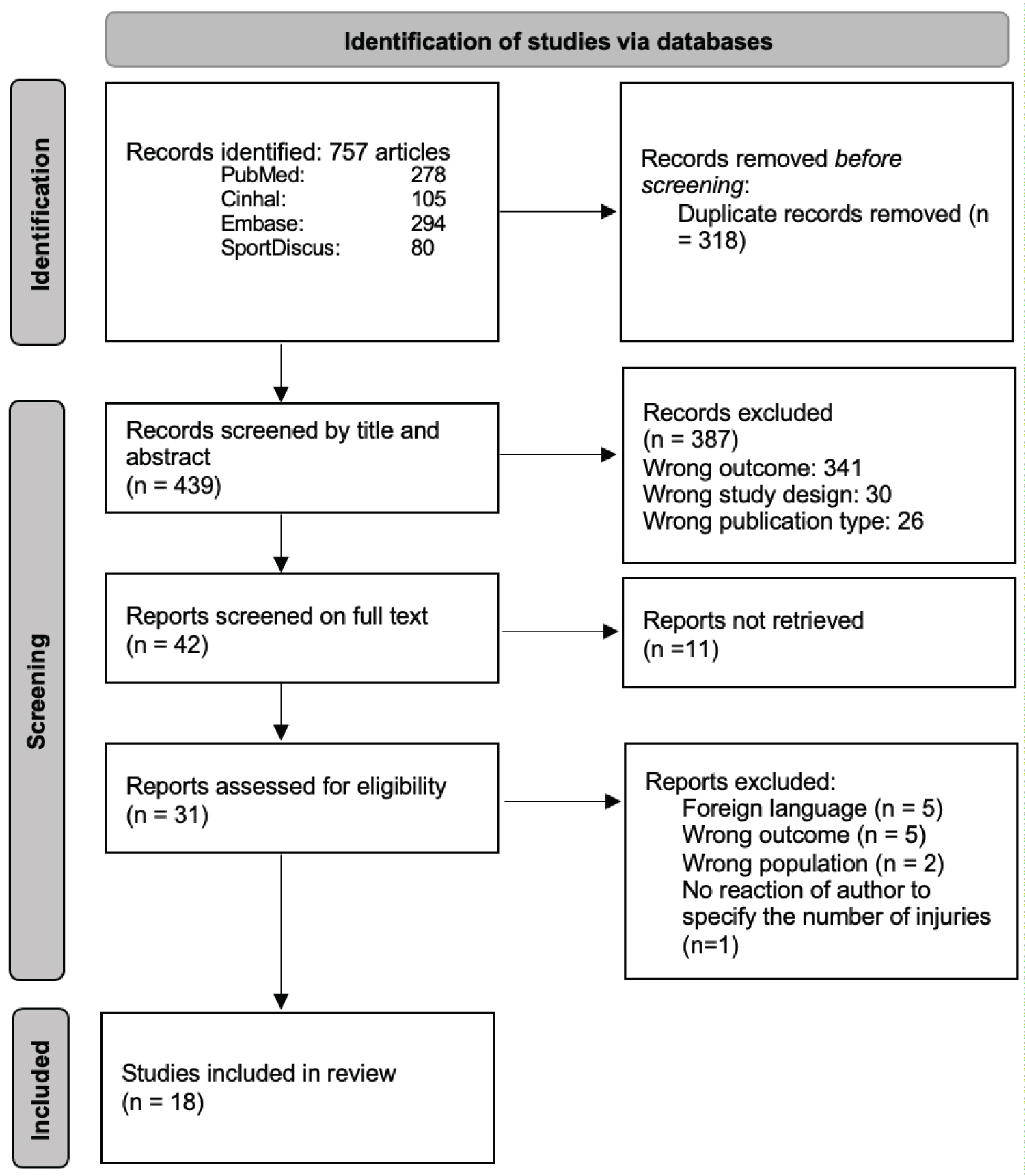 Figure 1: PRISMA flow diagram.
View Figure 1
Figure 1: PRISMA flow diagram.
View Figure 1
Table 2: Brief overview injury characteristics, injury prevalence/incidence. View Table 2
Table 3: Brief overview injury characteristics, injury prevalence/incidence (continue). View Table 3
The results of the quality assessment are presented in Table 4. Four studies have been assessed as 'good' quality. Six studies have been assessed as 'fair' and eight as 'poor' quality.
Table 4: Quality assessment. View Table 4
A total of 7,915 Cross Fit athletes (4,198 male, 3,524 female, 193 unknown gender) participated in the included studies, ranging from 54 to 3,049 athletes per study. The average age ranged from 17 to 69 years [12,13,15-18,20-24,40-45]. Fifteen studies described the level of experience in CrossFit training, which is shown in Table 1 (characteristics of the included studies) included in Appendix 1 [12,13,15-17,22,23,40-45,58].
