Objective: To investigate the effects of acupuncture on pain and stiffness intensity and the symptoms associated with DOMS after 24 and 72 hours following the induction of DOMS.
Design: A preliminary, randomized controlled single blind study.
Methods: 22 healthy physiotherapists and podiatrists (10 female and 12 male) aged 21-48 years, were randomly assigned to an acupuncture intervention group or a non-treatment/control group. Immediately following the induction of DOMS, the treatment group underwent 20 minutes of manual acupuncture while the control group rested for 20 minutes. A Visual Analog Scale (VAS) and the short-form McGill Pain Questionnaire (SF-MPQ) were used to evaluate the experience and intensity of pain and muscle stiffness of each participant. Data analysis was conducted using SPSS 25. Independent samples t-tests and Levene's tests for homogeneity of variances were completed for all data sets.
Results: This study demonstrated a significant (P < 0.05) effect of acupuncture in the reduction of pain and stiffness compared with the control group at 24 and 72 hours following the induction of DOMS. The acupuncture intervention group reported 79% less pain and 41% less stiffness than the control group 24 hours after the induction of DOMS and 80% less pain and 62% less stiffness than the control 72 hours following the induction of DOMS.
Conclusions: The results of this study demonstrated the beneficial effects of selected acupuncture points in reducing both pain and stiffness 24 and 72 hours following the induction of DOMS. The findings of this study further indicate that stiffness may pose a greater problem to the recovery of athletes following intense exercise than pain; therefore, treatment should be aimed at reducing both pain and stiffness.
Delayed-onset muscle soreness, DOMS, Acupuncture, Stiffness, Muscle pain
Delayed-Onset Muscle Soreness (DOMS) relates to pain and stiffness someone experiences following exercise. DOMS can occur after any type of exercise activity but particularly after exercise which has involved an eccentric component. The intensity of the symptoms increases for the first 24 hours after exercise and peaks at around 24-72 hours, and usually ease off within 5-7 days post exercise [1]. DOMS can be seen in novice or experienced athletes following a bout of intense eccentric loading exercise [2]. It is classified as a grade I muscle strain [3], which is experienced as muscle tenderness on palpation and stiffness on movement. There is a reduction in muscle strength, range of motion, localized swelling, increased level of intramuscular enzymes such as creatine kinase, lactate dehydrogenase, and myoglobin [4-7]. The primary cause of pain is from the release of inflammatory cytokines, and prostaglandins that will sensitize nociceptive pathways [8-10]. It has been extensively documented in human and animal studies that muscle injury occurs following intense bouts of eccentric muscular contraction and is followed by an inflammatory response and accumulation of neutrophils and type 1 proinflammatory macrophages [4,11-18]. Macrophages have been reported to differentiate into subtypes (M1 and M2) depending on the stimuli that is initiated. Following intense exercise, neutrophils and M1 proinflammatory macrophages are first to arrive in the muscles. M1 macrophages secrete proinflammatory cytokines (e.g., TNF-α, IL-1β, and IL-6), as well as secretory leukocyte protease inhibitor [19]. They also attract more inflammatory cells. Excess production of reactive oxygen and nitrogen species by inflammatory cells have been reported to intensify muscle damage [16,20,21]. This will impact negatively on athletic performance and increase the risk of sustaining injuries.
Following exercise-induced muscle damage there is reported muscle stiffness; however, in the assessment and management of DOMS, stiffness has received very little attention in comparison with other parameters associated with soreness and weakness. Howell and colleagues [22] observed changes in muscle stiffness, strength loss, swelling and soreness following exercise-induced injury in the elbow flexors of humans. They found that stiffness increased immediately after exercise and stayed elevated for about 3 days before exhibiting a marked downward trend. These finding are supported by an earlier study by Jones, et al. [23], who found that after eccentric exercise of the elbow flexors, resting muscle stiffness increased and the relaxed arm adopted a slightly flexed posture. There have been numerous studies that have investigated the effectiveness of acupuncture in the management of DOMS. However, most studies that have investigated the effect of acupuncture in the management of DOMS have focused on pain and activating peripheral segmental and central pathways through needling directly into the affected muscles to elicit an acupuncture-induced analgesia. Generally, none of the points in these studies was chosen to address the physiological aspects of DOMS. For acupuncture to be effective in the management of DOMS, it is important to choose points with regards to their evidence-based physiological effect on the inflammatory and healing process and not solely for their effect on pain. Inflammation will cause both pain and stiffness within muscles. Pain and stiffness are symptoms of DOMS and not the cause, hence measures to reduce inflammation and initiate the healing process will in turn lead to a reduction in pain and stiffness following intense eccentric loading activity. Therefore, the aim of the current study was to investigate the effects of acupuncture on pain and stiffness intensity and the symptoms (heaviness, tenderness, cramping, and aching) associated with DOMS after 24 and 72 hours following the induction of DOMS. Acupuncture points in this study were selected based on their known physiological effect on the inflammatory and healing process of muscles and tendons. The findings from this study will give practitioners the tools to allow athletes to train hard and recover quickly in preparation for competition.
