Previous studies have shown that High-Intensity Interval Training (HIIT) is effective in improving maximal oxygen uptake, blood pressure, and physical health-related indicators in older adults. However, whether HIIT is more effective in improving cardiorespiratory fitness and exercise capacity in older adults compared with Moderate-Intensity Continuous Exercise (MICT) remains controversial. This review and META analysis assessed the outcomes associated with HIIT on cardiorespiratory fitness and exercise capacity in older adults by searching five electronic databases (PubMed, Embase, SPORTDiscus, Scopus, and Cochrane Library) (built to July 2022). Relevant studies were included using the Cochrane Risk of Bias Assessment Tool; statistical analyses were performed using REVMAN software. HIIT significantly improved VO2max (HIIT vs. MICT) (weighted mean difference = 1.80, 95% confidence interval: 1.25-2.35, p < 0.001) and maximal heart rate, ventilation maximal power output compared to the MICT protocol. Subgroup analysis determined that training period < 12 weeks, training frequency three times/week, 20 min per intervention, < 80% intensity VO2 peak, 3 repetitions, < 60s per training session, and ≤ 90s rest time had the greatest effect on VO2 max. Compared with MICT, HIIT was more effective in improving cardiorespiratory fitness and exercise capacity in older adults.
Aging reduces the body's cardiorespiratory fitness and exercise capacity [1]. The ageing process reduces the body's cardiorespiratory fitness and exercise capacity. For each level of cardiorespiratory fitness, mortality due to cardiovascular disease is reduced by 16% [2,3]. The increase in cardiopulmonary health is associated with a 16% reduction in mortality due to cardiovascular disease. At the same time, improving exercise capacity is an effective means of improving survival in older adults [4]. Therefore, the implementation of cardiopulmonary health promotion and exercise capacity is essential. Therefore, the implementation of measures to promote cardiorespiratory fitness and exercise capacity is essential to reduce the incidence of disease mortality in older adults and to reduce government health care costs [5]. The current interventions to promote cardiorespiratory fitness are Current interventions to promote cardiorespiratory fitness include exercise training, medical treatments (medication and surgery), etc [6-8]. However, because medication and surgery do not provide long-term therapeutic benefits and may even have toxic side effects [9]. This suggests that exercise training may be a long-term solution with no side effects. Previous studies have shown that aerobic exercise is effective in improving cardiorespiratory fitness, exercise capacity and blood pressure [10-13]. However, lack of time to participate in exercise is a common problem for all elderly populations [14]. The lack of time for exercise is a common problem for all older adults. High-Intensity Interval Training (HIIT) is characterized by short bursts of high-intensity exercise with short intervals of rest or active recovery. Studies have shown that intense intervals of 1-2 minutes three times a day can reduce cardiovascular risk mortality in older adults by 47% [15]. In addition, HIIT can effectively improve the aerobic capacity of different people [16] as well as lower blood pressure, etc [17]. It is important to note that HIIT not only has the potential to improve aerobic capacity, but also to reduce blood pressure. It is important to note that HIIT is not only more time efficient than moderate intensity, but it has also been reported that older adults with cardiovascular disease can safely participate in HIIT [18]. These advantages make it a popular choice for patients and clinicians with aging-related diseases [17,19]. These advantages make it a popular choice for patients and clinicians with co-occurring disorders of aging. Previous META analyses have concluded that HIIT is more effective than MICT in improving aerobic capacity in older adults of different status, but only VO 2 max was compared in older adults, not in combination with other cardiorespiratory fitness indicators and not in subgroups [20,21]. However, only one study has been conducted on healthy older adults and based on this finding, subgroup analysis was conducted to provide specific exercise programs [22]. The only study that provided specific exercise programs was a subgroup analysis of healthy older adults with this finding. Unfortunately, older adults are more likely to have a disease related to cardiorespiratory function downregulation, suggesting that studies that include older adults with disease can provide a more comprehensive overview of the effects of exercise on cardiorespiratory function in older adults and that the effects of HIIT and Moderate Intensity Continuous Exercise (MICT) on cardiorespiratory function and exercise capacity improvement, as well as the effects of different indicators, may be relevant. The effects of HIIT and Moderate Intensity Continuous Exercise (MICT) on cardiorespiratory fitness and exercise capacity, as well as the effects of different indicators, may not be the same, and this poses a problem for targeted exercise prescription for older adults with different health conditions. In addition, previous META analyses comparing HIIT and MICT on blood pressure and exercise capacity in older adults with cardiometabolic abnormalities [23] and exercise capacity [24]. However, such isolated studies may have overlooked the intrinsic link between human cardiopulmonary function, blood pressure, and exercise capacity. Therefore, the purpose of this systematic evaluation and META analysis was to assess the effects of HIIT and MICT on different indicators of cardiorespiratory fitness and exercise capacity in older adults. Further subgroup analyses of the indicators with effects will be conducted to determine which exercise is more effective in modulating cardiorespiratory fitness and exercise capacity, and to reveal the intrinsic link between HIIT and human cardiorespiratory fitness, blood pressure, and exercise capacity.