Most studies used a 'time loss' definition of injury [12,13,15-17,22,23,42-45,59]. Seven studies used the same injury definition, referring the study of Weisenthal, et al. [12,15,16,22,42,43,45]. One study did not report an injury definition [40]. A summary of injury definitions used in the included studies is presented in Table 5.
Table 5: Injury definitions. View Table 5
The injury prevalence, reported in eleven retrospective studies, was between 19.4 and 73.5% [15-18,20-22,40,43-45]. Two studies reported injuries since the beginning of participation in CrossFit training [15,18], four studies over the prior twelve months [16,17,44,45], and four studies over the prior six months [20-22,43]. The injury registration period of one study was not reported [40].
The injury incidence, reported in three prospective studies and four retrospective studies, was between 12.8 and 66.2% [12,13,23,24,41,42,58]. Retrospectively, two studies reported a life time incidence [41,42], one study reported the incidence over the prior six months [12] and one study did not reported the time period. One prospective study had a follow up of eight weeks, and two studies performed a twelve week follow-up [13,23,24].
A total of 2,111 injuries have been reported among 4,182 participants in fourteen included studies [12,16,18,20-24,40,41,43,45,58].
A total of 553 shoulder injuries have been reported among included studies, representing between 6.7 and 40.6% of all injuries [12,13,16,18,20-24,40,41,43-45,58]. One study only reported shoulder injuries [22]. The lifetime prevalence for shoulder injuries was 36.4% in the study by Hak, et al. [18]. The prevalence over a six to twelve months period was 5.4 to 26.4% [16,20,21,22,43-45]. Three prospective studies reported a shoulder injury incidence between 0.9 and 11.5% [13,23,24]. Three retrospective studies reported an injury incidence for shoulder injuries between 16.7 and 36.9% [12,41,58]. One study did not reported the number of shoulder injuries in their study [42].
The lower back was with 452 injuries the second most reported injury location. Two studies did not reported the number of lower back injuries in their study [22,42]. Lower back injuries were accounting between 12.9 and 36.0% of all injuries reported in retrospective studies, and between 15.0 and 33.3% of all injuries reported in prospective studies [11,13,15-18,20,21,23,24,40,41,43,45]. The injury prevalence, over 6 months to lifetime period, ranged from 3.1 to 28.0% [16,18,20,21,40,43-45]. The injury incidence was 4.1 to 9.1% in the prospective studies with a follow-up of eight to twelve weeks, and 10.7 to 40.6% in retrospective studies [12,41,58].
Less commonly reported were hand/wrist (n = 273), knee (n = 214), elbow (n = 115), foot/ankle (n = 110), hip (n = 100) and neck (n = 58) injuries. Hand/wrist injuries accounted for 4.0 to 32.7% of all injuries [12,13,15-18,20,21,24,40-45,58]. The prevalence of hand/wrist injuries was 1.3 to 14.4% [16,18,20,21,40,43-45]. Whereas, the injury incidence was betweenn 1.7 and 37.5% [12,13,24,41,42,58]. Knee injuries accounted for 4.7 to21.4% of all reported injuries. The prevalence for knee injuries ranged from 2.4 to 13.6%, the injury incidence ranged from 2.5 to 14.3% [12,13,15-18,20,21,23,24,40,41,43-45,58]. Elbow injuries were accounting between 2.0 and 17.9% of all injuries [12,13,15-18,21,23,24,40,41,43-45]. The prevalence for elbow injuries was between 0.5 and 18.9% [16,18,40,43,44,45]. The incidence for elbow injuries ranged from 0.9 to 7.4% [12,13,23,24,41]. Ankle/foot injuries were accounting between 3.0 and 10.2% of all injuries [12,13,15-18,21,23,24,40,41,43-45]. The prevalence of ankle/foot injuries ranged between 0.7 and 11.4%, the incidence was between 0.6 and 13.1% [12,13,15-18,21,23,24,40,41,43-45]. Hip/thigh injuries were less reported injuries with 1.6 to 13.3% of all injuries reported [12,13,15-18,21,23,24,40,41,43-45]. The prevalence for hip injuries was between 1.0 and 12.8% [16,18,21,43,44,45]. The incidence was ranged between 0.6 and 9.4% [12,13,23,24,41,58].
Eight out of eighteen included studies have investigated CrossFit related exercises and training modalities that may be associated with the occurrence of injury [12,20,22,24,40,41,43,45]. All these results were based on self-reported findings.
Two out of eight studies only reported the association with an injury and the type of training [20,45]. Mehrab, et al. found that 100 injuries (39.7%) occurred during participation in a WOD [45]. Minghelli, et al. found that most injuries occur during (unspecified) training sessions (85.9%) [20]. Both studies did not report which movements were associated with the injuries [20,45].