This was a randomized controlled single blind study which followed the guidelines of the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) as outlined by MacPherson, et al. [24]. Following ethical committee approval, subjects were recruited from convenience sampling of physiotherapy and podiatry students on the medical acupuncture foundation course. Twenty-two healthy physiotherapists and podiatrists (10 female and 12 male) aged 21-48 years were randomly assigned to an acupuncture intervention group or a non-treatment/control group. Randomization was generated by a computer-based random number table. Participants were included if they had no previous experience of acupuncture, were fit and healthy and were not taking any anti-inflammatory medication or painkillers. Prior to any testing, each subject was given a verbal explanation of the experimental procedure and all subjects gave their written informed consent. The person analyzing the data was blind to each participant; however, it was difficult to blind each participant as they were podiatrists and physiotherapists undergoing acupuncture training. The practitioners giving acupuncture were not involved in the assessment outcomes.
To elicit DOMS each participant in both groups performed 5 minutes running warm-up followed by eccentric loading exercises consisting of 5 sets of 20 kneeling gun drills, 5 sets of 20 squat jumps and 5 sets of 20 squats, with 30 seconds rest between each set.
Immediately following the induction of DOMS, the treatment group underwent 20 minutes of manual acupuncture supervised by an experienced acupuncture practitioner of 20 years. Before the needles were inserted into the acupuncture points, the skin was cleaned with sterilized gauze and sterile solution (chlorhexidine). Acupuncture was applied to GB-34, ST-36, SP-6, and Liv-3. Phoenix A-Type 0.25 mm × 25 mm stainless steel handle needles with guide tubes were inserted to a depth of between 0.5 mm-1 cm depending on the anatomical location of the acupuncture points and the subject's constitution (e.g., skin thickness and subcutaneous fat layer). Deqi was not sought in this study. The needles were left in place for 30 minutes and manually stimulated (rotated back and forth) every 5 minutes for 10-15 seconds. Immediately upon the removal of the needles, Magrain seeds were applied to each of the acupoints and the participants were advised to manipulate each point for one minute each day. A combination of traditional Chinese and western medical evidence-based approach was taken in the administration and selection of acupuncture points. Classical acupuncture points were chosen based on their physiological effects on enhancing the repair process of muscles and their ability to reduce inflammation. ST-36 and SP-6 was chosen as several studies have demonstrated the anti-inflammatory effect of these points in the management of acute inflammation [25-32]. Liv-3 was chosen as it has been shown to enhance blood flow to the muscles and the periphery [33]. Liv-3 is recommended where there is acute tear of the muscles anywhere in the body. GB-34 was chosen as it is the influential point for disorders of the muscles and tendons and is recommended when there is stiffness and tightness of the muscles and joints, and contraction of the sinews [34]. Immediately following the induction of DOMS, the control group rested in a supine position on the couch for 20 minutes. Both groups were advised not to partake in any other activity and not to take any anti-inflammatory medication over the next few days.
The Visual Analog Scale (VAS) was used to assess the primary outcome measure of muscle pain and stiffness. The VAS is a common scale used in a clinical setting and research to measure a patient's pain intensity. It has been shown to be a reliable and valid assessment tool for measuring acute and chronic musculoskeletal pain [35,36] and in the assessment of DOMS [37,38]. The secondary outcomes were assessed using the short-form McGill Pain Questionnaire (SF-MPQ) to evaluate the experience and intensity of symptoms (heaviness, tenderness, cramping, and aching) of each participant. Pain, stiffness, and symptoms assessment were conducted 24 hours and 72 hours following the induction of DOMS. The SF-MPQ is commonly used for assessment and diagnosis in research in a wide range of pain-related conditions. The test-retest reliability of the SF-MPQ has been found to be adequate for general musculoskeletal pain [39,40].