This systematic evaluation and meta-analysis was registered with PROSPERO on February 8, 2022 (CRD42022302359) and follows the PRISMA-P statement [25]. The authors have read, understood and comply with the journal's ethical standards document.
Studies were included if they met the following criteria: 1. The exercise intervention involved supervised HIIT and MICT; 2. The mean age of subjects in the MICT and HIIT groups was ≥ 55 years; 3. The duration of the exercise intervention was ≥ 2 weeks (the shortest time effective for upregulating cardiorespiratory fitness). 4. The exercise modality of choice was running, cycling, and elliptical. The following were excluded from the study: 1. Type of literature was reviews, animal experimental studies, theoretical basis exploration, descriptive studies, conferences, etc.; full-text non-English papers, repeatedly published literature. 2. One-time exercise, experimental reports with ambiguous information and missing data literature; 3. Interventions containing combined dietary or pharmacological interventions; non-controlled and cross-sectional studies. Ending indicators: cardiorespiratory fitness (VO 2 , RER, HR, VE/VO 2 , OUES), physical performance (6 min, METs, peak power output, time up and go test), blood pressure (SBP, DBP). HIIT is usually defined as "near maximum" effort performed at an intensity that elicits ≥ 80% "HRmax" effort to elicit ≥ 80% HRmax [17]. Subjects were not restricted by Body Mass Index (BMI), gender, pathology, or race; there were no restrictions on exercise duration.
Electronic database searches were conducted in PubMed, Embase, SPORTDiscus, Scopus, and the Cochrane Library using all available records as of September 10, 2022. The MeSH terms used were "high-intensity interval training" and "elderly" or "cardiopulmonary index" and related terms. Specifically, the database search was performed using keywords and truncations along with the MeSH terms: "High-Intensity Interval Training" OR "High Intensity Interval Training" OR "High-Intensity Interval Trainings" OR "Interval Trainings" High-Intensity" OR "Training, High-Intensity Interval" OR "Trainings, High-Intensity Interval" OR "High- Intensity Intermittent Exercise" OR "Exercise, High-Intensity Intermittent" OR "Exercises, High-Intensity Intermittent" OR "High-Intensity Intermittent Exercises" OR "Sprint Interval Training" OR "Sprint Interval Trainings" OR "HIIT" OR "HIIE" OR "high-intensity interval exercise" OR "sprint interval exercise" OR "high intensity intermittent exercise" OR "high-intensity intermittent training"; elderly "aged" OR "elder" OR "old" OR " senior" OR "adult" OR "veteran" OR "geriatric" OR "retirement" OR "geriatric" OR "aging" OR "elderly" OR "seniors" and cardiopulmonary indicators "systolic blood pressure" OR "diastolic blood pressure" OR " peak oxygen" uptake OR "homeostatic model assessment insulin resistance" OR "low-density lipoprotein cholesterol" OR "glucose" OR "HbA1c" OR "body fat" OR "fasting insulin" OR "C reactive protein" OR "interleukin 6"). These terms and descriptors are combined using the Boolean operators "AND" and "OR". There is no time limit for publication. In addition, the reference lists of included articles and related reviews were scanned for potentially relevant studies.