In six studies the specific type of movements or exercises associated with the occurrence of an injury have been reported [12,22,24,40,41,43]. Five studies reported that most injuries were related to weightlifting or power lifting movements [12,22,24,40,43]. Four studies reported the distribution over injured body part among those movements [12,22,41,43]. Three studies reported lower back as most common injury in association with weightlifting or power lifting movements [12,41,43], followed by shoulder injuries [12,22,43]. Five studies have reported specific exercises that may result in a higher injury risk; specifically, the overhead press, snatch, dead lift and squat variations [12,22,24,40,41]. The injury incidence or prevalence associated with specific exercises were not reported in currently published literature.
One study reported that most injuries (40% of all cases) were associated with gymnastic exercises.11 Four other studies reported that injuries were associated with gymnastic exercises [12,22,40,43]. In four studies, shoulder injuries were found as most common injuries associated with gymnastic movements, followed by wrist injuries [12,22,40,43]. Two studies specified the exercises associated with potential higher injury risk: kipping pull-ups, and ring dips were commonly reported as exercises that were associated with the occurrence of shoulder injuries [41,22]. Summitt, et al. reported ring muscle-ups as an exercise with a high risk for shoulder injuries [22]. Alekseyev, et al. supported this finding by reporting muscle-ups as a related exercises in 5% of the cases, however did not report the distribution of these number into specific body parts [40]. Eight studies reported conditioning or endurance exercises, however specific conditioning or endurance exercises were not reported [12,20,22,24,40,41,43,45].
The purpose of this study was to review the injury prevalence in CrossFit trained participants, in particular, specified to injured body parts. The injury prevalence wasbetween 19.4 and 73.5% [15-18,20-22,40,43-45]. The injury incidence which was reported in seven studies, was between 12.8 and 66.2%. Shoulder injuries, lower back injuries, and hand/wrist injuries were found as most common injury location associated with CrossFit training [12,13,16,18,20-24,40,41,43-45,58]. Gymnastic movements as kipping pull-ups, ring dips and muscle ups were reported as exercises with a higher risk for shoulder injuries [22,40,41]. Lower back injuries were more commonly reported in association with weightlifting and power lifting movement. Overhead press, dead lift, snatch and squats were reported as exercises with a higher risk for injuries [12,22,24,40,41,43].
The majority of included studies in this systematic review had a retrospective design. Only three out of eighteen included studies had a prospective study design [13,23,24]. Of these prospective studies, Moran, et al. and Larsen, et al. reported a relatively low injury incidence (12.8% and 14.9%). The relatively short follow-up period, 12 and 8 weeks respectively [23,24], may have resulted in a lower injury incidence compared to other studies. Both studies found that lower back (25.0-33.3%) and knee injuries (20.0-21.4%) were more commonly reported than shoulder injuries (6.7-7.1%) [23,24]. It could be that during the study period of 8 and 12 weeks, focus was on certain exercises or muscle groups which in this case put more strain on the lower back and knee and less focus on shoulder movements [23,24]. This could be confirmed by the fact no injuries were reported associated with gymnastics movements [24]. Larsen, et al. investigated the injury incidence and rates only among athletes with no history of CrossFit participation, this may also influence the followed programming and the complexity of the performed movements [23]. The third prospective study, performed by Szeles, et al. reported a higher injury incidence (32.8%) compared to the studies of Larsen et al. and Moran, et al. [13,23,24]. The follow-up period was 12 weeks, similar to the study of Moran, et al. however significant more participants were included in the study of Szeles, et al. [13,24]
Highest injury prevalence has been reported in the study performed by Hak, et al. (73.5%) [18] This was the first study that investigated injury rates and profiles among CrossFit athletes. When CrossFit was founded and registred in 2000, the sport was still relatively new at the time this study was conducted. The lack of scientific knowledge about injuries associated with CrossFit training could have had an impact on injury management, programming, and coaching at that time. Also, a relatively open injury definition is used in this study.
Different injury definitions were used in the included studies. It is recognized that to date there is no widely used definition of what constitutes a sports injury, especially among CrossFit trained participants [60-62]. Study outcomes might have been influenced by the used injury definition. The use of a less specific injury definition may result in higher incidence or prevalence numbers, since par example a bit of pain in the knee already could be considered as an injury. Further research is recommended to create a clear injury definition.