Data analysis was conducted using SPSS 25. Independent samples t-tests and Levene's tests for homogeneity of variances were completed for all data sets. Any corrected results for data with unequal variances are reported where necessary. Group means, and their respective standard deviations, were used for statistical analysis. A paired t-test was used to test for a significant difference in stiffness intensity and pain intensity between the intervention group and the control group 24 and 72 hours following the induction of DOMS. A P value of less than 0.05 was considered as significant in all tests that were conducted.
Twenty-two healthy physiotherapists and podiatrists (10 female and 12 male) aged 21-48 years completed the study with no adverse reactions and no dropout during the procedure. Baseline assessment at the start of the study indicated that all subjects were pain free, fit, and healthy.
Analysis for stiffness intensity (VAS) between groups over time revealed a significant effect of acupuncture intervention at 24 hours t (20) = -2.541, P < 0.05) and 72 hours t (20) = -2.972, P < 0.05) following the induction of DOMS (see Figure 1). The acupuncture group reported 41% less stiffness than the control group 24 hours after the induction of DOMS and 62% less stiffness than the control 72 hours following the induction of DOMS.
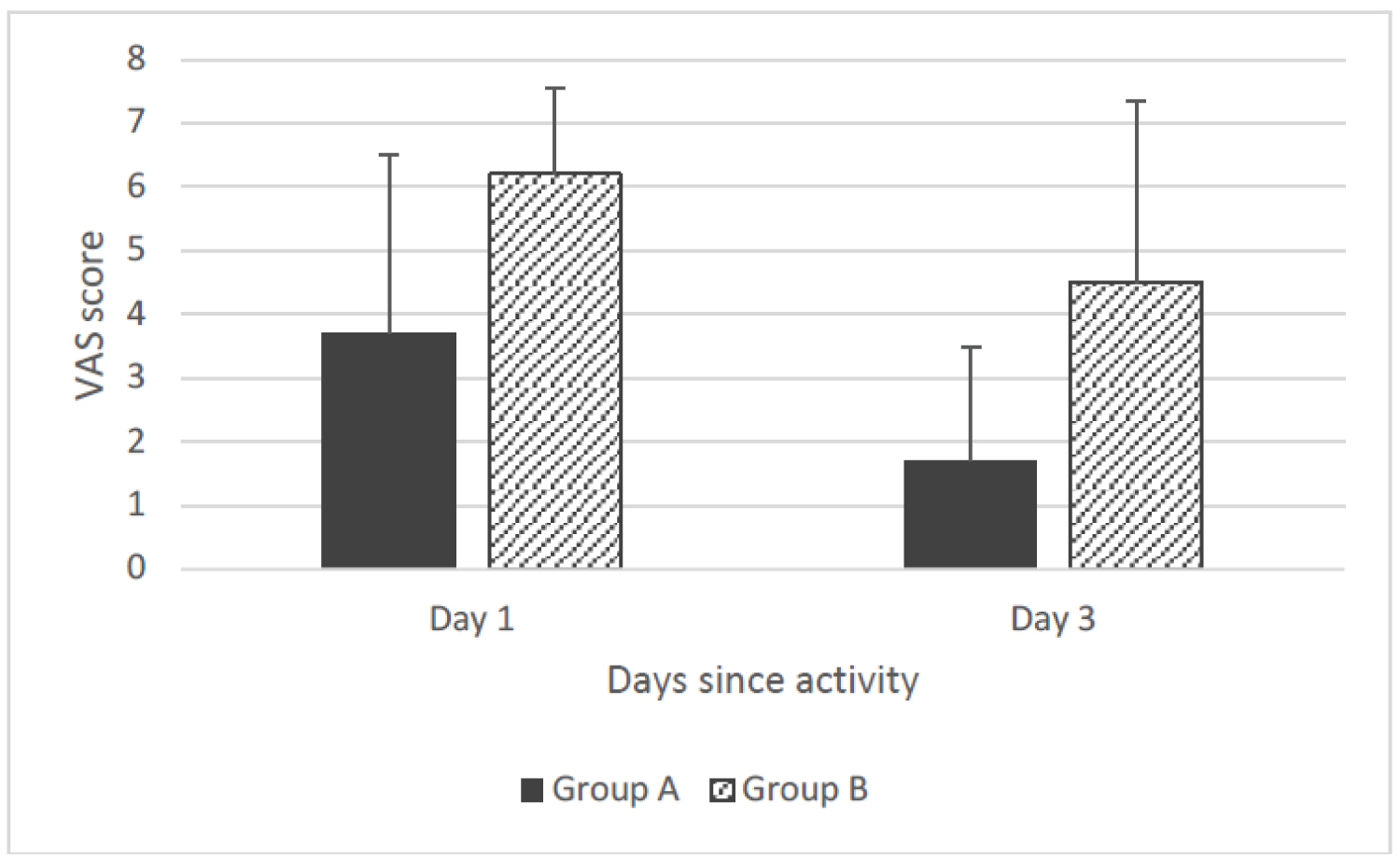 Figure 1: A chart to show average severity of self-reported VAS of stiffness.