The following steps were performed by two independent evaluators (YY, CYX), and any discrepancies were resolved by discussion or consensus with a third evaluator (HGX). Complete papers were collected, and corresponding authors were contacted by email when complete manuscripts were not available. In addition, to avoid missing relevant literature, the reference list of relevant studies was manually searched to identify additional eligible studies [26]. Intervention characteristics were extracted independently by two authors (YY and CYX) according to a pre-prepared table. Extracted data included authors' names, year of publication, basic subject information (number, sex, age) exercise intervention details (type, duration, frequency and intensity); and all relevant cardiorespiratory fitness and exercise capacity outcomes. Extraction of data from the graphs was not included in the study. Standardization of different units of outcome measures was performed when necessary. For trials with missing data, data remained excluded from the analysis if there was no response from the contact author. Data were analyzed using RM and study results were described as MD or SMD, and if there was heterogeneity in the results, the source of heterogeneity was further explored [26].
The search strategy identified 6709 articles from electronic databases and an additional 3 articles from previous relevant META studies were found manually on PubMed. A total of 2317 duplicate publications were removed, 2969 articles were screened out in the title, and 1344 were excluded after abstract screening. Of the remaining 87 articles, 30 met our inclusion criteria (Figure 1).
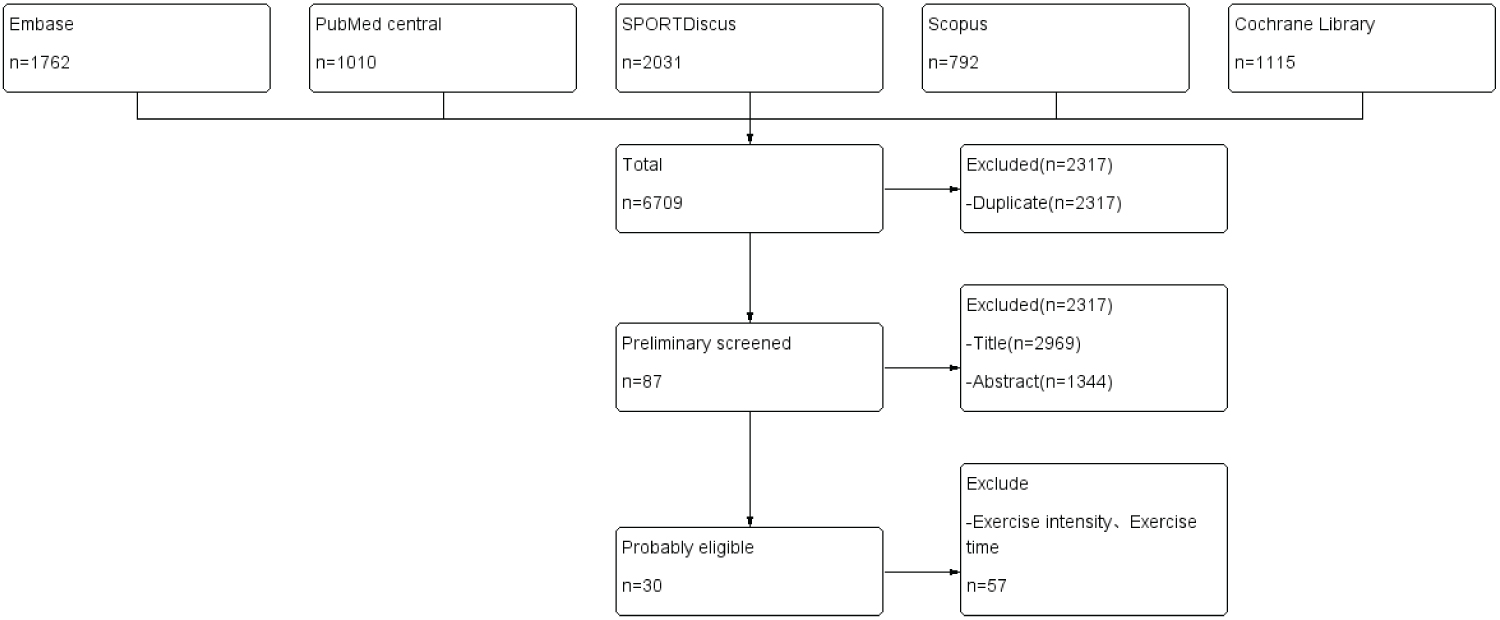 Figure 1: The search strategy identified 6709 articles from electronic databases and an additional 3 articles from previous relevant META studies were found manually on PubMed. A total of 2317 duplicate publications were removed, 2969 articles were screened out in the title, and 1344 were excluded after abstract screening. Of the remaining 87 articles, 30 met our inclusion criteria.
View Figure 1
