Spina bifida occulta represents a limited form of spina bifida. In this condition, the vertebral laminae fail to fuse. Spina bifida occulta can be diagnosed on prenatal ultrasound or after birth on routine x-ray. In most cases, SBO is asymptomatic. Here, we present the unique case of a 30-year-old male who presented with bilateral hamstring tightness of lifelong duration, with low back pain of one year duration. Physical exam was notable for bilateral knee flexion contractures of 20 degrees, reduced lumbar flexion by 20 degrees, hypertonicity of bilateral hamstring muscle bellies, with significant tenderness on palpation of ischial tuberosities. Additionally, three long, dark hairs were present at the level of the L5 spinous process, with asymmetrical gluteal cleft and a port wine stain on the right buttock. XR and MRI confirmed the diagnosis of L5 spina bifida occulta. The patient was referred to spina bifida clinic. Physical therapy including core strengthening and aggressive hamstring stretching significantly improved the patient's symptoms and functional mobility.
Spina bifida is a birth defect in which the spinal cord does not develop due to incomplete closure of the neural tube at approximately 28 days of gestation. Spina bifida is the most common birth defect affecting the central nervous system that results in permanent disability [1]. Spina bifida occulta (SBO) represents a limited form of spina bifida in which the defect is limited to the mesoderm of the posterior arch, preventing fusion of vertebral laminae. This defect rarely leads to maldevelopment of the spinal cord or meninges [2].
The prevalence of SBO varies from 1.2 to 50% in different study populations [3]. The most accurate estimate of occurrence rate is 17% of examined spines [4]. SBO can be diagnosed on prenatal ultrasound or after birth on routine x-ray (XR). In most cases, SBO is asymptomatic. However, symptoms may include back pain, enuresis, motor or sensory dysfunction, and disc pathology [5]. In addition, an increasing amount of evidence links SBO with a variety of clinical syndromes including tethered cord syndrome, genitourinary or gastrointestinal dysfunction, lumbar spondylolysis, foot deformities, and syringomyelia [4,6].
Here we present a case of SBO diagnosed in a 30-year-old patient who presented to a sports medicine clinic with bilateral hamstring tightness. Currently, there are no published case reports documenting the diagnosis of SBO after a chief complaint of hamstring tightness. The purpose of this article is to highlight the importance of obtaining imaging if SBO is suspected and to further describe management.
A 30-year-old male with past medical history significant for developmental delay presented for initial evaluation of chronic bilateral tight hamstrings of lifelong duration, with low back pain of one year duration. The patient had a history of autism and prior testing ruled out a genetic cause of developmental delay. He was conversational and able to walk and run independently. He was independent with all activities of daily living but required assistance with instrumental activities of daily living.
The patient's gait was notable for short steps with bilateral knee flexion contractures of 20 degrees. Lumbar flexion was reduced by 20 degrees. Knee extension was reduced by 50 degrees on the left, and 60-70 degrees on the right. Strength testing revealed full strength in bilateral hip flexion, knee flexion, knee extension, and ankle plantarflexion. Weakness was appreciated in bilateral ankle dorsiflexion. Sensation to light touch was intact throughout bilateral lower extremities. Hypertonicity was appreciated on palpation of bilateral hamstring muscle bellies, with significant tenderness on palpation of ischial tuberosities. He was tender on palpation of the L3 spinous process. Three long, dark hairs were present at the level of the L5 spinous process. The patient had an asymmetric gluteal cleft, with a 2-3 cm port wine stain on the right buttock near the gluteal fold.
Lumbar spine XR was obtained in the office, which revealed incidental occult spina bifida at the L5 level (Figure 1). Subsequent lumbar spine MRI confirmed the diagnosis of L5 spina bifida occulta (Figure 2). There was no evidence of meningocele or myelomeningocele on MRI. The patient was referred to a spina bifida clinic and physical therapy to improve posture, gait, and decrease hamstring tightness. Ten months after the diagnosis, the patient made significant gains including improved knee extension range of motion, posture, and gait.
 Figure 1: XR lumbar spine shows spina bifida occulta at the L5 level.
View Figure 1
Figure 1: XR lumbar spine shows spina bifida occulta at the L5 level.