View Figure 1
Figure 1: A chart to show average severity of self-reported VAS of stiffness.
View Figure 1
Analysis for pain intensity (VAS) between groups over time revealed a significant effect of acupuncture at 24 hours t (13.970) = -4.432, P < 0.05) and 72 hours t (20) = -4.251, P < 0.05) following the induction of DOMS (see Figure 2). The acupuncture group reported 79% less pain than the control group 24 hours after the induction of DOMS and 80% less pain than the control 72 hours following the induction of DOMS.
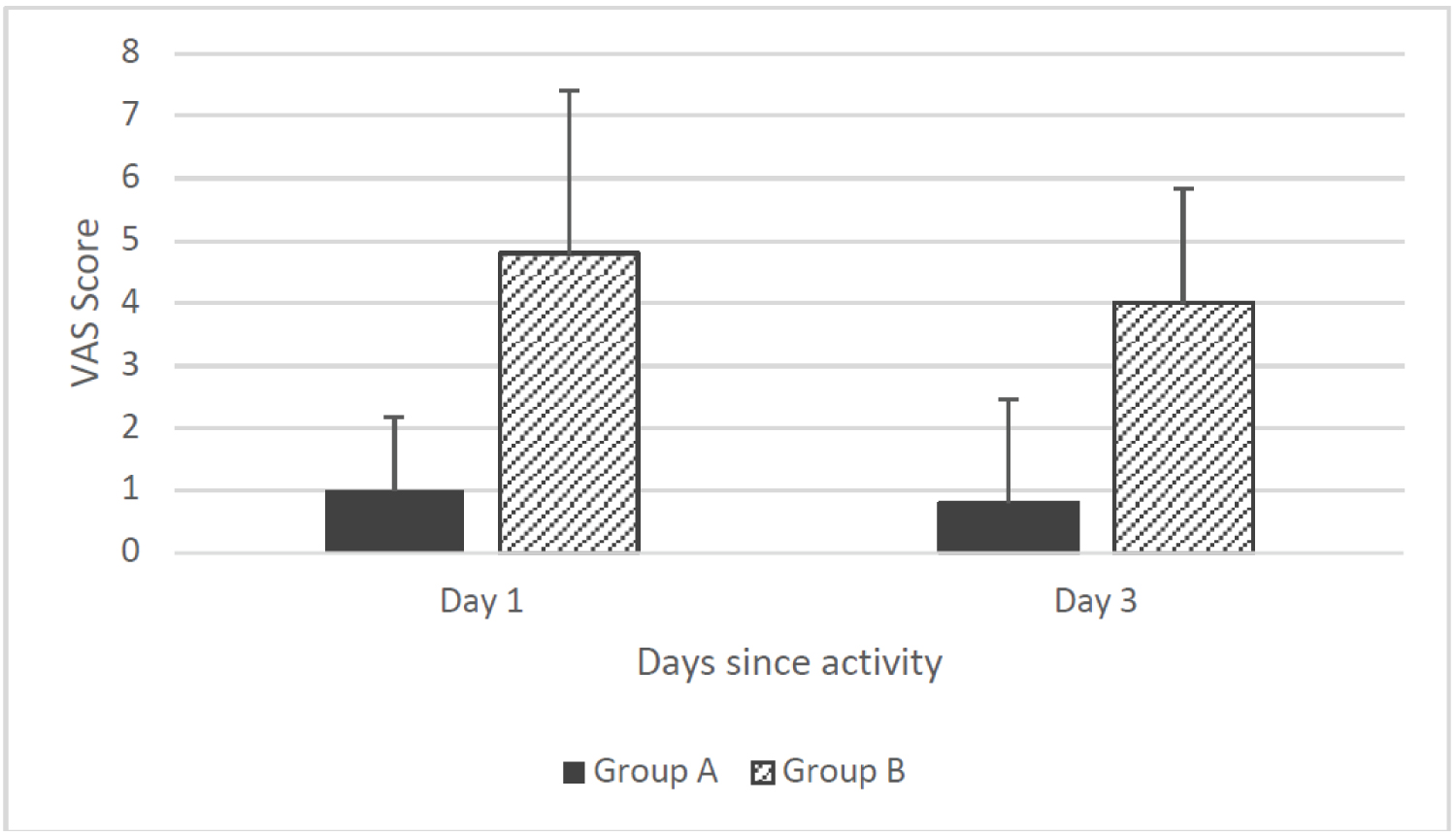 Figure 2: Chart to average severity of self-reported VAS of pain.
View Figure 2
Figure 2: Chart to average severity of self-reported VAS of pain.
View Figure 2
Mean reported stiffness was highest in both the acupuncture group (3.7) and control (6.3) group 24 hours following the induction of DOMS and reduced by 54% in the acupuncture group and 29% in the control group by 72 hours.
Mean reported pain was highest 24 hours following the induction of DOMS in the acupuncture and control groups, and reduced in the acupuncture group by 20% and the control group by 17% by 72 hours. Within group analysis for pain indicated no significant change between day 1 and day 3 for the acupuncture (P > 0.05) and control (P > 0.05). While, within group analysis for stiffness in the acupuncture group indicated a significant (P < 0.05) reduction by 54% between day 1 and day 3 but no significant (P > 0.05) change in stiffness between day 1 and day 3 in the control group.