Figure 1: The search strategy identified 6709 articles from electronic databases and an additional 3 articles from previous relevant META studies were found manually on PubMed. A total of 2317 duplicate publications were removed, 2969 articles were screened out in the title, and 1344 were excluded after abstract screening. Of the remaining 87 articles, 30 met our inclusion criteria.
View Figure 1
1973 subjects were included in the meta-analysis. The intervention protocol is summarized. The most widely used HIIT protocol consisted of alternating between 4 minutes of high intensity and 3 minutes of recovery. Other HIIT protocols were used for short periods of time (10 seconds to 1 minute) at high intensity. The duration of the interventions was generally more than two weeks. The frequency of all interventions is more than 2 days per week. (Data provided in the Annex).
A summary of the overall judgment for all seven domains of bias is presented in Figure 2. All included studies showed a "low" or unknown risk of bias in the areas of allocation concealment and completeness of outcome data. One study showed a high risk of bias arising from randomized sequences, mainly due to its own mention of the absence of blinded selection [27]. Six studies showed a "high" risk of blinding bias for investigators and subjects, mainly due to explicitly informing subjects of all relevant selection requirements [28-31]. Two studies showed a high risk of blinded evaluation of study outcomes [29,32]. Three studies showed a high risk of selective reporting of study results due to high dropout rates [29,33,34]. Two studies showed high risk for other sources because of drug use during participation [30,31].
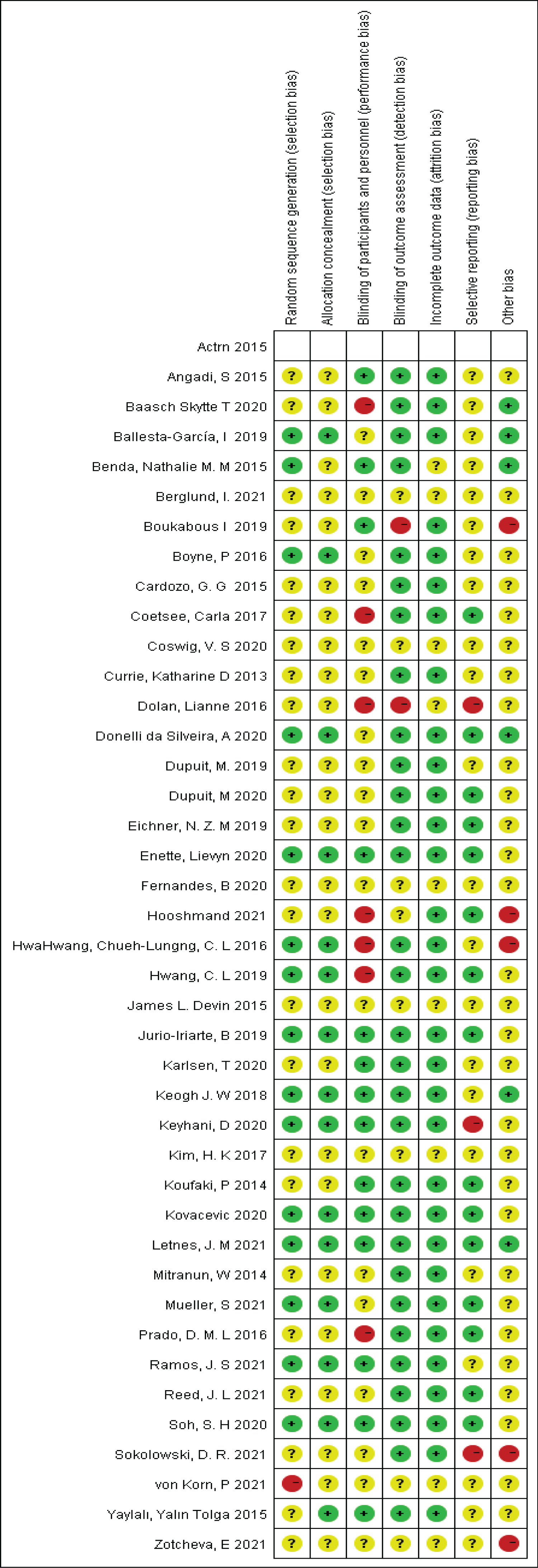 Figure 2: A summary of the overall judgment for all seven domains of bias is presented in Figure 2.
View Figure 2
Figure 2: A summary of the overall judgment for all seven domains of bias is presented in Figure 2.
View Figure 2
VO 2 max was significantly higher in older adults after HIIT intervention compared to controls (WMD = 2.97, 95% CI: 2.39-3.56, p < 0.001). Also, HIIT improved VO 2 peak to a greater extent than MICT (HIIT vs. MICT: WMD = 1.80, 95% CI: 1.25-2.35, p < 0.001).