View Figure 1
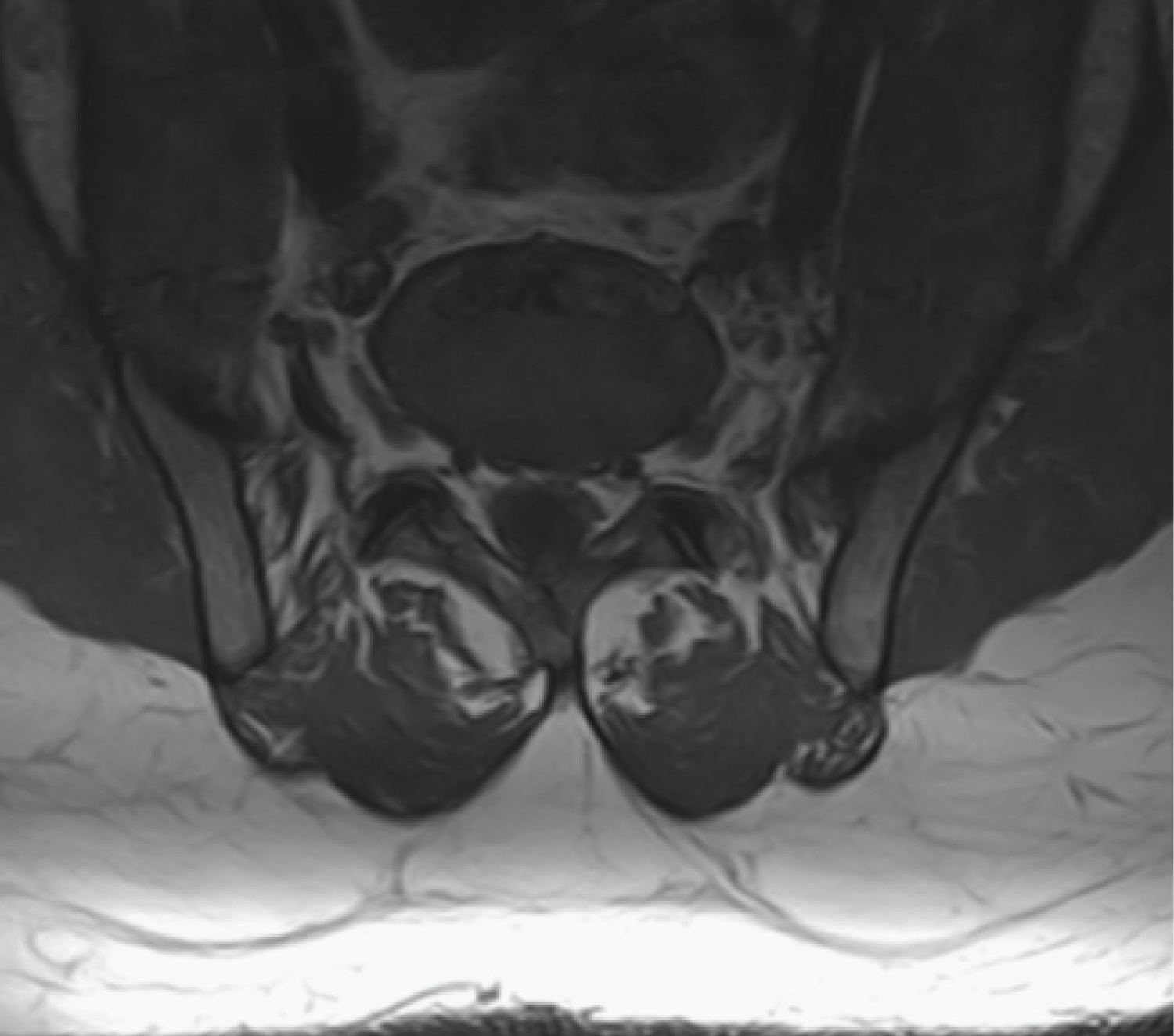 Figure 2: MRI lumbar spine confirms diagnosis of L5 spina bifida occulta.
View Figure 2
Figure 2: MRI lumbar spine confirms diagnosis of L5 spina bifida occulta.
View Figure 2
Spina bifida occulta is commonly detected incidentally on lumbar imaging. Physicians must be aware of the more serious conditions that can be associated with SBO, such as genitourinary symptoms and tethered cord syndrome [5,7,8]. These cases must be referred to an orthopedic spine specialist or neurosurgeon, and typically require surgical intervention.
In this case, the patient presented with long-standing bilateral hamstring tightness with chronic low back pain over the last year. He had additional physical exam findings consistent with spina bifida occulta including long dark hairs at the L5 spinous process, asymmetrical gluteal clefts, and a port wine stain. The patient's history and physical exam did not include any red flag signs.
The patient's hamstring tightness and low back pain were likely complications of spina bifida occulta. Spina bifida occulta reduces the attachment sites for multifidi muscles. This leads to impaired proprioception, which contributes to lower lumbar and pelvic instability [9]. The patient's long-standing pelvic instability likely led to chronic stress on the hamstring tendons, given their attachment at the ischial tuberosity.
In addition, tight hamstrings pull the pelvis posteriorly, leading to a forward flexed lumbar spine, which can predispose to low back pain. This patient's low back pain is likely multifactorial, due to the primary effect of lumbar spine instability and secondary effect from the hamstring tendons. The association between SBO and neuromuscular scoliosis has been previously reported, which highlights the importance of better understanding the potential impacts of these birth defects on the growing spine [10].
It is imperative to refer these patients with functional impairments to physical therapy. In this patient, a core strengthening program and aggressive hamstring stretching significantly improved his symptoms and gait.
This case report describes a new diagnosis of spina bifida occulta in a 30-year-old patient who presented with a chief complaint of bilateral hamstring tightness. This case demonstrates the importance of obtaining a thorough history, physical exam, and imaging (XR and MRI) to further direct management if spina bifida occulta is suspected. A course of physical therapy focused on core stabilization significantly improved the patient's range of motion and function, including posture and gait.
No disclosures.
Both authors contributed equally to this manuscript.