The SF-MPQ showed that the acupuncture group reported fewer symptoms (heaviness, tenderness, cramping, and aching) than the control group, and the symptoms reported were less severe. As shown in Figure 3, on day 1, across all participants in the acupuncture group, a total of 41 symptoms were reported; 26 of these were mild, 14 moderate and 1 severe. By day 3 this had reduced to 18 symptoms: 17 mild and one severe. The control group reported a total of 51 symptoms on day 1, 25 of which were mild, 21 moderate and 5 severe. By day 3, this had reduced to 42 symptoms: 26 mild, 13 moderate and 3 severe. The most reported symptoms for both groups were cramping, aching, heaviness, and tenderness. Figure 4 illustrates the occurrence of the most reported symptoms across both groups, at day 1 and day 3.
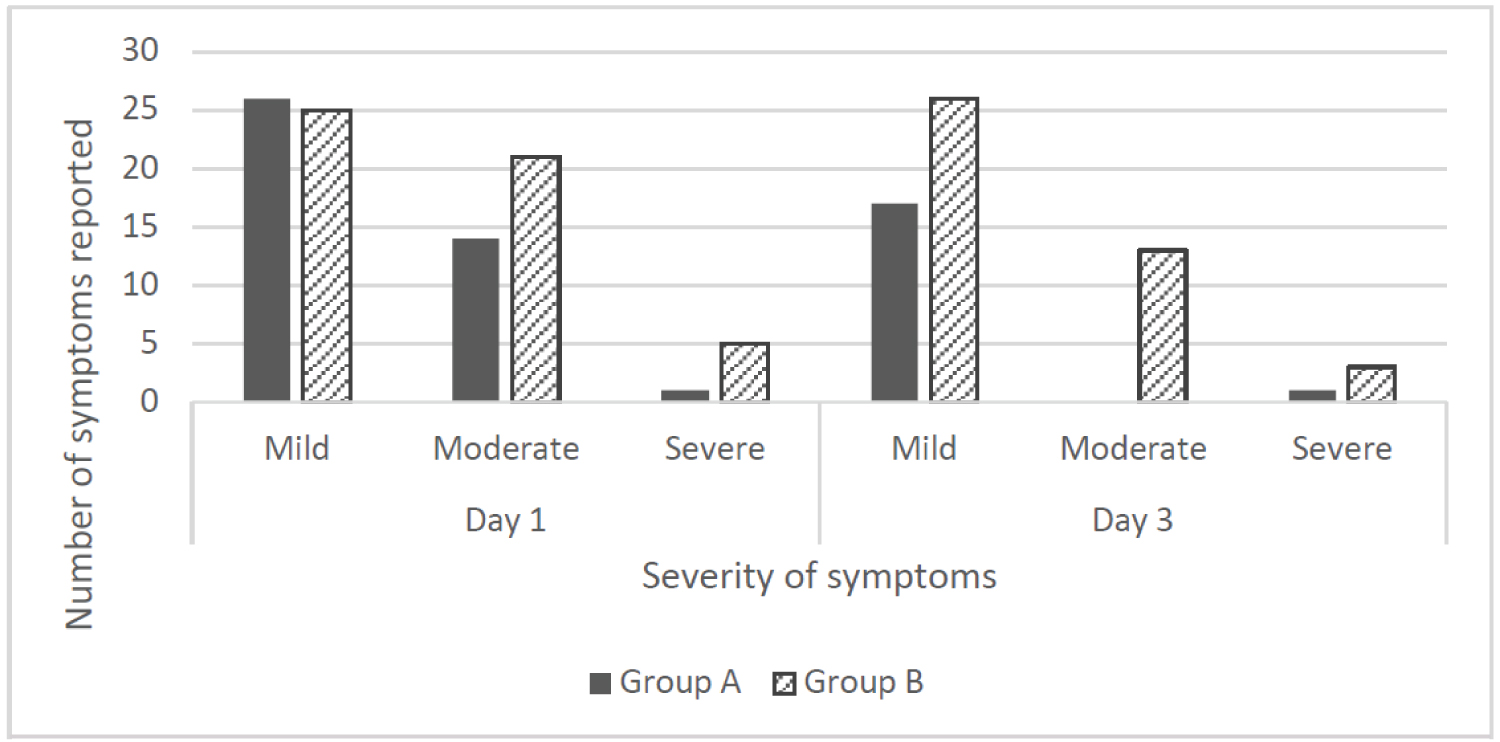 Figure 3: Chart to show number and severity of reported symptoms.
View Figure 3
Figure 3: Chart to show number and severity of reported symptoms.
View Figure 3
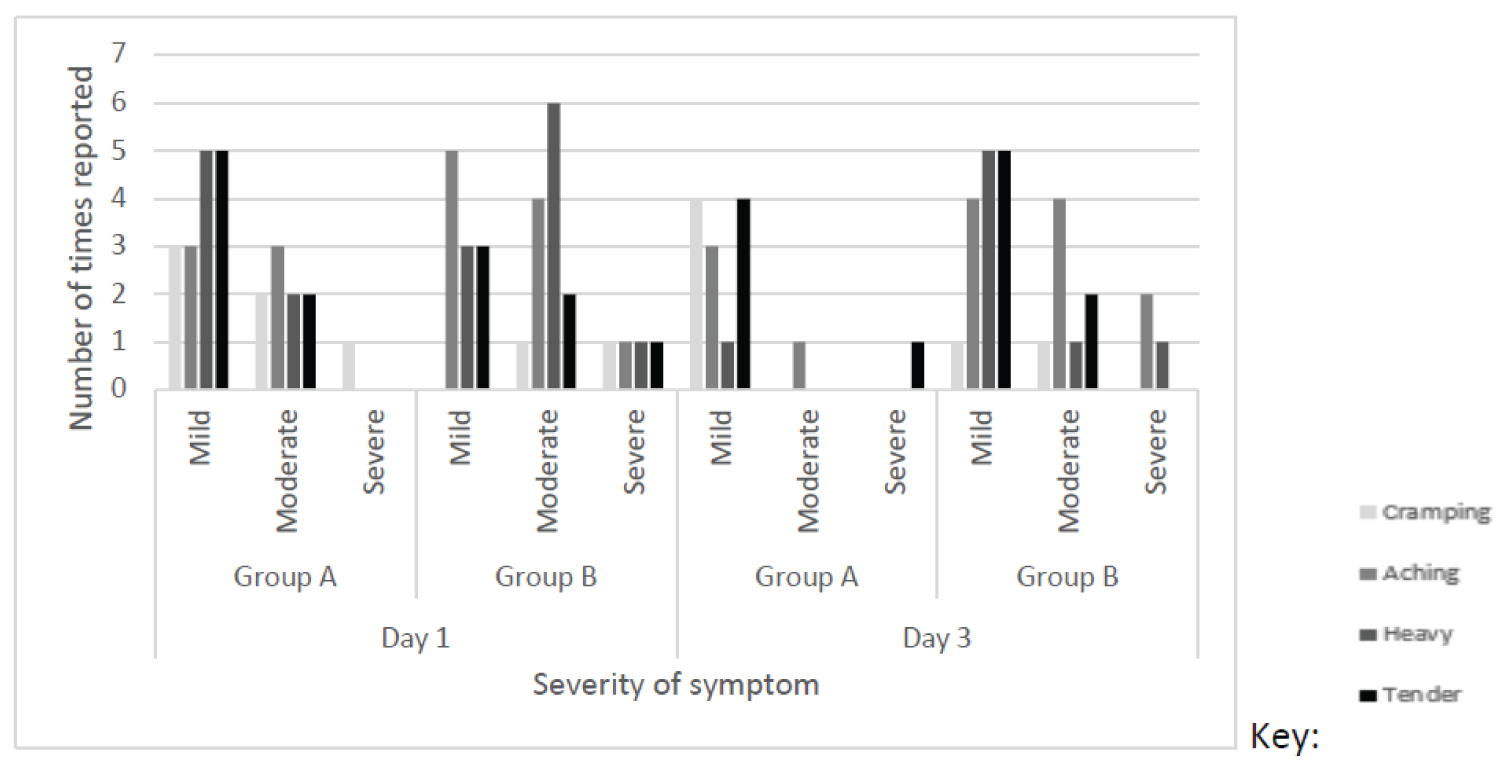 Figure 4: Chart to show most common symptoms of cramping aching heaviness and tenderness.
View Figure 4