Table 1 shows the results of subgroup analyses of VO 2 peak measures for eight subcategories: Training period, duration, frequency, presence or absence of disease, intensity, number of repetitions and sets per group, training time per repetition, and intergroup interval. In the training cycle subgroup, < 12 weeks of training (WMD = 3.59, 95% confidence interval 3.34, 3.85; I 2 = 77.2%, q = 48.26, df = 11, p < 0.001) were associated with a higher number of training cycles (WMD = 2.51, 95% confidence interval 2.06-2.95; I 2 = 87%, q = 104.15, df = 14, p < 0.001) produced a larger VO 2 peak effect. In the training frequency subgroup, the effect of 2, 3 and 4 training sessions per week on VO 2 peak was greater in older adults, with mean WMDs of 2.44 (twice), 4.46 (three times) and 2.33 (four times), respectively. The training intervention time subgroups were 20 min (WMD = 3.57, 95% confidence interval 0.35-6.79; I 2 = 0%, q = 0.38, df = 1, p < 0.001), 30 min (WMD = 3.36, 95% confidence interval 3.12, 3.61; I 2 = 76%, q = 127.62, df = 30, p < 0.001), 40 min training (WMD = 3.22, 95% confidence interval 2.71-3.74; I 2 = 80%, q = 25.02, df = 5, p < 0.001) produced a larger VO 2 peak effect. Sick patients had a larger effect on VO 2 peaks in older adults compared to healthy subjects, with mean WMDs of 3.85 and 2.47, respectively. In the training intensity subgroup, training intensity ≥ 80% VO 2 peaks and training intensity < 80% VO 2 peaks had a larger effect on VO 2 peaks in older adults, with mean WMDs of 3.23 (≥ 80% VO 2 peaks) and 4.47 (< 80% VO 2 peaks), respectively. The mean WMD was 3.25 (95% CI 2.73, 3.78; I 2 = 88%, q = 24.71, df = 3, p < 0.001), 2.95 (95% CI 2.67, 3.24; I 2 = 70%, q = 94.38, df = 28, p < 0.001), and 2.95 (95% CI 2.67, 3.24; I = 70%, q = 94.38, df = 28, p < 0.001), respectively, for each group with more than 3, 4, and 4 replicates. 4.51 (95% CI 4.04, 4.98; I 2 = 0.0%, q = 3.39, df = 4, p < 0.001). Repetition training time ≤ 60S subgroup (WMD = 3.44, 95% confidence interval 1.66, 5.22). The repetition training time > 60 s subgroup (WMD = 3.34, 95% confidence interval 3.12, 3.57; I 2 = 77%, q =148.97, df = 34, p < 0.001) produced a larger VO 2 peak effect. The ≤ 90 s rest period subgroup (WMD = 4.04, 95% confidence interval 2.00, 6.08; I 2 = 74.5%, q = 35.25, df = 9, p < 0.001) and the > 90 s subgroup (WMD = 3.34, 95% CI 3.11, 3.56; I 2 = 75%, q =1.97, df = 3, p < 0.001) had a greater impact. < 12 weeks of training cycle (WMD = 3.59), three training frequency (WMD = 4.46), 20 min per intervention (WMD = 3.57), < 80% intensity VO 2 peak (WMD = 4.47), > 4 repetitions (WMD = 4.51), > 60s per training session (WMD = 3.34), ≤ - 90s rest time (WMD = 4.04) had the greatest effect on the VO 2 peak.
Table 1: Shows the results of subgroup analyses of VO2 peak measures for eight subcategories. View Table 1
Nine HRs (WMD = 1.90, 95% CI: 0.07-3.74) (HIIT vs. MICT: WMD = 2.68, 95% CI: 0.84-4.53, p < 0.004), seven VE/VO 2 (WMD = -0.40, 95% CI: -1.88-1.07) compared with the control group and the MICT group (HIIT vs. MICT: WMD =1.04, 95% CI: 0.66-1.42, p < 0.0001) showed significant differences. Three OUES (WMD = 0.31, 95% CI: 0.24-0.37), six RER (WMD = -0.01, 95% CI: -0.07-0.04), and four FFM (WMD = 0.16, 95% CI: -0.95-1.28) showed significant differences compared to controls.
A total of 16 studies showed a significant reduction in systolic blood pressure (WMD = -2.59, 95% CI: -5.06- -0.12) and diastolic blood pressure (WMD = -1.40, 95% CI: -3.46-0.66) after HIIT in the elderly (p < 0.04), although the difference was not statistically significant (P > 0.05).
The decline was significantly better for greater than or equal to 12 weeks (WMD = -3.73, 95% CI: -5.93- -1.54) than for less than 12 weeks (WMD = -2.54, 95% CI: -3.52- -1.56), greater than 6 times (WMD = 0.90, 95% CI: -2.39-4.19), and less than 6 times (WMD = -2.87, 95% CI: -3.90, -1.85).
Seven studies compared older adults with significant upregulation of PPO (WMD = 30.17, 95% CI -29.49-30.86; I 2 = 0.0%, q = 2.51, df = 7, p = 0.000) after HIIT intervention. Also, HIIT showed greater improvement in PPO compared to MICT (HIIT vs. MICT: WMD = 16.54, 95% CI: 15.77-17.30, p < 0.001). 5 studies comparing the change in 6MWT were significantly higher in the HIIT group than in the control group (WMD = 51.60, 95% CI = 29.98- 73.22; I 2 = 0.0%, q = 1.11, df = 3, p < 0.00001). Four studies described Time and go TEST changes (standardized mean difference = -0.62, 95% CI: -1.09- -0.14; I 2 = 0.0%, q = 0.23, df = 2)., 2 studies comparing METs (standardized mean difference = -0.62, 95% CI: -1.09- -0.14; I 2 = 0.0%, q = 2.68, df = 4).