In two included studies participants were only able to report a single injury over the injury registration period [4,44]. Two studies did reported the percentage of injuries among the specific body parts, but did not report the total number of injuries [15,17]. Tawfik, et al. reported 168 injured participants. The purpose of their study was to examine hand/wrist injuries, there for only 55 injuries were specified by the specific body part. The other 113 injuries were unspecified [42]. All studies were based on self-reported injury data. There is a risk that the actual number of injuries was underestimated or overestimated [10,63]. Injuries diagnosed or controlled (para) medicals may provide more valid and reliable information [10]. Therefore, the methods used for collecting data on the number of injuries and how they could occur, should be taken into careful consideration. Further prospective research with (para) medical approved injury diagnosis in a larger population is needed to obtain more reliable information to describe specific injury types and risk factors associated with the participation in CrossFit training.
Shoulder injuries among CrossFit trained participants were most commonly reported association with gymnastic movements [12,22,41,43]. In sports like gymnastics, ankle, elbow and shoulder injuries are common reported injuries [24,64-67]. Ankle and elbow injuries could be caused by the high level of jumping and tumbling in a sport such as gymnastics, which is not comparable with CrossFit. Within gymnastic exercises ring dips and kipping movements were frequently reported to be injury related. However, the relationship between the specific exercises and the reported injuries have not been studied yet. From a biomechanical point of view a lack of optimum muscle stiffness, strength and flexibility might cause the injuries. Increased stiffness were found tobe associated with bony injuries and decreased stiffness with soft tissue injuries in other sports [68-71]. Furthermore, it is known that a greater physiological stress and fatigue experienced lead to a higher injury risk [69,70]. Several studies on the effects of fatigue have described a decrease of joint stability, alterations in muscle activity, changes in balance and muscle function and decrements in pro prioceptive ability, in combination with high intensity, increasing loads and the occurrence of fatigue [68-71]. Specifically for shoulder injuries, a relationship between a decreased rotational strength and the occurrence of shoulder injuries have been found in overhead and throwing athletes [72-78]. However, this still needs to be studied in CrossFit. CrossFit training can be rendered as a composite training of gymnastics, weightlifting and power lifting movements. In this systematic review, six studies indicated that most injuries during CrossFit training occur within weightlifting or power lifting exercises [12,22,24,40,41,43]. In sports as weightlifting and power lifting, shoulder and lower back were frequently reported injury locations [9,25,79]. Comparable results were found in this study.
Our study adhered to the PRISMA guidelines and we performed an extensive search strategy assisted by a biomedical information specialist. This resulted in a new finding which adds to the currently available literature: hand/wrist injuries were the third most common injury location and could therefore be of interest in future research. Despite our thorough study design, this study has several limitations. Eighteen studies have been included in this review. Fourteen of these were rated as fair to poor methodological quality. Three out of four studies rated as good methodological quality were prospective studies [13,23,24]. A prospective design gives more accurate results by reducing the risk of recall bias. The retrospective studies within this systematic review collected injury data over a wide diversity of time. This makes it difficult to compare the reported findings.
The use of a clear injury definition has not been included in our eligibility criteria. As a result, one study has been included without reporting an injury definition [40]. Therefore, the reported data should be taken into careful consideration. To the best of our knowledge, no studies using (para) medics to diagnose or confirm injuries were published. Self-reported data may lead to an overestimation or underestimation of the reported number of injuries [10,63].
Eleven articles have been excluded, after full-text request by corresponding author, based on the absence of the full-text article. Based on given abstracts, four articles of the excluded studies may contain useful information for this systematic review [80-83]. Due to the absence of the full-text article these results could not been included or compared with the results of this review. One article has been excluded since we were not able to extract the number or proportion of injured body parts from the article, the authors were contacted but unfortunately did not respond to our request [14]. One article has been excluded because it was unclear if the reported injury proportion was among the CrossFit participants or amongst the total sample studied [79]. The exclusion of this article may have influence the results of this article since high injury proportions were reported.
The inclusion of only active CrossFit members in retrospective studies might have led to a selection bias. Former CrossFit members, who maybe have had to cancel their membership due to a musculoskeletal injury associated with CrossFit training, could not be included in the studies.
According to the studies included in this systematic review, the injury prevalence in CrossFit participants was between 19.4 and 73.5% [15-18,20-22,40,43-45] and the injury incidence was between 12.8 and 66.2% [12,13,23,24,41,42,58]. Shoulder injuries (6.7to 40.6% of all injuries), lower back injuries (12.9 to 36.0%) and hand/wrist injuries (4.0 to 32.7%) were found as most common injury location associated with CrossFit training. Knee, elbow, ankle/foot, hip and neck injuries were less commonly reported [12,13,16,18,20-24,40,41,43-45,58]. The majority of shoulder injuries were associated with gymnastic exercises such as ring dips, ring muscle ups, and exercises containing kipping movements [22,40,41]. Lower back injuries occurred more during weightlifting and power lifting exercises. Overhead press, dead lift, snatch and squats were reported as exercises with a higher risk for injuries.
Not applicable.
Not applicable.