Figure 4: Chart to show most common symptoms of cramping aching heaviness and tenderness.
View Figure 4
The primary purpose of this study was to investigate the effects of acupuncture on reducing the symptoms of DOMS following intense eccentric loading exercise in healthy adults. This study demonstrated a significant effect of acupuncture in the reduction of pain and stiffness compared with the control group at 24 and 72 hours following the induction of DOMS. The acupuncture intervention group reported 79% less pain and 41% less stiffness than the control group 24 hours after the induction of DOMS and 80% less pain and 62% less stiffness than the control 72 hours following the induction of DOMS. The difference between the acupuncture intervention and control groups is quite large; therefore, one can infer that acupuncture will produce clinically important reductions in DOMS in healthy adults. Our findings agree with earlier studies [41-46] that found classical acupuncture and tender points were more effective than sham or no acupuncture in reducing VAS values for pain up to 72 hours following the induction of DOMS.
Previous studies that assessed the effect of acupuncture on DOMS mainly focused on reducing pain; however, stiffness is a common complaint of DOMS and can indicate that there is some inflammation present within the muscles. Similar to the study by Howell and colleagues [22], our findings showed that 82% of the acupuncture and 91% of the control group presented with greatest stiffness 24 hours following the induction of DOMS. The reported VAS rating was greater for stiffness than pain and was slower to reduce back to baseline than pain. Overall stiffness was reported to be mild in the acupuncture group with a mean VAS rating of 3.7 at 24 hours which reduced to 1.7 at 72 hours, whereas the control group reported a moderate to severe stiffness of 6.3 (mean) at 24 hours, which reduced to 4.5 VAS rating at 72 hours. This indicates that stiffness may pose a greater problem to athletes following intense exercise than pain, and treatment should be aimed at reducing both pain and stiffness.
The results of this study demonstrated the beneficial effects of selected acupuncture points in reducing both pain and stiffness 24 and 72 hours following the induction of DOMS. The findings of this study further indicate that stiffness may pose a greater problem to the recovery of athletes following intense exercise than pain; therefore, treatment should be aimed at reducing both pain and stiffness.
The author has no conflicts of interest to declare regarding this manuscript.
No funding was received for this research.
The author thanks Bethany Liddington for her assistance with data analysis.