Maximal oxygen consumption (VO 2 max) is the amount of oxygen that the body can take in when exercising at maximum intensity and when the systems are at their highest state. It is an important indicator of the body's aerobic capacity and is negatively associated with the development of cardiovascular disease and different types of cancer. Previous studies have concluded that MICT has a greater beneficial effect on younger subjects (individuals with strong cardiorespiratory fitness) VO 2 max, while HIIT has a more pronounced beneficial effect on subjects with poorer cardiorespiratory fitness [21,35]. The present study showed that HIIT significantly upregulated VO 2 peak in older adults, increasing VO 2 peak by 3 and 1.8 mL/kg/min compared to the control group (WMD = 3) and MICT group (WMD = 1.8), respectively. And this study found a higher VO 2 peak effect for 3 sessions/week (WMD = 4.46) than for 2 sessions/week training (WMD = 2.44) and 4 sessions/week training (WMD = 2.33) by subgroup analysis. This is consistent with the more significant improvement in VO 2 peak with 3 HIIT sessions per week in patients with vascular dysfunction [36] study results. Notably we demonstrate for the first time that HIIT improves VO 2 max faster in older patients with lower levels of cardiorespiratory fitness and pharmacological interventions compared to healthy individuals, again demonstrating that HIIT may have a better impact on individuals with lower basal metabolic rates. Interestingly, unlike previous META analyses on older adults, this study showed a greater benefit of training for less than 12 weeks compared to training for more than 12 weeks to improve VO 2 max. This is not consistent with a previous meta-analysis conducted in an overweight/obese population. We speculate that this may be due to the length of the experiment, which resulted in a lack of timely adjustment of exercise intensity after the rise in subject cardiorespiratory fitness, and possibly due to the increased aging of subjects due to the length of some of the experimental interventions (5 years), with an increase in HIIT improvement after removing the 5-year study (WMD = 2.93). Even so, the present study found HIIT to be effective in mitigating the decrease in VO 2 max associated with aging. In addition, we also found better results with intensities less than 80% VO 2 peak and a training time of less than 60 seconds per session, which may be closer to the original intention of HIIT setting, which is to favor exercises below 40s and to ensure that the body is in anaerobic energy supply. The hypoxemia treatment protocol used in this study suggested that incorporating a supervised treatment protocol (i.e., 8 × ≤ 60s HIIT at < 80% VO 2 peak, ≤ 90s recovery, 3 times per week for less than 20 min for less than 12 weeks) was effective in improving VO 2 peak. Although this differs from previous studies that mentioned that it seems that longer exercise duration and more exercise per week are better for cardiorespiratory health, considering that the latest study mentioned that excessive exercise may lead to coronary calcification and plaque progression in subjects with an average of 53.6 years, it suggests that moderate exercise is best for patients with a poor exercise base. Notably, the American College of Sports Medicine (ACSM) recommends 20 minutes of vigorous exercise 3 days per week [37,38], which appears to be the same as the results we obtained. Furthermore, the American College of Sports Medicine State College study showed that older adults should accumulate 150-300 minutes (30-60 min/d × 5 times/week) of moderate-intensity aerobic exercise per week, yet our results may explain that HIIT achieves better results in a shorter period of time, especially considering that the safety concerns associated with HIT are unfounded [39-41]. This provides valuable information for those involved in the design and implementation of HIIT programs. META analysis demonstrates that HIIT improves cardiac function in healthy older adults [42,43].
It is worth noting that VO 2 max is a composite indicator, which suggests the need for other aerobic capacity indicators to complement the effect on aerobic specific function. Maximum heart rate refers to the heart rate that occurs when the body is performing extreme exercise and is able to withstand a maximum load, and an increase in maximum heart rate within a certain range implies an increase in oxygen transported. Previous studies have shown a similar increase in peak VO 2 and OUES [44]. The physiological mechanism reflected in OUES is the development of metabolic acidosis [45], metabolic acidosis is controlled by the distribution of blood to skeletal muscle and by the effect of lung perfusion leading to increased physiological dead space. The results of previous HIIT studies on ventilation efficiency showed that exercise training improvements significantly reduced VE/VCO 2 slope levels [46]. This provides additional evidence that HIIT improves cardiopulmonary function, and the 6min walk test is the most commonly used measure of endurance walking capacity, and improving 6MWT is a valuable target for older adults with severely impaired function (Li, et al., 2019). It is suggested that HIIT may be a significant effect on oxygen transport, oxygen utilization efficiency, carbon dioxide metabolism and other aerobic indicators [44,47].
Interestingly, the present study found a significant effect of HIIT only on SBP, while no superior effect of HIIT over MICT was observed for SBP, DBP. However, previous systems conducted using meta-analysis also had controversial results when assessing the effect of HIIT versus MICT on BP. The present study speculates that previous studies suggest that cardiac systolic function is associated with greater improvement in aerobic adaptations and that HIIT may be effective in inducing left ventricular remodeling in older adults while improving systolic function to a greater extent, but not diastolic function of the heart [48]. This is consistent with a significant reduction in systolic blood pressure after both HIITs and is not affected by gender [33,49]. The present study suggests that longer duration of intervention and lower frequency of exercise are more effective. Regarding the reduction in blood pressure may be related to the reduction in catecholamine levels and systemic vascular resistance. The physiological mechanism of blood pressure improvement related to the renin-angiotensin system may be that exercise also improves endothelial function, improves autonomic regulation, and reduces vascular resistance [50]. This is the same result we obtained [51]. Unfortunately, the present study did not find subgroup analyses confirming a greater effect of HIIT on participants with high blood pressure at the beginning of the study compared to individuals with hypotension across groups [52]. This is not consistent with previous findings of a reduced SBP response in older adults with controlled hypertension after HIIT [53]. This may be related to the fact that some participants did not discontinue their medications during the intervention.
The HIIT-induced TUG time was reduced by 1.2 seconds in the time up and go test and by 3.86 seconds in the chair test. The Metabolic Equivalent (MET), which indicates the relative energy metabolic level and exercise intensity, also increased significantly. Sella, et al. [54] implemented a longer intervention than the current study (12 weeks) and used a combined aerobic and endurance training program (aerobic-three times/week with interval training), with a significant increase in PPO after a gradual increase from 60%-75% PPO to 110% PPO. Power in practice, the heavier the load, the lower the speed, and the lighter the load, the higher the speed. This is because the maximum power output is located in the middle of the force-velocity curve [55,56]. The rate of muscle shortening in the human body is limited, so to improve PPO, an increase in strength must be achieved. It is interesting to note that HIIT has a superior effect on PPO than MICT, which, combined with the improvement in both Time up and go, METS and chair tests, may suggest that HIIT has a significant enhancement effect on neural activity, muscle area and muscle strength, which is also consistent with previous studies. Unfortunately, due to the small number of studies on muscle area, relevant metrics were not included in this study. Despite these limitations, based on the best applicability to practitioners and clinicians, this study created a possible combination of HIIT subclasses. Although the effects of these interventions on risk factors may not be statistically significant, such changes can produce important health outcomes if participants are transferred to healthy older adults [57]. Following exercise reporting guidelines can help address the lack of detail in the reporting of exercise interventions and improve the translation of exercise dose responses into clinical exercise prescriptions [37,58]. This review found no serious adverse events associated with reported exercise interventions.
HIIT may be an effective means of improving cardiorespiratory fitness and exercise capacity in older adults. However, compared to MICT, HIIT significantly improved changes in VO2 max, VE/VCO2, PPO and HEART, suggesting that it may increase muscle strength and oxygen utilization (which is similar to resistance exercise). Unfortunately, this paper does not specifically examine the relationship between the utility of comparing such changes to each other, which needs to be explored in further net META analyses.